Ultrasound Center Startup Costs: $605K CAPEX And $493K Cash Need
This ultrasound center cost breakdown covers $605,000 in startup CAPEX, pre-opening expenses, first-year staffing, recurring software, and the working capital needed through the early ramp-up period The model also shows a $493,000 minimum cash need in Month 4, so the funding plan should not stop at equipment and buildout
Calculate Fuding Needs
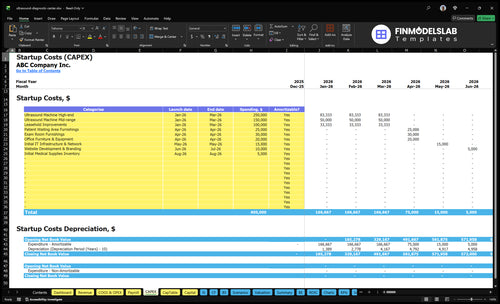
Startup cost summary
This table shows the main opening costs for an ultrasound center and separates capital spending from opening cash needs.
Highlighted CAPEX$375,000Base planning example
Excluded cash needs$493,000Outside CAPEX total
Funding need$868,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Ultrasound machine
$200,000
Machine spec and scanner package
Yes
Leasehold improvements
$100,000
Tenant buildout and finish level
Yes
Patient waiting area furnishings
$25,000
Reception size and décor
Yes
Exam room furnishings
$30,000
Room count and fixture quality
Yes
Office furniture and equipment
$20,000
Reception and admin setup
Yes
Opening cash buffer
$493,000
Cash needed to cover the Month 4 trough
No
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates capitalized startup assets only for an ultrasound center.
!
Scope limits This calculator covers capitalized startup assets only. It excludes payroll ramp-up, operating losses, payer delays, financing costs, debt service, deposits, working capital, and inventory runway; if opening supplies are booked as inventory, fund them outside CAPEX.
Ultrasound startup costs jump as you add machines, rooms, and staff. Lean stays close to one mid-range unit, Base matches the source model, and Full moves above that for a larger outpatient center.
Lean, Base, and Full launch cost comparison for an ultrasound center
Scenario
Lean LaunchReferral testing launch
Base LaunchBalanced two-room launch
Full LaunchScale-ready outpatient center
Launch model
A lean launch uses one mid-range ultrasound machine and a small shared buildout for referral-driven testing.
A base launch follows the source model with one high-end machine, one mid-range machine, and a standard buildout.
A full launch starts above the base case and adds more rooms, machines, probes, staff, and working capital.
Typical setup
It covers one room, basic furnishings, IT, website, and initial supplies.
It includes exam-room setup, furnishings, IT, website, and supplies for a balanced outpatient center.
It supports higher patient flow, more service lines, and a larger clinical team from day one.
Cost drivers
Mid-range machine
shared buildout
furnishings
IT and website
initial supplies
High-end machine
mid-range machine
$100,000 buildout
furnishings
IT and website
supplies
More rooms
more machines
probes
added staff
working capital
Planning rangeCAPEX only
$330,000 - $380,000Lowest cash need
$580,000 - $630,000Model-aligned
Above $605,000Highest capital
Best fit
Best for founders starting with referral volume and a tight footprint.
Best for operators who want a balanced two-room launch with broader service mix.
Best for teams building a scale-ready outpatient center with room to grow fast.
!
Planning note: These scenario ranges are researched planning assumptions, not exact vendor quotes; payer mix, utilization, and local buildout quotes can move the total.
How should I plan funding for an ultrasound center startup?
If you're funding an Ultrasound Center, build the plan around launch timing, reimbursement lag, and cash runway, not just the equipment bill. This model points to $605,000 CAPEX, Month 1 breakeven, and a $493,000 minimum cash need in Month 4, with $368,000 in Year 1 EBITDA, a 17-month payback, 1826% ROE, and 011% IRR. Lenders and investors will check startup cost proof, working capital, payer ramp, staffing, utilization, and equipment useful life, so validate the financial model before you sign leases, order equipment, or hire full staff.
Funding inputs
$605,000 CAPEX drives startup cash need
Month 1 breakeven needs fast patient flow
$493,000 minimum cash in Month 4
17-month payback supports debt and equity review
What backers test
Show payer ramp by month
Match staffing to utilization
Prove reimbursement timing and lag
Check equipment useful life assumptions
What hidden costs of opening an ultrasound center affect cash?
Opening an Ultrasound Center costs more than equipment. Beyond CAPEX, cash gets tied up in reimbursement lag, payer enrollment, radiologist interpretation, accreditation planning, insurance setup, HIPAA policies, software, IT, and billing workflow; see How Much Does The Owner Of Ultrasound Center Typically Make? for the revenue side. Month-one fixed burn already includes $10,000 rent, $1,500 utilities, $1,200 insurance, $2,000 RIS/PACS, $1,800 EHR/billing software, $1,000 IT support, $2,500 service contracts, and $800 supplies and cleaning.
Fixed cash burn
$10,000 rent each month
$1,500 utilities each month
$2,000 RIS/PACS and $1,800 EHR/billing
$2,500 service contracts plus $1,000 IT support
Hidden Year 1 fees
40% billing and collections fee
30% patient referral commissions
20% medical supplies
30% contracted radiologist fees
What drives ultrasound machine cost for startup planning?
For Ultrasound Center, plan machine cost as a range, not a quote: about $150,000 for a mid-range unit or $250,000 for a high-end unit, then add probes, carts, workstations, installation, calibration, warranty, and uptime risk. Service contracts matter too; at $2,500 per month, that is $30,000 a year. If cardiac capability starts in Year 2 staffing, founders should decide now whether to buy it up front or phase it in.
Purchase plan
Compare new and used units
Start with $150,000 to $250,000
Match equipment count to exam mix
Price OB, general, and Doppler probes
Operating risk
Add carts and workstations
Budget $2,500 monthly service
Include installation and calibration
Phase cardiac if staffing starts in Year 2
Key Takeaways
Equipment CAPEX starts at $400k, before service.
Buildout adds $175k and needs clinical-ready space.
PACS/IT runs $4.8k monthly after $15k setup.
Staffing and working capital need $493k by Month 4.
Ultrasound Center Core Five Startup Costs
Ultrasound Equipment Startup Expense
Machine Stack
Two source machines set the base at $400,000: one high-end unit at $250,000 and one mid-range unit at $150,000. That’s before probes, transducers, carts, workstations, installation, calibration, warranty coverage, and backup capacity. This is CAPEX, not payroll or monthly service.
What It Covers
Probes, transducers, carts, workstations, installation, and calibration sit on top of the machine price. Size it with room count, specialty mix, expected scan volume, and whether the site serves obstetric, general, or cardiac studies. Used equipment can lower cash needs, but it can also raise warranty risk and service uncertainty.
Count rooms first.
Match probes to scan mix.
Check used-unit warranty terms.
Monthly Costs
The $2,500 monthly service contract is a recurring operating cost, not equipment CAPEX. Keep it separate from sonographer payroll, since labor and maintenance move for different reasons. If one machine is down, backup capacity matters, so the cheapest upfront option is not always the lowest-risk setup.
Sizing Questions
Start with how many rooms you’ll open, then map each room to the scan mix. An obstetric-heavy center may need different probes and more uptime than a general-only site, while cardiac volume can change equipment needs fast. If you buy used machines, ask for calibration history and warranty scope before you sign.
Staffing And Working Capital Startup Expense
Launch Payroll
Staffing is a startup cash need, not equipment. The Year 1 team includes a center director at $95,000, lead sonographer at $110,000, 3 sonographers at $80,000 each, an employed radiologist at $300,000, a patient coordinator at $42,000, billing/admin at $48,000, and a physician liaison at $75,000.
Budget Inputs
Build this line from headcount, salary, and months before revenue. Add launch training, recruiting, uniforms, front desk setup, billing workflow, and supplies. These costs hit before collections do, so they belong in startup funding, not CAPEX.
Count each paid role separately
Cover pre-open payroll months
Include training and setup costs
Keep It Lean
Start with the minimum clinical coverage, then add hours only when scheduled volume supports them. Don’t cut radiologist or billing support too hard; weak reads or slow claims can hurt cash faster than one extra salary saves it.
Stage hires to patient volume
Protect billing and report speed
Buy uniforms once, not twice
Cash Buffer
$493,000 minimum cash in Month 4 is the working capital signal. That buffer has to carry payroll, supplies, and the gap between service dates and cash receipts. If cash falls below that line, the launch is underfunded even if the machines are paid for.
Ultrasound Center Buildout Startup Expense
Buildout Budget
The buildout budget is about $175,000: $100,000 leasehold improvements, $25,000 waiting area furnishings, $30,000 exam room furnishings, and $20,000 office furniture and equipment. That covers the space before imaging gear arrives, so keep it separate from the $400,000 machine package. A normal office lease is not clinical-ready, so plan for a true healthcare fit-out.
Fit-Out Scope
Here’s the quick math: room count and square footage drive the spend. Buildout needs waiting room, reception, exam rooms, accessible access, patient privacy, electrical, HVAC, plumbing, lighting, storage, signage, and a clean workflow from check-in to scan. Local code rules and the landlord’s tenant improvement allowance can move the budget fast.
Control The Spend
Lock the layout before you sign, then build before equipment delivery so you do not pay twice for moves and rework. The best savings come from early code review, a clear room count, and a strong tenant improvement allowance. Biggest mistakes are underbuilding privacy, power, and HVAC, then fixing them after the lease is live.
Day-One Readiness
What this estimate hides: a small suite can still run over if the lease needs more square feet, more rooms, or heavier code work. If the landlord contribution is weak, the tenant pays more cash upfront. So the real test is whether the space is ready for clinical imaging on day one.
Licensing, Accreditation, And Payer Setup Startup Expense
Licensing Setup
Licensing and payer setup are not plug-and-play. Budget for business registration, state medical facility requirements, local permits, legal review, accounting setup, HIPAA policies, compliance files, and the model’s $1,200 monthly insurance line for general liability and malpractice, or $14,400 a year.
Payer Enrollment
Payer credentialing can delay cash. Build for enrollment time, document rework, and billing setup before launch. Add radiologist coverage agreements and a medical director if your state or structure needs one. If claims cannot go out on day one, fixed costs still run, so launch runway has to cover the gap.
Accreditation
Accreditation planning is mostly documentation work. Expect policies, quality checks, image storage rules, report workflows, and proof that staff follow them. The cost sits in legal time, admin time, and repeat submissions if files are incomplete. Do not assume every state or payer asks for the same package.
Go-Live Readiness
Do not open until billing is ready. Test payer enrollment, claim setup, compliance files, and coverage agreements before the first patient arrives. That is where cash risk hides: a clean schedule does not help if claims sit unbilled for weeks, or if missing documents trigger rework after launch.
PACS And IT Setup Startup Expense
PACS and RIS
PACS stores and shares ultrasound images, and RIS schedules studies, tracks status, and helps reporting. For launch, budget $15,000 for IT infrastructure and network, then $2,000 monthly for RIS/PACS, $1,800 for EHR (electronic health record)/billing software, and $1,000 for IT support. That is $4,800 a month before implementation fees.
Cost Inputs
Here’s the quick math: use one-time quotes for setup, then add monthly fees for storage, support, and billing. The estimate depends on workstations, image storage size, DICOM workflow needs, cybersecurity controls, and billing integration. If pricing is per study instead of flat subscription, model it against expected scan volume.
Keep It Lean
Cut waste by standardizing workstations, limiting custom integrations, and matching storage to real volume. Don’t skimp on network reliability or cybersecurity; a weak link can stop image access and billing. Ask for clear implementation fees, service terms, and support response times. The best savings usually come from clean scope, not the cheapest software.
Budget Impact
This setup adds $15,000 upfront and $4,800 a month in software and support, or $57,600 a year. For an ultrasound center, that fixed load matters before volume is steady, so cash planning has to cover image storage, reporting, and billing even if early patient flow is light.