 Owner income~$220k
Owner income~$220kHow Much Does an Urgent Care Center Owner Make at 46 Visits a Day?

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income~$220k  Net margin103%
Net margin103% Revenue for target pay~$213k
Revenue for target pay~$213k Business difficultyHard
Business difficultyHard


You’re weighing clinic ownership against a costly payroll, so this page separates urgent care center revenue and profit from owner take-home pay In the researched model, revenue moves from $124M in the first year to $213M in the second year, while EBITDA moves from -$200k to $220k before debt, taxes, reserves, and reinvestment This is US planning context, not personal tax advice or a guaranteed distribution
Owner income~$220kNet margin103%Revenue for target pay~$213kBusiness difficultyHardWant to test your urgent care owner income?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate, not guaranteed salary, tax advice, or owner distribution advice. Actual owner income will change with collections, staffing, payer mix, debt, and reserve policy.
Want to see how owner income fits in the Urgent Care Center model?
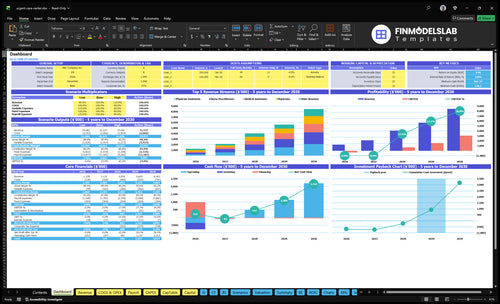
Open the Urgent Care Center Financial Model Template to review revenue, EBITDA, cash flow, owner income, and break-even charts. It tests $124M, $213M, and $406M revenue paths, and owner pay follows operating cash needs.
Owner-income model highlights
- Owner pay comes later
- Volume links to revenue
- Scenarios test assumptions
Can one urgent care center support an owner?
An Urgent Care Center can support an owner only when volume, collections, staffing, and reserves all work together. In this model, Year 1 EBITDA is -$200k, so distributions do not work; Year 2 EBITDA is $220k, which may allow limited owner pay before debt, taxes, reserves, and reinvestment. By Year 3, the model shows $114M EBITDA and about 85 daily billable encounters, but staffing still has to keep pace.
Owner pay timing
- Year 1: -$200k EBITDA
- No distributions in Year 1
- Year 2: $220k EBITDA
- Limited owner pay only
What fixes a weak site
- 85 daily billable encounters helps scale
- Improve utilization first
- Push payer contracts and collections
- Control costs before new sites
Can an urgent care owner pay themselves a salary?
Yes, an owner can pay themselves a salary at an Urgent Care Center if it is built into the budget and fits the ownership and clinical setup. Non-physician owners still need licensed clinical coverage and medical direction, so don’t assume every owner can practice medicine. In the modeled payroll, the Medical Director is 0.8 FTE at $160k in Year 1, plus a physician at $220k; an owner-operator salary reduces EBITDA (earnings before interest, taxes, depreciation, and amortization), and distributions come after operating needs. Year 2 EBITDA of $220k is the pre-tax pool before debt, reserves, reinvestment, and owner distributions.
Owner salary rules
- Pay salary only if budgeted.
- Match ownership and clinical rules.
- Keep licensed coverage in place.
- Use distributions after expenses.
Model math
- Medical Director: 0.8 FTE.
- Medical Director pay: $160k Year 1.
- Physician pay: $220k.
- Year 2 EBITDA: $220k.
What profit margin does an urgent care center make?
If you're sizing an Urgent Care Center, start with How Much Does It Cost To Open Your Urgent Care Center? because profit can swing hard early: the model shows -161% EBITDA margin in Year 1, then 103% in Year 2 and 281% in Year 3. Margin improves as core provider capacity rises from 60% to 70%, fixed costs spread over more encounters, and owner income is planned from collected revenue, not gross billed charges.
Year 2 math
- $213M revenue
- $122M wages
- $3,036k fixed overhead
- 182% supply and variable costs
What moves margin
- Payer mix changes collections fast
- Denials cut net revenue
- Coding errors hit margin
- Provider payroll moves profit
Want to see the main income drivers?
1
28-85/dayPatient Volume
Moving from 28 to 85 daily billable encounters is what flips the clinic from heavy losses to strong profit because fixed costs spread over more visits.
2
$125-$133Net Collections
A small lift in revenue per visit adds up fast once the center is seeing steady walk-ins.
3
$900K-$1.9MProvider Staffing
Staffing rises quickly, so scheduling and role mix decide how much of each visit turns into take-home profit.
4
$253K/moOverhead Discipline
With fixed overhead at about $253K per month, the clinic needs steady volume and tight reserve control because reserves and taxes sit outside EBITDA.
5
HighPayer Mix
A better payer mix keeps collections near the top of the visit range and improves margin without adding many new visits.
6
Add-onsAncillary Services
X-ray and basic lab work add revenue per encounter, so these services raise income without needing the same lift in exam-room traffic.
Urgent Care Center Core Six Income Drivers
Patient Volume
Patient Volume
Urgent care visits per day is the main fixed-cost lever. At 28 daily billable encounters in Year 1, the clinic misses break-even; at 46 in Year 2, it clears it; at 85 in Year 3, expanded staffing can spread $253k in monthly fixed overhead and provider payroll across more visits, which supports owner pay.
The catch is throughput. Long waits, weak local demand, limited hours, and thin provider coverage can cap volume and hurt collections. If volume stays above break-even, cash flow gets more stable and the owner can draw from profit with less month-to-month swing.
Track Visits per Day
Measure billable encounters per day, not just check-ins. Track daily volume by hour, provider, and day of week so you can see when demand outruns staffing. The real target is enough consistent visits to cover fixed overhead, not a one-time busy week.
- Watch wait times before volume slips.
- Match hours to peak demand.
- Staff for peaks, not averages.
- Test local demand by zip code.
- Keep coverage thin only if safe.
Use those numbers to decide when to add shifts or cut dead hours. If the clinic can hold Year 2 volume near 46 visits/day and keep moving toward 85, the owner gets a cleaner profit line and less risk of drawing cash before the clinic can fund itself.
1
Net Collections Per Visit
Net Collections Per Visit
This is the cash you actually keep per billable urgent care visit, not the charge on the claim. Use net collections per visit = cash collected ÷ billable encounters. In this model, average revenue per billable encounter rises from $125 in Year 1 to $129 in Year 2 and $133 in Year 3, driven by contracted reimbursement, coding, self-pay policy, denials, and collections speed.
Small changes move owner pay fast. At 1,000 visits, a $1 gain adds $1,000 a month, and the shift from $125 to $133 adds $8,000. With Year 2 margin at 103%, payer underpayment, denied claims, or slow collections can cut EBITDA (earnings before interest, taxes, depreciation, and amortization) without adding the same labor.
Tighten Cash Per Visit
Track collections by payer type: commercial, Medicare, Medicaid, workers’ compensation, and self-pay. Reconcile charges, allowed amounts, denials, and days to cash every month. If credentialing lags or denials rise, your net collections per visit will fall even when visit volume looks fine.
Use a front-desk collection script and a clear self-pay policy, then audit underpayments and coding misses. A small leak on each encounter compounds across every visit. Better collections lift EBITDA without the same labor load, so more of each extra dollar can flow to owner draw.
2
Provider Payroll
Provider Payroll
Provider payroll is the biggest controllable cost block in an urgent care center. It covers the Medical Director, physicians, physician assistants, nurse practitioners, radiology techs, medical assistants, the clinic manager, and front desk staff. The owner only wins when staffing matches visit volume by hour, because payroll that runs ahead of demand cuts margin and cash for owner pay.
The modeled wage load is $900k in Year 1, $122M in Year 2, and $1925M in Year 3. Too much coverage means paying for idle rooms; too little means slower throughput, weaker quality, and unsafe hours. The key metric is labor cost per billable encounter, not headcount alone.
Match Coverage to Visits
Track visits per day, peak-hour demand, and labor hours by role. Staff the highest-cost clinicians only where scope of practice requires them, then use PAs, NPs, MAs, and front desk support to keep flow moving. Better staffing match protects profit and makes owner take-home more stable.
- Visits per day by hour
- Labor hours by role
- Labor cost per encounter
Stress-test the roster before adding shifts: overstaffing before volume, understaffing during peaks, and expensive physician coverage are the main leaks. If demand is thin, fixed provider hours crush margin; if peaks are uncovered, wait times rise and visits are lost. Watch call-outs, training time, and local wage pressure.
3
Payer Mix
Payer Mix
Payer mix is the split of commercial insurance, Medicare, Medicaid, workers’ compensation, and self-pay visits. It changes net collections per visit and days to cash, so the same visit count can produce very different owner pay. Charges don’t pay payroll; collections do.
Model this as visit volume × payer mix-weighted net collections per visit. In the model, revenue per billable encounter rises from about $125 in Year 1 to $129 in Year 2 and $133 in Year 3, so small mix shifts matter. Weak contracts, delayed credentialing, denials, and self-pay leakage can squeeze cash even when volume holds.
Track Collections, Not Charges
Measure net collections by payer, denial rate, and days to cash every month. Split commercial, Medicare, Medicaid, workers’ comp, and self-pay so you can see which mix truly funds overhead. With fixed overhead at $253k per month, slow payers can block owner draws fast. One bad payer mix can hide strong traffic.
Fix the cash levers first: finish credentialing fast, tighten coding, collect self-pay at check-in, and review underpaid claims weekly. The goal is to lift net collections per visit and shorten days to cash without adding rooms. Stronger contracts and cleaner collections improve margin and protect take-home pay.
4
Ancillary Services
Ancillary Revenue
Ancillary services are add-on items such as X-rays, labs, physicals, vaccines, drug testing, workers’ compensation, and employer contracts. They raise revenue per encounter, but only when visit volume, coding, and payer rules support the service mix. One extra test can lift cash per visit; if it is denied or underused, margin slips instead.
The key inputs are visit volume, service mix,
Track Revenue by Service Line
Measure each add-on separately: X-ray count, lab volume, vaccine mix, and drug test claims. Compare collected dollars per visit with and without ancillaries, then watch denial rates and days to cash. If a service does not cover its staffing, coding, and supply cost, it is not helping owner income.
Test the services with the best payer fit first. Keep a simple rule: add only what your staff can code cleanly and use often enough to avoid idle equipment. Low utilization and outsourced lab fees can erase the upside fast, so forecast margin by service, not just total visits.
- Track revenue per encounter
- Watch denial and write-off rates
- Check equipment utilization weekly
- Price for staffing and compliance
5
Overhead and Reserves
Overhead and Reserves
Overhead is the cash leak that comes after visits are billed. In this urgent care model, fixed overhead is $253k per month, including $12k rent, $35k malpractice insurance, $3k marketing, and $25k IT and software. That is about $3.0M a year before debt, taxes, reserves, and reinvestment, so owner pay can stay tight even when EBITDA is positive.
Protect Owner Cash
Track net cash after overhead, not just EBITDA. Here’s the quick math: each month, subtract fixed overhead, the 76% variable fees for lab, imaging, billing, and EMR, then reserve for debt service, taxes, and reinvestment. If distributions start before those cash needs are funded, the owner may have to put money back in. Tight billing, clean collections, and a set reserve policy protect take-home pay.
6
Compare low, base, and high urgent care owner income scenarios
Owner income scenarios
Owner income swings hard here because volume, pricing, and staffing scale together. Early losses can flip to cash flow once daily encounters and capacity rise.
| Scenario | Low CaseRamp-up risk | Base CaseBreak-even | High CaseScale leverage |
|---|---|---|---|
| Launch model | This is the weaker earnings path, with year 1 still under pressure from startup ramp and thin cash flow. | This is the modeled middle path, where the clinic moves into positive EBITDA but still has tight cash before tax and reinvestment. | This is the stronger earnings path, where higher daily volume and more staffed capacity drive much faster owner income. |
| Typical setup | About 28 daily billable encounters, roughly $125 average revenue per encounter, and negative EBITDA as staffing and fixed costs outrun early volume. | About 46 daily billable encounters, about $129 average revenue per encounter, and a leaner cost base that starts to cover fixed overhead. | About 85 daily billable encounters, about $133 average revenue per encounter, and a bigger team that spreads fixed costs across more visits. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | -$200kNo safe base | $220kTight cash | $114MUpside case |
| Best fit | Use this to stress-test the first operating year and see how much loss the clinic can absorb. | Use this as the working plan for lender talks, hiring pace, and cash monitoring in year 2. | Use this to test upside if the clinic fills capacity faster and holds pricing while adding staff. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Urgent Care Center Porter's Five Forces Analysis
- Urgent Care Center BCG Matrix
- Urgent Care Center Business Model Canvas
- 7 Key Metrics to Track for Urgent Care Center Profitability
- Urgent Care Center Business Plan Template in Pre-Written Word
- 7 Strategies to Boost Urgent Care Center Profit Margins
- How Much Does It Cost To Run An Urgent Care Center Each Month?
- Urgent Care Center Startup Costs: $413K CAPEX Planning Budget
- Urgent Care Center Financial Model Template in Excel
- How To Open An Urgent Care Center In 6 To 12 Months
- How to Write an Urgent Care Center Business Plan (7 Steps)
- Urgent Care Center Marketing Mix
- Urgent Care Center Marketing Plan
- Urgent Care Center Business Proposal
- Urgent Care Center PESTEL Analysis
- Urgent Care Pitch Deck Example Editable PPTX
- Urgent Care Center Business SWOT Analysis
- Urgent Care Center Value Proposition Canvas
Frequently Asked Questions
In this model, first-year take-home is not supported because EBITDA is about -$200k on $124M revenue By the second year, the clinic produces about $220k of EBITDA on $213M revenue That is not the owner’s guaranteed pay Debt, reserves, taxes, and reinvestment reduce cash distributions