 Owner income$1.4M
Owner income$1.4MHow Much Can A Rheumatoid Arthritis Clinic Owner Make With $232M Revenue?

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Owner income$1.4M  Net margin48%–75%
Net margin48%–75% Revenue for target pay$2.3M
Revenue for target pay$2.3M Business difficultyMedium
Business difficultyMedium


Key Takeaways
- Year 1 infusion volume is the biggest revenue lever.
- Payer mix and denials determine net cash collected.
- Fixed overhead sets the floor before owner pay.
- Reserves are critical because cash gets trapped.
Owner income$1.4MNet margin48%–75%Revenue for target pay$2.3MBusiness difficultyMediumWant to test your RA clinic owner pay?
Owner income calculator
Estimate owner take-home and target-pay gap from monthly revenue, gross margin, staffing cost, overhead, reserves, and target pay.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
Want to check owner income in the Rheumatoid Arthritis Treatment Clinic model?
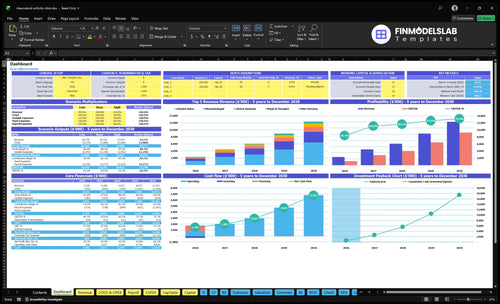
Screenshot shows revenue, margin, costs, reserves, and owner take-home assumptions in Rheumatoid Arthritis Treatment Clinic Financial Model Template. It also maps $232M to $1,233M revenue, $912k to $922M EBITDA, and $285k startup capex. Open it to test scenarios.
Owner-income model highlights
- Owner take-home outputs
- Revenue and EBITDA charts
- Scenario tests on inputs
How much can a rheumatoid arthritis clinic owner take home after expenses?
A Rheumatoid Arthritis Treatment Clinic owner can take home the included $280k owner-clinician salary, plus a possible draw from $912k EBITDA after taxes, debt service, reserves, and reinvestment; for cost context, see What Are Operating Costs For Rheumatoid Arthritis Treatment Clinic?. Here’s the quick math: $912k EBITDA on $232M revenue equals a 0.39% EBITDA margin, so cash discipline matters.
Take-home view
- $280k salary is already in payroll
- $912k EBITDA funds any extra draw
- Pay taxes before owner distributions
- Hold reserves for clinic cash flow
Cost guardrails
- $249k/month listed fixed overhead
- $620k/year listed payroll
- 21% Year 1 variable costs
- Model added hired-clinician payroll separately
How many patients does a rheumatoid arthritis clinic need to pay the owner?
The clinic can’t be sized by patient count alone; it needs about 366 encounters a month to cover fixed payroll and overhead, and about 486 encounters a month if the owner also wants $300k a year. At the Year 1 model, monthly revenue is about $1.932M from roughly 729 treatment encounters, or about $265 blended revenue per encounter.
Break-even math
- $766k fixed payroll and overhead
- 79% contribution margin
- $969k monthly collections to break even
- About 366 encounters per month
Owner pay target
- Add $300k annual distribution
- Needed collections rise to $1.286M monthly
- That is about 486 encounters per month
- Payer mix and no-shows change the math
Does in-office infusion increase rheumatoid arthritis clinic owner income?
Yes, it can boost owner income for a Rheumatoid Arthritis Treatment Clinic, but only if reimbursement, drug-cost timing, authorization work, and chair use all hold up. In the model, Year 1 infusion revenue is $96k per month, nearly half of total monthly revenue, and Year 5 infusion revenue reaches $5355k per month. The catch is cash: specialty biologic drug inventory is modeled at 85% of revenue in Year 1 and 75% in Year 5, so higher acquisition costs or delayed collections can drain cash fast.
Revenue drivers
- $96k monthly in Year 1
- Nearly half of monthly revenue
- $5355k monthly in Year 5
- Model the infusion line separately
Cash risk points
- 85% inventory in Year 1
- 75% inventory in Year 5
- Delayed collections can squeeze cash
- Authorization delays slow chair use
What drives RA clinic owner income most?
1
$2.3MProvider Capacity
Year 1 revenue is $2.318M at 65% rheumatologist capacity and 50% infusion nurse capacity, so filled slots drive the fastest lift in owner cash.
2
$1.2KInfusion Economics
Infusion visits price at $1,200 in Year 1, so keeping the infusion suite busy can add more EBITDA than low-ticket care.
3
21%Margin Rate
COGS and variable spend run about 21% in Year 1, so tighter billing, claims, and supply control drops straight to take-home.
4
$620KPayroll Load
Year 1 payroll is about $620K, so staffing the right mix keeps growth from getting eaten by labor.
5
$24.9K/moFixed Overhead
Fixed overhead is about $24.9K per month, so lease, insurance, IT, and admin discipline protect reserves and distributions.
6
43.9%Owner Payout
With a 43.89% IRR and one-month payback, the owner can balance draw, reserves, and reinvestment without choking growth.
Rheumatoid Arthritis Treatment Clinic Core Six Income Drivers
Provider Capacity And Patient Volume
Provider Capacity And Visit Volume
When more scheduled visits are actually completed, collections rise fast because most overhead does not move line by line. At Year 1 levels, 208 monthly rheumatology visits at $250 each and 80 monthly infusion treatments at $1,200 each produce about $148,000 per month before overhead and staffing pressure.
This driver includes show rate, follow-up cadence, new-patient access, and schedule gaps. No-shows and empty slots cut revenue right away, while moving capacity toward Year 5 levels can lift income materially. The catch: volume only helps if billing, staffing, and clinical quality keep pace, or owner pay can get squeezed by rework and delays.
Track Filled Slots, Not Just Open Slots
Here’s the quick math: 208 visits × $250 = $52,000 and 80 treatments × $1,200 = $96,000. So the real target is completed care, not booked calendar time. Track completed visits, infusion chair use, no-show rate, and time from referral to first visit, because those are the levers that move cash into the business.
Use a weekly schedule review to spot gaps, late cancels, and slow follow-up. If access is tight or the calendar is fragmented, revenue softens even when demand is there. One clean rule: every empty slot is lost collection, unless the team has a fast way to refill it and bill it cleanly.
- Measure completed visits, not bookings.
- Watch no-shows and open gaps.
- Protect infusion chair and nurse time.
- Keep billing and staffing aligned.
1
Payer Mix And Net Collections
Payer Mix And Net Collections
Owner pay follows cash collected, not billed charges. With prices from $75 clinical assistant encounters to $1,200 Year 1 infusion treatments, payer mix, Medicare share, prior authorization, denials, and billing speed can move take-home income fast. Billing and claims fees are modeled at 30% of revenue in Years 1–2, then 25% by Year 5.
Test Reimbursement Before You Add Infusion
Track payer mix, denial rate, days in A/R (days to collect cash), and net collections per visit. If a service collects $100, a 30% billing fee leaves $70 before other clinic costs. Local reimbursement assumptions must be tested before hiring or expanding infusion. Slow auth or weak contracts can delay distributions even when visit volume looks strong.
- Medicare share and contract rates
- Authorization turnaround time
- Denial rate and appeal lag
- Days in A/R and posting speed
2
In-Office Infusion Economics
Infusion Revenue and Cash Flow
Infusion is the biggest revenue lever here, but it’s also the biggest cash-flow risk. Year 1 assumes $96k per month from 2 infusion nurses at 50% capacity; by Year 5, the model rises to $5,355k per month with 5 nurses at 85% capacity. Owner pay only grows if that volume turns into clean collections, not just billed charges.
The pressure point is the drug cash tied up before payment clears. Biologic inventory is modeled at 85% of revenue in Year 1 and 75% in Year 5. So if authorizations slow, chairs sit empty, or nursing coverage breaks, revenue drops fast while inventory and labor still hit cash. That can shrink distributions even when the clinic looks busy.
Track Drug Cash and Chair Use
Measure capacity by nurse, chair utilization, authorization lag, denial rate, and days in inventory. These inputs tell you if infusion is producing spendable profit or just tying up cash. Model each payer separately, since payer spread changes both margin and the speed of collections.
Do not add chairs or nurses until monthly collections beat drug purchases and staffing cost. If authorizations slip, the clinic can show strong revenue on paper and still run short on cash for owner draws. One clean metric beats a dozen hopeful ones.
3
Staffing Efficiency And Clinical Labor
Staffing Efficiency and Clinical Labor
If payroll does not turn into completed visits and clean claims, it turns into dead weight. Listed payroll rises from $620k in Year 1 to $730k in Years 3 and 4, then $775k in Year 5, so the clinic has to keep schedules full across clinical and front-office staff.
The key test is simple: paid labor must produce billable work fast enough to support owner distributions. Roles include a lead rheumatologist, clinic director, receptionists, care coordinator, and billing manager, plus rheumatologists, infusion nurses, physical therapists, occupational therapists, and clinical assistants. If added clinician payroll is missing from the wage schedule, add it before sizing profit.
Track Labor per Billable Visit
Measure completed visits per staffed hour, claim clean rate, no-shows, and the share of payroll tied to direct care versus admin. Those inputs show whether labor is supporting revenue or just adding fixed cost.
- Track visits by role each week
- Separate direct care and admin payroll
- Log claim errors and resubmits
- Add missing clinician wages first
When volume softens, cut schedule gaps before cutting core clinical coverage. When billing slows, cash gets trapped even if visits happened, and owner pay comes later.
4
Fixed Overhead And Operating Costs
Fixed Overhead Floor
Fixed overhead is the monthly bill the clinic pays before the owner sees any pay. Here, that floor is $249k per month, including $12k lease, $65k malpractice, $22k EHR and IT, $18k utilities, $900 supplies, and $15k licensing. These costs do not fall much when visit volume dips, so they set the minimum cash the clinic must collect each month.
One clean rule: if collections do not clear the $249k floor, owner income gets squeezed fast. Keep drug costs and clinical supplies separate, because mixing them into overhead will hide the real margin. In Year 1, the extra load from 50% marketing and 30% billing also cuts into cash left for salary, reserves, and distributions.
Track the Floor, Then Price for It
Measure monthly collections, fixed overhead, and variable billing and marketing costs in the same view. The key test is simple: do net collections after direct clinical costs still clear the $249k floor and leave room for owner pay? If not, the clinic may be busy but still not profitable enough to pay the owner well. p>
Control the big lines first: lease, malpractice, EHR and IT, utilities, licensing, and staff support. Then watch whether higher visit volume improves cash or just raises billing and marketing spend. If collections lag behind visits, tighten denial follow-up, reduce wasted seats, and forecast cash weekly so the owner can see when distributions are safe.
5
Owner Role, Reserves, And Distributions
Owner Salary, Reserves, And Draws
Owner take-home here comes from $280k lead salary plus any distribution from EBITDA. The model shows Year 1 EBITDA of about $912k before taxes, debt service, reserves, and reinvestment, so cash pay can be much lower than profit on paper. EBITDA is not spendable owner income.
What matters is cash left after infusion inventory, delayed collections, and the cash reserve the clinic keeps on hand. The model’s Year 5 EBITDA is listed at $922M, but the real question is how much stays in the bank after working capital and debt service.
Set A Distribution Floor First
Track three inputs every month: salary, cash reserve target, and free cash after inventory and collections. If collections lag or infusion stock ties up cash, keep distributions low even when EBITDA looks strong. That keeps the owner paid without starving the clinic.
- Pay salary before draws.
- Hold a reserve for delays.
- Review cash after billing.
- Limit draws during inventory spikes.
6
Compare lean, base, and high RA clinic income scenarios
Owner income scenarios
Owner income moves with service mix, staffing, and infusion volume. The low case keeps the clinic lean; the high case tracks toward Year 5 scale.
| Scenario | Low CaseDownside | Base CaseBase | High CaseUpside |
|---|---|---|---|
| Launch model | This is the conservative earnings path if the clinic stays consult-heavy and infusion volume remains modest. | This is the modeled middle path using the Year 1 operating plan. | This is the stronger earnings path if the clinic scales toward the Year 5 operating plan. |
| Typical setup | Keeps infusion use low, runs tighter staffing, and stays below the Year 1 capacity buildout while protecting cash flow. | Runs with 2 rheumatologists, 2 infusion nurses, 1 physical therapist, 1 occupational therapist, and 2 clinical assistants, with Year 1 revenue of $2.318 million and EBITDA of $1.115 million. | Moves closer to Year 5 scale with 6 rheumatologists, 5 infusion nurses, 4 physical therapists, 2 occupational therapists, and 6 clinical assistants, with Year 5 revenue of $12.327 million and EBITDA of $9.286 million. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $180,000 - $240,000Lower income | $280,000Base income | $400,000 - $600,000Higher income |
| Best fit | Use this to stress-test a slower start and thinner owner take-home. | Use this as the main plan for a stable opening year. | Use this to test upside if demand and staffing both scale cleanly. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Rheumatoid Arthritis Treatment Clinic Porter's Five Forces Analysis
- Rheumatoid Arthritis Treatment Clinic BCG Matrix
- Rheumatoid Arthritis Treatment Clinic Business Model Canvas
- What Are The Five KPI Metrics For Rheumatoid Arthritis Treatment Clinic?
- Rheumatoid Arthritis Treatment Clinic Business Plan Template in Pre-Written Word
- How Increase Profits Rheumatoid Arthritis Treatment Clinic?
- What Are Operating Costs For Rheumatoid Arthritis Treatment Clinic?
- Rheumatoid Arthritis Clinic Startup Costs: $305K CAPEX Plan
- Rheumatoid Arthritis Clinic Financial Model Template in Excel
- How To Open A Rheumatoid Arthritis Treatment Clinic In 6–9 Months
- How To Write A Business Plan For Rheumatoid Arthritis Treatment Clinic?
- Rheumatoid Arthritis Treatment Clinic Marketing Mix
- Rheumatoid Arthritis Treatment Clinic Marketing Plan
- Rheumatoid Arthritis Treatment Clinic Business Proposal
- Rheumatoid Arthritis Treatment Clinic PESTEL Analysis
- Rheumatoid Arthritis Clinic Pitch Deck Example Editable PPTX
- Rheumatoid Arthritis Treatment Clinic Business SWOT Analysis
- Rheumatoid Arthritis Treatment Clinic Value Proposition Canvas
Frequently Asked Questions
In the provided first-year model, the clinic produces about $232M in revenue and $912k in EBITDA before taxes, debt, reserves, and reinvestment That includes listed payroll of $620k and fixed overhead of $249k per month Owner pay depends on whether the owner takes the $280k lead rheumatologist salary and how much cash the business keeps