 Owner income$0-$523k
Owner income$0-$523kHow Much Does a Speech Therapy Clinic Owner Make? $0 to $214M

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$0-$523k  Net margin-67% to 31%
Net margin-67% to 31% Revenue for target pay$521k
Revenue for target pay$521k Business difficultyHard
Business difficultyHard


You’re not comparing employee SLP wages here you’re modeling clinic owner economics This five-year view covers $521k to $3747k in monthly collected revenue, payroll, rent, billing costs, marketing, reserves, and potential owner pay before taxes, debt, and personal living costs
Owner income$0-$523kNet margin-67% to 31%Revenue for target pay$521kBusiness difficultyHardWant to test your clinic owner income?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate, not guaranteed salary, tax advice, or owner distribution advice. Actual owner pay depends on collections, payer mix, staffing, debt, and reserve needs.
Want the full Speech Therapy Clinic forecast and owner income view?
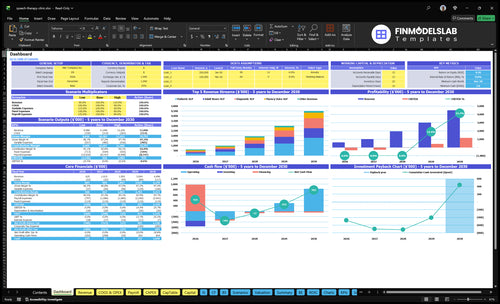
The screenshot shows revenue, margin, costs, reserves, and owner take-home assumptions; open the Speech Therapy Clinic Financial Model Template for the full forecast.
Owner-income model highlights
- Collected revenue: $521k–$3,747k
- EBITDA: -$1,032k to $214M
- Margin: -165% to 475%
- Low/base/high scenarios
Is solo SLP private practice income better than hiring employees?
Solo Speech Therapy Clinic income is usually simpler and safer at the start, because the owner keeps more of each collected session. Hiring employees can lift total income, but only if utilization (filled sessions) and collections cover payroll before owner pay. With this model, 6 clinical FTEs and $550k payroll in Year 1 can still create a loss, while 22 clinical FTEs support about 2,205 collected sessions per month and $214M EBITDA by Year 5.
Why solo can pay better
- Owner keeps more per session
- No payroll drag at start
- Fewer scheduling gaps to cover
- Income is easier to predict
When hiring helps
- Only if sessions stay full
- Only if collections stay tight
- Supervision and billing must run well
- Payroll must beat owner draw
Can a speech therapy clinic owner make six figures?
Yes, a Speech Therapy Clinic owner can make six figures, but not automatically; What Is The Main Goal Of Your Speech Therapy Clinic? should separate owner-operator pay from clinic profit. In this model, the Lead SLP Clinical Director role is budgeted at $110k/year, but Year 1 EBITDA is -$1.032M, so owner distributions are not available yet.
Six-Figure Path
- Earn $110k as clinical director
- Separate salary from distributions
- Pass collected-visit break-even
- Improve therapist utilization
Profit Reality
- Year 1 EBITDA: -$1.032M
- No Year 1 distributions
- Year 2 EBITDA: ~$828k
- Year 2 revenue: $101M
What profit margin can a speech therapy clinic make?
A Speech Therapy Clinic can show strong margin once paid visits grow faster than clinician payroll and fixed overhead, but early owner profit can still be thin. In this model, direct supply and transaction costs are 35% in Year 1 and fall to 26% by Year 5, while EBITDA margin moves from -165% in Year 1 to 82% in Year 2, 264% in Year 3, and 475% in Year 5. For launch cost context, see How Much Does It Cost To Open And Launch Your Speech Therapy Clinic?
Margin drivers
- 35% direct cost in Year 1
- 26% direct cost by Year 5
- Paid visits must outgrow payroll
- Gross margin lifts with utilization
Take-home risks
- No-shows cut revenue fast
- Denials delay cash and profit
- Rent and admin add pressure
- Documentation time hits owner take-home
Want the six drivers that decide owner income?
1
$144-$170Collected Rate
This is the cash you keep per session, and small rate gains scale across hundreds to thousands of visits.
2
361-2.2KVisit Volume
More monthly collected sessions spread the fixed base and drive the move from loss to profit.
3
8.5-28 FTEStaffing Margin
Payroll rises as the clinic adds clinicians, so take-home depends on adding sessions faster than staff.
4
Cash GapPayer Mix
Denials and slow pay can turn booked work into delayed cash, and billed charges are not the same as collections.
5
$9.9K/moFixed Overhead
Rent, software, insurance, and admin set the monthly floor the clinic must clear before owner income turns positive.
6
1 FTEOwner Role
A full-time owner clinician can pull in revenue directly, but a heavier management role usually means more hired labor.
Speech Therapy Clinic Core Six Income Drivers
Collected Rate Per Session
Collected Rate Per Session
Collected rate per session is the cash you actually keep per completed visit, not the sticker price. In Year 1, the model shows $120 pediatric sessions up to $350 diagnostic sessions, with about $144 collected per visit after mix and utilization. At 361 collected visits a month, that is about $52,000 in monthly revenue before costs.
This driver moves owner income fast because payer contracts, patient responsibility, denials, and write-offs all change what lands in cash. By Year 5, the range rises to $140 to $390, with about $170 collected per visit. The same visit count would lift revenue by about 18%, and every extra collected dollar adds to contribution after variable costs.
Improve collected dollars per session
Track collected rate by service line, payer, and visit type. The key formula is cash collected ÷ completed visits. If collections slip, look first at denials, patient balances, and contract rates, not just schedule fill. A small drop across many visits can wipe out owner pay even when the calendar looks full.
Use weekly reports to compare billed charges, collected cash, and write-offs. Then test which mix brings the best net rate: pediatric therapy, diagnostic work, or other session types. The goal is simple: keep the collected amount per visit moving up while protecting margin and cash flow.
1
Visit Volume And Utilization
Collected Visit Volume
Volume means collected visits, not inquiries or booked slots. Year 1 runs at 55% to 70% capacity by service line and reaches about 361 collected visits per month; Year 5 rises to 80% to 90% and about 2,205 collected visits per month. That gap matters because payroll and overhead get paid before owner pay, so low utilization can leave the clinic busy on paper but short on cash.
Here’s the quick math: fixed overhead is $99k per month, and Year 1 break-even is about 427 collected sessions per month versus 361 modeled. Cancellations, no-shows, school-year seasonality, and clinician availability can swing revenue fast. One clean line: if collected visits dip, owner draw usually drops first.
Raise Visit Completion
Track scheduled visits, collected visits, cancellations, no-shows, and filled openings by clinician and service line. The useful rate is completed visits divided by available capacity, not booked slots. If a therapist looks 70% full but no-shows are high, real output is lower, and that gap hits margin because the payroll cost is already committed.
- Watch completion by therapist.
- Backfill same-day openings.
- Measure seasonality by month.
- Keep a waitlist ready.
At about $144 collected revenue per visit in Year 1, every 10 extra collected visits add roughly $1,440 before variable costs. Protect school-year demand, reduce no-shows, and staff to real fill rates, not hopeful schedules. What this estimate hides: weak collections or overstaffing can still erase the gain.
2
Clinician Staffing Margin
Clinician Staffing Margin
Clinician staffing margin is the gap between collected visit revenue and the full cost of the team delivering care. In this model, annual wages rise from $550k in Year 1 to $196M in Year 5, with roles like $110k for the Lead SLP Clinical Director and $85k to $92k for therapy specialists. That makes payroll the main pressure on owner profit and pay.
The real cost is higher than salary alone. Employee models add payroll taxes, benefits, supervision, and non-billable time, so margin depends on utilization per clinician, meaning how many booked hours turn into collected visits. One clean rule: if a clinician is paid but not producing enough billed sessions, the owner still eats the cost.
Track Billable Time Per Clinician
Measure collected visits per clinician, not just scheduled hours or headcount. Compare each service line against its wage load: Pediatric SLPs at $85k, Adult Neuro SLPs at $90k, Fluency Voice SLPs at $88k, and Diagnostic SLPs at $92k. The goal is simple: more collected sessions per paid hour.
Test staffing mix before adding people. If the clinic can use contractor or assistant models where allowed, margin risk can change fast, but only if quality and supervision stay tight. Watch non-billable time, no-shows, and cancellations together, because those three items decide whether payroll turns into profit or just payroll.
3
Payer Mix, Denials, And Collections
Payer Mix And Collections
Payer mix is the split across private insurance, Medicaid, self-pay, schools, and contracts. It changes collected rate per visit, payment timing, and billing work, so cash can lag even when revenue looks fine. The model should use collections, not billed charges. At 1,000 visits a month, a mix that supports $170 per visit instead of $144 adds $26,000 in monthly cash.
Denials and slow patient balances hit owner take-home fast because payroll and fixed overhead are already locked in. Here’s the quick math: visits × collected rate per visit drives cash, not schedule volume. A small collection drop across 1,000+ monthly visits can erase distributions, especially when school contracts or Medicaid pay slower than self-pay. This is a planning sensitivity, not billing advice.
Track Collections By Payer
Break monthly results into private insurance, Medicaid, self-pay, schools, and contracts. Track billed amount, collected amount, denial rate, and patient balance aging for each group. If one payer starts paying slower, you’ll see the hit in cash flow before it shows up in revenue reports or owner draws.
Stress test the forecast with a lower collected rate per visit and slower payment timing. Keep visit volume the same, then see how much cash is left after fixed costs and payroll. If owner pay disappears under a modest collection change, the clinic needs tighter billing follow-up and cleaner payer rules.
- Track collected rate per visit.
- Watch denial rate by payer.
- Age patient balances monthly.
- Test school and contract timing.
4
Fixed Overhead And Operating Expenses
Fixed Overhead and Operating Expenses
Fixed overhead is the monthly cost floor the clinic must cover before owner pay. Here, modeled fixed expenses are $99k per month, including $5k rent, $12k liability insurance, $700 EHR software, and other set costs. That means profit stays tight until collected sessions rise enough to absorb payroll plus overhead.
Here’s the quick math: Year 1 break-even is about 427 collected sessions per month, but the model expects 361. That leaves a gap of 66 sessions before owner income starts to look safe. The risk is highest early, because payroll is already committed while volume is still thin.
Track the Cost Floor Weekly
Track collected sessions, not scheduled visits, against fixed spend every week. Use the monthly cost stack to spot drift in rent, insurance, software, utilities, and office items b efore it hits cash flow. If collections stay below 427 sessions, owner draw should stay conservative.
Watch the gap between expected volume and break-even volume. If session count slips, the fix is usually utilization, scheduling, or collections, not more overhead. Keep the cost floor lean so each extra collected visit drops more cash to profit and then to owner pay.
5
Owner Clinical Versus Management Role
Owner Clinical Role
If the owner fills the Lead SLP Clinical Director role, that work is not free. The model treats it as a $110k annual salary inside payroll, so owner pay is really salary plus any remaining profit. If the owner steps back and hires that role, distributions depend on what is left after payroll, overhead, and collections. One line matters: owner time changes the cost structure.
Here’s the quick math: treating clients can lift revenue, but it also pulls the owner away from management. That tradeoff only works if clinicians stay productive and collections are reliable. With $99k monthly fixed overhead and a Year 1 break-even near 427 collected sessions per month versus 361 modeled, the owner’s clinical time helps only if it closes the gap, not if it slows growth.
Track Salary Versus Distributions
Measure the owner role in two ways: salary value and profit draw. If the owner is in the clinic, track collected visits, collected revenue per visit, and non-billable admin time. If the owner is in management, track clinician utilization, denials, and cash collection timing. The real question is simple: does the owner’s time raise profit more than a hired clinical director would cost?
- Track collected visits per month.
- Watch utilization by clinician.
- Compare salary to added profit.
- Flag slow collections fast.
Test the switch only when the schedule is stable. If clinicians are productive and billing is tight, stepping into management can scale income by freeing the owner to build volume. If not, owner clinical work may protect cash short term, but it caps growth because every treatment hour taken by the owner is one less hour spent on team, payer, and referral management.
6
Compare lean, base, and mature owner income scenarios
Owner income scenarios
Owner income moves with session volume, collected rates, staffing, and fixed overhead. Early years stay tight, then break-even improves as calendars fill and capacity rises.
| Scenario | Low CaseLow case | Base CaseBase case | High CaseHigh case |
|---|---|---|---|
| Launch model | This is the weaker path where Year 1 volume and staffing keep owner income negative. | This is the modeled middle path using Year 3 volume, pricing, and staffing. | This is the stronger path where Year 5 volume and pricing lift owner income well above break-even. |
| Typical setup | The clinic runs on Year 1 assumptions: about 361 collected sessions a month, about $52k in monthly revenue, and payroll plus fixed overhead still outrun collections. | By Year 3, the clinic is around 1,056 collected sessions a month, about $193k in monthly revenue, and a larger therapist bench that pulls EBITDA close to break-even. | By Year 5, the clinic reaches about 2,205 collected sessions a month, roughly $375k in monthly revenue, and a bigger team with much better capacity use. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | -$350kLow income | -$3k to $0Base income | $1.15MHigh income |
| Best fit | Use this to stress-test a slow ramp, payer delays, or underfilled calendars. | Use this as the main planning case for staffing, cash, and lender talks. | Use this to test what full calendars and strong referrals can produce once the clinic is mature. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Speech Therapy Clinic Porter's Five Forces Analysis
- Speech Therapy Clinic BCG Matrix
- Speech Therapy Clinic Business Model Canvas
- 7 Critical KPIs for Speech Therapy Clinic Success
- Speech Therapy Clinic Business Plan Template in Pre-Written Word
- Increase Speech Therapy Clinic Profitability: 7 Actionable Strategies
- What Are the Monthly Running Costs for a Speech Therapy Clinic?
- Speech Therapy Clinic Startup Cost: Plan From $183K CAPEX
- Speech Therapy Clinic Financial Model Template in Excel
- How To Open A Speech Therapy Clinic In 3 To 6 Months
- How to Write a Speech Therapy Clinic Business Plan in 7 Steps
- Speech Therapy Clinic Marketing Mix
- Speech Therapy Clinic Marketing Plan
- Speech Therapy Clinic Business Proposal
- Speech Therapy Clinic PESTEL Analysis
- Speech Therapy Clinic Pitch Deck Example Editable PPTX
- Speech Therapy Clinic Business SWOT Analysis
- Speech Therapy Clinic Value Proposition Canvas
Frequently Asked Questions
Owner income can range from no distribution in an early loss year to meaningful profit in a mature clinic In this model, Year 1 shows $625k revenue and -$103k EBITDA, while Year 5 shows $450M revenue and $214M EBITDA Actual take-home depends on taxes, debt, reserves, and whether the owner takes a clinical salary