 Time to Open8 monthsOpening prep
Time to Open8 monthsOpening prepHow to Open an Ultrasound Center: 4 to 8 Month Launch Guide

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open8 monthsOpening prep  Launch Sequence6 stagesCompliance first
Launch Sequence6 stagesCompliance first Key BottleneckStaffing gapProvider coverage
Key BottleneckStaffing gapProvider coverage First Revenue StepCompleted scansClaims ready
First Revenue StepCompleted scansClaims ready


Opening an ultrasound center usually takes 4 to 8 months when you include site selection, legal setup, facility readiness, ultrasound equipment, sonographers, interpreting physicians, billing, and referral outreach The researched planning assumptions show a first-year operating base of 500 monthly service or reading units at modeled capacity, before cardiac ultrasound is added in Year 2 The main bottlenecks are accreditation or payer requirements, payer enrollment, qualified sonographer coverage, and radiologist interpretation agreements First revenue starts when referred or self-pay patients become completed scans with images stored, reports delivered, and claims or payments processed
Time to Open8 monthsOpening prepLaunch Sequence6 stagesCompliance firstKey BottleneckStaffing gapProvider coverageFirst Revenue StepCompleted scansClaims readyLaunch timeline
This is a short web summary of the launch plan, and the XLSX export contains the detailed Gantt Chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8
Licensing
- Entity filing
- Lease diligence
- HIPAA policies
- Accreditation prep
Buildout
- Space layout
- Leasehold buildout
- Utilities setup
- Room furnishing
- Final walkthrough
Equipment
- Machine order
- RIS setup
- Billing setup
- Network install
- Acceptance testing
Staffing
- Role plan
- Recruit sonographers
- Contract radiologist
- Onboard team
- Coverage roster
Payers
- Payer list
- Enroll plans
- Fee schedule
- Billing test
- Cash forecast
Referral marketing
- Referral list
- Outreach calls
- Website launch
- Dry runs
- Go-live
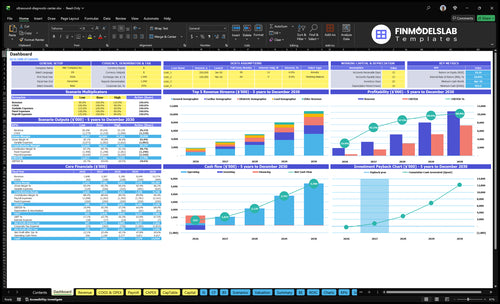
Can your Ultrasound Center model handle the launch ramp?
The screenshot shows dashboard and model tabs, launch timing, revenue, assumptions, costs, cash needs, and break-even logic—open the Ultrasound Center Financial Model Template.
Financial model highlights
- 104 obstetric, 192 general
- 84 lead, 120 reading units
- $154k monthly revenue
- 12% variable, $165k fixed
- Cardiac starts Year 2
What do you need to open an ultrasound center?
To open an Ultrasound Center in the US, treat launch as a due-diligence checklist: entity setup, lease approvals, HIPAA workflows, insurance, payer standards, staffing, imaging systems, and billing readiness. The practical test is covered in What Is The Most Important Metric To Measure The Success Of Ultrasound Center?: can a referral become a scheduled scan, completed image, signed report, and billable claim?
Startup Checklist
- Register the business and tax accounts
- Secure lease and local facility approvals
- Set HIPAA privacy and security workflows
- Buy professional and general liability insurance
Clinical Readiness
- Staff 1 OB sonographer, 2 general sonographers
- Add 1 lead sonographer and 1 radiologist
- Use RIS/PACS, EHR, and billing setup
- Need CLIA only if lab testing occurs
How do you get patients for an ultrasound center?
You get patients for an Ultrasound Center by starting with referral-driven growth: OB/GYN offices, primary care groups, urgent care clinics, and vascular practices if your scope fits, while keeping self-pay scheduling easy; for startup planning, see How Much Does It Cost To Open An Ultrasound Center?. Trust comes from fast orders, clear prep instructions, reliable reports, and follow-up, not broad consumer hype. Local SEO can support cash-pay and convenience searches, but 500 monthly service or reading units is a Year 1 capacity model, not a promise until referral workflows are tested.
Referral sources
- Target OB/GYN offices first
- Add primary care groups
- Work urgent care clinics
- Use vascular practices if relevant
Win trust
- Make online scheduling simple
- Send clear prep instructions
- Deliver reliable reports fast
- Handle billing and collections cleanly
What mistakes should you avoid when opening an ultrasound center?
If you're opening an Ultrasound Center, don’t buy equipment before you prove demand by exam type and lock in referral flow. Also, don’t assume payer enrollment is fast: Year 1 capacity depends on 1 obstetric, 2 general, 1 lead sonographer, and 1 radiologist, and rent, utilities, insurance, RIS/PACS, and EHR/billing already total about $165k per month before payroll and financing.
Before you buy
- Validate demand by exam type first
- Build referral ties before launch
- Check payer enrollment timing
- Confirm counsel on referral fees
Before you bill
- Use full scanning protocols
- Collect consent forms every time
- Set report turnaround clearly
- Build billing handoff into workflow
Build an operational pre-opening checklist for an ultrasound clinic
Launch readiness checklist
Use this go-live approval checklist to confirm the Ultrasound Center is ready before opening.
Compliance
- Entity and permits approvedCritical
The center needs legal approval before it signs leases, hires staff, or opens.
- HIPAA workflow approvedCritical
Protected patient data must be handled correctly before any scans or reports begin.
- CLIA need confirmedMedium
If lab testing is added, CLIA review is needed before launch.
Facility
- Lease and occupancy clearedCritical
The site must be open for medical use before patient service starts.
- Privacy and accessibility setHigh
Patients need private, accessible flow from reception to exam rooms and reports.
- Electrical and network readyHigh
Imaging gear and software need stable power, internet, and data access to run.
Equipment
- Ultrasound machines installedCritical
Scans cannot start until the machines are installed and working.
- RIS PACS and EHR liveCritical
Image storage, charting, and billing need working software on day one.
- Vendor training acceptedHigh
Staff must know the equipment and software before the first patient arrives.
Staffing
- Year 1 hires confirmedCritical
The Year 1 plan calls for the right sonographer and radiologist coverage.
- Interpretation agreement signedCritical
Scans need reading coverage so reports can be issued without delay.
- QA process definedHigh
A basic quality review process helps catch bad images and missed steps.
Revenue
- CPT codes configuredCritical
Correct codes are needed so claims price and route properly.
- Claim and cash-pay testedCritical
Both payment paths must work before the first real patient is billed.
- Referral intake and scheduling liveHigh
Referrals, booking, and reports need one clean flow to create first revenue.
Finance
- Cash runway confirmedCritical
The model shows minimum cash of $493k in Month 4, so runway needs to hold.
- Operating costs loadedHigh
Fixed rent, software, staffing, and service costs must be in the launch budget.
- Go-live signoff completeCritical
Do not open if reading coverage, payer path, QA, or cash runway is still open.
Want the six launch drivers that decide opening readiness?
1Compliance Path
4-8 moWritten policies and payer setup keep opening on track and reduce first-claim friction.
2Facility Ready
Site readyA tested room with utilities, privacy, and access cuts soft-opening cancellations.
3Equipment Buy
Opening dayThe right machine, probes, and image links make day-one scanning possible.
4Clinical Staffing
5 rolesYear 1 coverage across five clinical roles supports predictable scan slots and report turnaround.
5Billing Pipeline
4% feesPayer enrollment and test claims speed the move from orders to collected cash.
6Workflow QA
500 unitsA dry run from intake to report delivery cuts rework and claim denials.
Compliance And Accreditation Path
Compliance Path Before First Scan
If compliance is not mapped early, the center can miss its opening date even when the room and machine are ready. Entity setup, local permits, facility approvals, HIPAA policies, and payer credentialing decide whether you can bill, share results, and look legitimate to referring doctors from day one.
The biggest mistake is assuming one ultrasound rule covers every state. State and payer rules vary, and CLIA review only matters if lab testing is part of the scope. Written policies, an assigned compliance owner, filed applications, and mapped billing rules are the readiness signal. That is what cuts opening delays and keeps payer talks clean.
Lock the Compliance Sequence
Start with the legal entity, then local and facility approvals, then HIPAA, payer enrollment, and accreditation checks tied to payer rules. Do not open referrals before credentialing is live; that creates cash delays and awkward calls with physician offices.
Use a simple launch file with permits, policy drafts, application dates, and payer status. One clean rule: no start date until the compliance owner can show every required filing and a test billing path. If that path is not ready, day-one operations are not ready either.
- Confirm state-specific coverage rules.
- Track every application date.
- Map billing rules before launch.
- Keep HIPAA workflow written.
1
Facility And Imaging-Room Readiness
Imaging-Room Readiness
If the site can’t handle privacy, power, data, and patient flow, the ultrasound center slips before the first scan. A lease that looks fine on paper can still fail on room size, accessibility, or equipment layout, which pushes the opening date and creates day-one bottlenecks.
The real test is a tested room with working utilities, secure network, clean check-in flow, and a setup that meets payer expectations for safe handling and documentation. If the room can’t support the machine, probes, cleaning, and report handoff, the first soft opening turns into cancelled appointments.
Test Before You Sign
Before signing the lease, map the full path from reception to exam room to report space. Verify electrical, network, privacy, accessibility, probe storage, cleaning flow, and vendor access. A good location is one that supports the workflow without staff improvising.
- Check power and data lines.
- Confirm room layout fits equipment.
- Document cleaning and storage steps.
- Test vendor delivery and service access.
Run a dry pass with staff before opening. If the scan, cleanup, and report handoff work in sequence, the site is ready; if not, fix the bottleneck first. That keeps the launch on time and lowers the risk of early cancellations.
2
Ultrasound Equipment Procurement
Launch-Fit Equipment
For an ultrasound center, the wrong machine mix can delay opening even when the room is ready. Year 1 is built around obstetric, general, lead-sonographer services, and radiologist readings, with cardiac sonographer count at 0 until Year 2, so buying for future wish-list services ties up cash and can slow day-one readiness.
Here’s the quick test: the site is ready only when test scans are completed, images are stored, reports are readable, and the vendor support path is in place. Late delivery or missing probes is the main bottleneck, because one missing component can block acceptance testing, staff training, and opening-day service availability.
Buy for Day 1
Match the equipment order to the launch mix before you sign off. That means machine selection, probes, workstation, RIS/PACS connection, image storage, reporting integration, maintenance terms, acceptance testing, and staff training all need one clean owner and one shared schedule.
Use a simple readiness checklist: completed test scans, stored images, readable reports, and a confirmed vendor support contact. If any probe is missing or the image/report flow breaks, the center may open with gaps in service, slower patient throughput, or manual workarounds that hurt day-one cash collection.
- Order only Year 1 service equipment
- Verify every probe arrives
- Test scan-to-report workflow
- Confirm maintenance response terms
- Train staff before opening day
3
Clinical Staffing And Interpretation Coverage
Clinical Staffing Coverage
Staffing decides whether the center can open with real capacity or just an empty schedule. The Year 1 plan needs 1 obstetric sonographer, 2 general sonographers, 1 lead sonographer, and 1 radiologist, with 0 cardiac sonographers in the first year. That mix has to be in place before referrals start, or day-one booking turns into delays and reschedules.
The key dependency is the interpretation workflow. Hire timing, credential documents, exam scope by type, training, and a signed physician read agreement all need to line up with turnaround standards. The readiness signal is simple: staffed schedules and a signed interpretation workflow. If one person is stretched across too many exams, scan slots shrink and report quality drops fast.
Build the coverage plan before opening
Map each exam type to a named sonographer and a named reader before you take referrals. That means verifying credentials, documenting scope limits, and testing the schedule against actual hours, not hopeful coverage. One clean rule helps: no open slot should depend on a single person who can also get pulled into another room.
Also lock the reporting path before the first patient books. Get the physician read agreement signed, confirm training on the handoff process, and set turnaround standards so reports don’t sit unfinished. The launch target is predictable scan slots and trusted reports, not a rushed soft open with coverage gaps.
- Assign exam type by provider.
- Verify licenses and credentials.
- Test schedule coverage by hour.
- Document read workflow and turnaround.
- Block overuse of one sonographer.
4
Payer Billing And Referral Pipeline
Billing and Referral Readiness
First revenue depends on payer enrollment, credentialing, and a working referral path, not just patient demand. If claims can’t be submitted and tracked on day one, orders turn into delayed cash, and opening feels busy but uncollected. The key risk is launching before payer and physician office channels are live, which slows collections and can strain working capital.
For Year 1, billing and collections fees are modeled at 4% of revenue, and patient referral commissions at 3% need compliance review before use. That means the revenue path is not free to run; it needs setup, testing, and rules. A test claim path and live referral contacts are the real go-live checks.
Test Claims Before Open
Before opening, verify payer enrollment, CPT workflow, EHR and billing setup, authorization checks, and the cash-pay process. Run a sample claim from order to submission to denial follow-up, then confirm who fixes errors fast. If the claim path breaks, first-day scans may still happen, but cash collection will lag.
- Confirm payer IDs and credentialing.
- Test claim submission end to end.
- Document referral intake and outreach.
- Review referral commissions for compliance.
- Assign one owner for billing fixes.
What this hides: even a good schedule can stall if referral offices are not sending orders or if authorizations are slow. The practical target is faster conversion from orders to collected cash, not just more scheduled ultrasounds.
5
Operating Workflow And Quality Control
Day-One Workflow and QC
This launch driver decides whether the center can turn an order into a safe scan, a stored image, a signed report, and a billable visit. Day-one flow has to cover intake, eligibility, orders, consent, prep instructions, scan protocol, image storage, report delivery, and billing handoff before the first patient arrives.
The main risk is opening with fast scheduling but slow reports or thin documentation. That creates rework, delays physician updates, and can block clean claims. One broken step can turn completed clinical work into unpaid work. For a diagnostic site, that hurts trust fast, because referring offices expect complete records on day one.
Dry Run the Full Visit
Before opening, run a dry run from scheduling through payment and assign one owner to each handoff. Confirm who checks the order, who verifies eligibility, who collects consent, who gives prep instructions, who stores the images, who sends the report, and who clears billing. Write the steps down so staff do the same thing every time.
- Verify order, consent, and eligibility.
- Test image storage and retrieval.
- Check report routing to physicians.
- Confirm billing handoff fields.
- Assign QA and escalation owners.
- Log follow-up for incomplete exams.
Run one test case for each exam type you plan to offer, and do not open real scheduling until the chart supports billing. If the report is late or the documentation is thin, the visit may look complete clinically but still fail operationally. Clean documentation is what turns scan volume into cash and repeat referrals.
6
Related Products
- Ultrasound Center Porter's Five Forces Analysis
- Ultrasound Center BCG Matrix
- Ultrasound Center Business Model Canvas
- 7 Essential Financial KPIs for Your Ultrasound Center
- Ultrasound Center Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Ultrasound Center Profitability
- What Are the Monthly Running Costs for an Ultrasound Center?
- Ultrasound Center Startup Costs: $605K CAPEX And $493K Cash Need
- Ultrasound Center Financial Model Template in Excel
- How Much an Ultrasound Center Owner Makes at $154K Monthly Revenue
- How to Write an Ultrasound Center Business Plan: 7 Actionable Steps
- Ultrasound Center Marketing Mix
- Ultrasound Center Marketing Plan
- Ultrasound Center Business Proposal
- Ultrasound Center PESTEL Analysis
- Ultrasound Center Pitch Deck Example Editable PPTX
- Ultrasound Center Business SWOT Analysis
- Ultrasound Center Value Proposition Canvas
Frequently Asked Questions
Start with service scope, referral demand, and compliance sequencing For this model, Year 1 opens without cardiac sonography and uses 1 obstetric sonographer, 2 general sonographers, 1 lead sonographer, and 1 radiologist That staffing supports 500 modeled monthly service or reading units at capacity, so validate referral flow before adding wider hours