 Time to Open6-12 monthsSetup window
Time to Open6-12 monthsSetup windowHow To Open An Urgent Care Center In 6 To 12 Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open6-12 monthsSetup window  Launch Sequence8 stagesValidate market
Launch Sequence8 stagesValidate market Key BottleneckCredentialing delayPayer lead time
Key BottleneckCredentialing delayPayer lead time First Revenue StepInitial visitsBooking live
First Revenue StepInitial visitsBooking live


You’re launching a walk-in clinic where licensing, buildout, payer credentialing, staffing, and systems all have to land before opening day This guide covers the urgent care opening checklist, a practical 6 to 12 month startup timeline, and the first revenue actions tied to search, referrals, employer outreach, and walk-in traffic Use the financial model only to validate ramp assumptions, including Year 1 capacity of 55% to 65% across key clinical roles
Time to Open6-12 monthsSetup windowLaunch Sequence8 stagesValidate marketKey BottleneckCredentialing delayPayer lead timeFirst Revenue StepInitial visitsBooking liveLaunch timeline
This short web summary shows the urgent care launch timeline, and the XLSX export contains the detailed Gantt chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8Month 9
Licensing / compliance
- License checklist
- Permit filings
- Policy manual
- Inspection prep
- Final approval
Site / buildout
- Lease review
- Floor plan
- Buildout work
- Utility rough-in
- Punch list
Equipment / tech
- Vendor quotes
- Equipment orders
- Lab and imaging
- EHR build
- Booking live
Payer enrollment
- Payer list
- Enrollment packs
- Submit apps
- Contract follow-up
- Effective dates
Staffing / training
- Recruit clinicians
- Hire support
- Privilege review
- Train workflows
- Mock visits
Marketing / launch
- Search listings
- Website launch
- Referral outreach
- Opening promo
- Grand opening
Why is a financial model critical before launch?
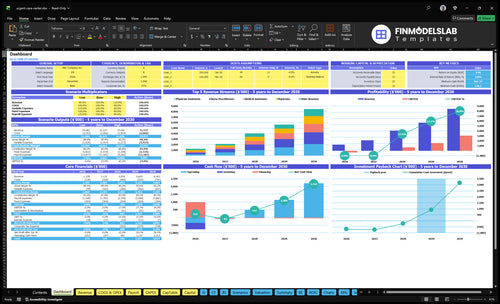
Use the Urgent Care Center Financial Model Template to test launch timing, payer mix, visit volume ramp, staffing, provider coverage, cash runway, and break-even. It also shows revenue, costs, cash needs, and assumptions—open the model.
Financial model highlights
- Planned revenue: $103,250
- Direct costs: 19%
- Rent: $12,000 monthly
- Utilities: $1,800 monthly
- Maintenance: $1,000 monthly
- Break-even sensitivity
What licenses are needed to open an urgent care center?
An Urgent Care Center usually needs business registration, state facility approval if required, clinician licenses, medical director rules, malpractice coverage, a CLIA waiver for basic lab tests, HIPAA and OSHA procedures, payer enrollment, and local zoning/signage permits before opening. Since rules vary by state, treat this as a founder checklist, then verify corporate practice of medicine rules with counsel and track demand with What Is The Current Growth Rate Of Patient Visits At Your Urgent Care Center?.
Core licenses
- Register the business entity first
- Confirm state medical facility approval
- License every clinician before patient care
- Assign medical director if required
Opening checks
- Get CLIA waiver before waived lab testing
- Set HIPAA privacy policies before intake
- Follow OSHA rules; logs apply over 10 employees
- Use 10-digit NPI for payer enrollment
What urgent care launch risks cause opening-day problems?
Opening-day problems usually come from revenue, staffing, and readiness gaps: if payer enrollment is not complete, visits may not turn into collectible claims, and if credentialing or billing workflows are not tested, cash collection slows. The fix is to start credentialing early and lock in the Year 1 team of 1 physician, 1 physician assistant, 1 nurse practitioner, 1 radiology tech, and 2 medical assistants before launch. Weak local visibility can also suppress first visits, so search, signage, booking, and referral outreach need to start before opening.
Billing first
- Start credentialing early.
- Test claims before launch.
- Fix EHR setup before opening.
- Unbilled visits hurt cash flow.
Launch ready
- Staff to Year 1 plan.
- Check CLIA and HIPAA.
- Confirm OSHA and lab readiness.
- Build local visibility before day one.
How long does it take to open an urgent care center?
Plan on 6 to 12 months to open an Urgent Care Center. That timeline is usually set by site buildout, inspections, payer credentialing, EHR and billing setup, hiring, and equipment delivery. Start payer enrollment early and run it alongside buildout, because the clinic can be physically ready but still not revenue-ready if EHR training, billing workflows, CLIA waiver, radiology workflow, or provider coverage slips. In Year 1, model only 55% to 65% capacity, so you do not assume full volume in month one.
What drives timing
- 6 to 12 months is the practical range.
- Buildout and inspections control the date.
- Credentialing and enrollment start early.
- Hiring and equipment can shift launch.
What can delay revenue
- EHR setup can lag opening day.
- Billing workflows need live testing.
- CLIA and radiology steps can slip.
- Provider coverage affects day-one revenue.
Use this urgent care opening checklist as a go/no-go screen
Launch readiness checklist
Use this go-live approval checklist before opening to confirm the clinic is ready to start seeing patients.
Clearances
- Entity registration completeCritical
The clinic needs a legal entity before permits, accounts, and contracts move forward.
- State clinic rules reviewedCritical
State facility rules shape what can open, staff, and bill from day one.
- Medical director coverage setCritical
Medical director oversight is a core launch control for clinical operations.
- Malpractice policy boundCritical
Coverage should be active before the first patient is seen.
Site flow
- Lease and zoning approvedCritical
The site must allow medical use before build-out money is spent.
- ADA access confirmedHigh
Accessible entry and rooms reduce launch risk and patient barriers.
- Triage and reception flow setHigh
Clear flow keeps walk-ins moving and limits bottlenecks at check-in.
Clinical setup
- X-ray unit installedCritical
Imaging is a core service, so the unit must work before opening.
- Basic lab equipment readyHigh
Point-of-care testing needs ready equipment if the clinic will offer it.
- Supply par levels setHigh
Supplies must cover the first patient surge without service gaps.
Staffing
- Year 1 team hiredCritical
Opening staffing should match the Year 1 model for patient flow.
- Clinical coverage scheduledCritical
Coverage must hold for physicians, advanced practice staff, and support staff.
- Staff training completedHigh
Staff need clear steps for triage, rooming, charting, and escalation.
Systems
- EHR and billing liveCritical
Records and claims must work before the first visit is billed.
- Payer enrollment completeCritical
Enrollment must be done or cash collection will lag after launch.
- Lab and imaging workflow testedHigh
Tested handoffs keep outside labs, imaging, and results from stalling care.
Financials
- Runway covers opening lossCritical
Year 1 EBITDA is negative, so cash must cover the early loss period.
- Visit volume target validatedHigh
Volume must support the staffing ramp and the breakeven path.
- Go-live signoff completeCritical
Final signoff should confirm compliance, staffing, systems, and cash are ready.
Which six drivers decide if the urgent care launch is ready?
1Licensing
License gateA complete compliance file clears go-live; missing state approvals or protocols can delay opening.
2Buildout
Site readyA compliant site with utilities, layout, and inspections keeps patient flow from bottlenecking on day one.
3Billing
Payers liveCredentialing and billing must be live before insured visits turn into collectible revenue.
4Staffing
Y1 crewYear 1 staffing needs 1 physician, 1 PA, 1 NP, 1 radiology tech, and 2 medical assistants.
5Systems
Day 1 liveWorking equipment, EHR, lab, and imaging links cut service stops and keep visits moving.
6Local Launch
55-65% capLocal search, referrals, and outreach push the first 30 to 90 days of visit ramp.
Licensing And Compliance
Licensing and Compliance
Licensing and compliance decides whether the clinic can open at all. A walk-in urgent care cannot safely see patients until state-specific approvals, a licensed medical leader, malpractice coverage, and written HIPAA (health privacy law) and OSHA (workplace safety rules) procedures are in place. If testing is offered, a CLIA waiver (federal permission for simple lab tests) is also part of day-one readiness.
The real risk is state variation and missing paperwork. One gap can delay inspections, force a narrower scope of services, or push back opening even if the buildout is done. The readiness signal is a complete compliance file, documented protocols, licensed clinicians, confirmed scope of services, and inspection-ready records. No file, no open.
Build the compliance file first
Before you set an opening date, verify the items that must clear before first patient. That keeps staffing, payer setup, and service launch lined up with the actual approval path, not a hopeful calendar date.
- Confirm facility rules by state
- Lock medical leadership coverage
- Verify malpractice policy terms
- Document HIPAA and OSHA workflows
- Check CLIA waiver needs for testing
- Review payer enrollment requirements
- Train staff on privacy and safety
- Test inspection readiness in advance
If documentation is thin, opening gets messy fast: staff can be hired but not used, tests may need to pause, and first-day visits may be limited to a smaller service set. That means slower revenue and more cash tied up before the clinic can operate at full speed.
1
Site Selection And Buildout
Site Fit and Buildout
This driver matters because an urgent care center cannot open on time if the site misses zoning, ADA access, parking, or signage rules. The right space also shapes patient flow from reception to triage, exam rooms, supplies, and radiology if offered, so a bad layout can slow visits on day one.
The readiness signal is a signed lease with compliant use, a buildout plan, an inspection path, installed utilities, a signage plan, and room-by-room workflow. The main bottlenecks are lease work, tenant improvements, permits, and inspections, which can push opening and burn cash before the first patient walks in.
Map the room flow before you sign
Before the lease is final, verify the space supports urgent visits: reception, triage, exam rooms, supplies, and staff movement. If radiology is part of the plan, lock the layout and utilities for that now, not later. One clean layout change can save weeks of rework.
- Confirm compliant use in writing.
- Review permit and inspection steps.
- Place signage early in the plan.
- Test patient and staff paths.
Sequence the buildout around long-lead items first: tenant improvements, utilities, permits, then inspection sign-off. If any step slips, the clinic may open with chokepoints at intake or in exam rooms, which hurts first impressions and slows cash collection from the first visits.
2
Payer Credentialing And Billing
Billing Readiness Before Open
Payer credentialing and billing setup decide whether insured visits turn into cash on time. If providers can see patients but are not enrolled, contracted, and coded correctly, the clinic can still open but most visits will sit as uncollected revenue. That delays cash, strains working capital, and makes day-one operations look busy but weak on collections.
The launch gate is simple: payer enrollment in progress or complete, billing software live, coding rules set, and denial handling assigned. Year 1 assumes billing and EMR software cost 3% of revenue, so this is not a back-office side task. It is part of the ramp model, and it affects how fast first visits convert to cash.
Start Enrollment Early
Begin credentialing while buildout and hiring are still moving. That keeps the opening date tied to real billing readiness, not just clinical staffing. Test the full path before go-live: patient registration, coding, claim submission, payment posting, and denial review. One clean test claim is worth more than a long checklist.
- Confirm payer applications are submitted.
- Test clearinghouse claim flow.
- Train staff on code entry.
- Assign one denial owner.
- Verify billing software is live.
Weak execution here creates a hidden launch delay: the clinic may be open, but insured visits still need manual fixes, resubmits, and extra follow-up. That slows cash conversion after the first patient visits and can force the owner to fund payroll and vendors longer than planned.
3
Clinical Staffing And Provider Coverage
Clinical Coverage Ready
Patient flow breaks fast if the clinic opens without licensed coverage. For this urgent care center, day-one access depends on a staffed schedule, backup coverage, credentialed clinicians, triage workflows, and role-specific training before go-live.
The Year 1 model uses 1 physician, 1 physician assistant, 1 nurse practitioner, 1 radiology tech, and 2 medical assistants. Modeled monthly capacity is 160 physician visits, 200 PA visits, 200 NP visits, 300 radiology tech services, and 250 MA services per assistant before capacity adjustment. Hire gaps are the main bottleneck, and weak coverage means longer waits and a less safe first month.
Staff the Schedule First
Build the opening roster before you set the launch date. The clinic is not ready until every shift has a named lead, a backup for each clinical role, and front desk coverage tied to intake, triage, billing support, and escalation paths.
- Verify all 5 clinical roles are covered.
- Document backup coverage for each shift.
- Train staff on triage and handoffs.
- Test opening-day patient flow by role.
- Confirm capacity against the visit plan.
What this hides: if one provider slips late, the whole schedule can compress. That can push start dates, cut same-day access, and force overtime or temp coverage before the clinic is stable.
4
Equipment, EHR, Lab And Radiology Setup
Equipment and Systems Go-Live
An urgent care clinic can’t open cleanly until exam equipment, EHR (electronic health record), billing, and lab/imaging routing all work together. If one link is down, staff may still see patients, but they can’t document care, order tests, collect payment, or bill claims on day one.
The setup also needs medical supplies at 7% of revenue, pharmaceuticals at 4%, outsourced lab and imaging at 5%, and billing and EMR software at 3%. Here’s the quick math: those lines total 19% of revenue, so missing stock or a failed go-live hits both cash and service flow fast.
Pre-Open Test Plan
Before opening, verify the clinic can register patients, document visits, order tests, take payment, and route lab or imaging without manual workarounds. Test phones, online booking, point-of-care testing if offered, and the handoff to outside lab and radiology vendors.
- Run one full patient flow end to end.
- Confirm supply counts before delivery week.
- Train staff on every system screen.
- Fix vendor install issues before go-live.
The main bottleneck is technology go-live and vendor installation. If setup slips, the clinic may still open, but visits slow down, charges get delayed, and missing orders create service interruptions.
5
Patient Acquisition And Local Launch
Local Patient Demand Before Open
This launch driver matters because first revenue starts only if nearby patients know the clinic exists before opening day. The readiness signal is a live local search profile, website service pages, online booking, phone lines, signage, launch hours, and insurance information. Without that, the clinic can open on time and still sit empty.
The first 30 to 90 days should push local search, walk-ins, referrals, schools, sports programs, and nearby employers. The Year 1 plan assumes ramped demand, not full demand: 60% capacity for physician, physician assistant, and nurse practitioner services, 55% for radiology tech services, and 65% for medical assistant services. Weak visibility is the main bottleneck.
Pre-Open Visibility Setup
Before opening, verify that every patient touchpoint is live and tested: search profile, booking, phones, signage, hours, and insurance details. Then assign outreach to local employers, schools, and sports groups so the clinic is not waiting for word-of-mouth to start. One clean launch can still miss revenue if people cannot find the door or book fast.
- Test booking on mobile and desktop.
- Confirm phone coverage at launch.
- Post insurance and service pages.
- Schedule outreach before opening week.
- Track visits daily for 90 days.
6
Related Products
- Urgent Care Center Porter's Five Forces Analysis
- Urgent Care Center BCG Matrix
- Urgent Care Center Business Model Canvas
- 7 Key Metrics to Track for Urgent Care Center Profitability
- Urgent Care Center Business Plan Template in Pre-Written Word
- 7 Strategies to Boost Urgent Care Center Profit Margins
- How Much Does It Cost To Run An Urgent Care Center Each Month?
- Urgent Care Center Startup Costs: $413K CAPEX Planning Budget
- Urgent Care Center Financial Model Template in Excel
- How Much Does an Urgent Care Center Owner Make at 46 Visits a Day?
- How to Write an Urgent Care Center Business Plan (7 Steps)
- Urgent Care Center Marketing Mix
- Urgent Care Center Marketing Plan
- Urgent Care Center Business Proposal
- Urgent Care Center PESTEL Analysis
- Urgent Care Pitch Deck Example Editable PPTX
- Urgent Care Center Business SWOT Analysis
- Urgent Care Center Value Proposition Canvas
Frequently Asked Questions
Start by confirming state rules, choosing a compliant site, appointing medical leadership, and mapping payer credentialing before buildout goes too far A practical launch plan runs 6 to 12 months The researched Year 1 staffing model uses 1 physician, 1 physician assistant, 1 nurse practitioner, 1 radiology tech, and 2 medical assistants