VAD Services Startup Costs: $113M First-Year Funding Floor

It costs about $113M to start ventricular assist device services under the provided first-year planning model The total combines $645k of CAPEX for telehealth, servers, simulation equipment, controllers, workstations, and patient education tools, plus $483k of minimum cash needed by Month 6 The model also assumes Year 1 revenue of $1709M, EBITDA of $319k, breakeven in Month 2, and payback in 17 months Treat these numbers as researched startup planning assumptions, not guaranteed quotes, payer terms, or clinical outcome projections
VAD Services CAPEX Calculator Objective
Startup CAPEX Calculator
Estimates capitalized startup assets only for a ventricular assist device services launch.
Important limits This calculator covers capitalized startup assets only. It excludes initial inventory, payroll runway, deposits, debt service, working capital, reimbursement lag, credentialing delays, operating losses, and other non-CAPEX funding needs. Deployment should be treated as startup-period spend, not one lump sum.
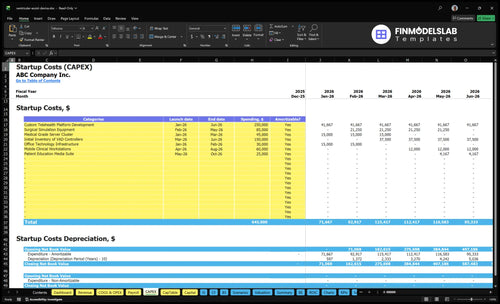
What does the Ventricular Assist Device Services screenshot show?
This Ventricular Assist Device Services Financial Model Template screenshot shows CAPEX categories, launch timing, costs, and depreciation or amortization, plus staffing ramp and reimbursement lag. Open it and adjust assumptions.
Key model highlights
- $645k base CAPEX
- $483k Month 6 cash
- Month 2 breakeven
How much does it cost to start VAD services in the US?
Starting Ventricular Assist Device Services in the US costs about $1.13M for the base affiliated implantation and follow-up model: $645k CAPEX plus $483k minimum cash. A lighter management-only or partner-hospital model can cost less, while a full high-acuity service line can cost more; see owner-side economics here: How Much Does An Owner Make From Ventricular Assist Device Services?
Base startup floor
- $645k startup CAPEX
- $483k minimum cash reserve
- $1.128M first-year funding floor
- Affiliated implantation and follow-up model
Cost drivers
- 2 cardiothoracic surgeons
- 4 VAD coordinators
- 2 perfusionists
- 3 telehealth nurses, 2 clinical specialists
What is the biggest cost in starting a VAD services company?
For Ventricular Assist Device Services, the biggest modeled one-time cost is custom telehealth platform development at $250k. Next come initial VAD controller inventory at $150k and surgical simulation equipment at $85k. The bigger cash drain after launch is recurring: $915k in Year 1 nonclinical payroll, $395k in fixed monthly overhead, malpractice at 60% of revenue, and data and security at 30% of revenue.
Biggest upfront costs
- $250k platform build
- $150k controller inventory
- $85k simulation equipment
- High-acuity clinical setup
Recurring cost drivers
- $915k Year 1 nonclinical payroll
- $395k fixed monthly overhead
- Malpractice at 60% of revenue
- Data and security at 30% of revenue
How much funding is needed to launch VAD services?
For Ventricular Assist Device Services, plan on a funding floor of about $113M, built from $645k of CAPEX and $483k of minimum cash. The Year 1 model shows $1709M revenue, $319k EBITDA, month-2 breakeven, and a 17-month payback. Because reimbursement can lag, use the model to test slower ramp and delayed collections.
Funding floor
- $645k CAPEX starts the build.
- $483k minimum cash covers runway.
- Month 2 is the breakeven point.
- 17 months is the payback window.
Volume ramp
- 2 surgeons, 4 monthly treatments each.
- 4 coordinators, 10 monthly treatments each.
- 2 perfusionists, 8 monthly treatments each.
- 3 nurses at 40 and 2 specialists at 12; test slower ramp and delayed collections.
VAD Services Startup Cost Breakdown Table
Startup cost summary
This table shows startup CAPEX and excluded cash needs for a ventricular assist device services launch, with low, base, and high planning ranges.
| Cost Category | Base Estimate | Main Cost Driver | CAPEX Calculator |
|---|---|---|---|
| Telehealth platform and server infrastructure | $295,000 | Platform build and secure hosting | Yes |
| Surgical simulation and mobile workstations | $145,000 | Training gear and clinician mobility | Yes |
| Initial VAD controller inventory | $150,000 | Starter controller stock and deposit | Yes |
| Clinical office and IT setup | $30,000 | Office network, devices, and setup | Yes |
| Patient education media suite | $25,000 | Patient onboarding content and tools | Yes |
| Operating reserve | $483,000 | Month 6 cash trough and payroll runway | No |
Ventricular Assist Device Services Core Five Startup Costs
Clinical Facility Setup Startup Expense
Facility Access
VAD clinical setup needs procedure access, recovery and monitoring space, infection control, emergency readiness, and accessibility tied to hospital affiliation. Keep owned buildout separate from contracted hospital access. The base model does not list owned facility buildout CAPEX, so do not invent it; the stated support costs are $12k/month for headquarters lease and $60k for mobile clinical workstations.
Cost Inputs
Estimate this cost from lease months, hospital access terms, and any quote for owned renovation. Here, the hard numbers are $12k/month for headquarters space and $60k for mobile workstations. If the service depends on hospital rooms for surgery and recovery, price that access separately so the facility line stays clean.
- Use months of coverage.
- Separate access from buildout.
- Price quotes, not guesses.
Keep It Lean
Use the hospital for clinical space where possible, and keep the owned footprint tight. That avoids loading the startup budget with construction you may not need on day one. The cleanest savings move is to contract access first, then add only the equipment and workstations that support daily patient flow.
- Contract access before building.
- Delay nonessential office space.
- Buy only needed workstations.
Infrastructure Risk
A full VAD service line will carry higher infrastructure cost than the $645k base CAPEX, even before any owned buildout is priced. The risk is underbudgeting space for emergency readiness and long-term monitoring. If the hospital affiliation covers rooms and recovery flow, owned spend stays lighter; if not, the facility bill moves up fast.
Device, Equipment, and Monitoring Startup Expense
Device Stack
Here’s the quick math: a ventricular assist device (VAD) launch needs $85k for surgical simulation gear, $150k for initial controllers, $60k for mobile workstations, and $25k for patient education tools. Add surgical kits and consumables at 80% of Year 1 revenue. Price it by units, coverage months, and contract terms.
What’s Included
This bucket covers controllers, batteries, driveline care supplies, monitoring gear, backup devices, and training stock. Decide each item as CAPEX, inventory, or pass-through based on the care model and supplier contract. Separate one-time deposits from recurring replenishment, and size opening stock from active patients plus spare ratios.
- Count active patients first
- Set backup ratios early
- Map contract payment timing
Cash Control
Use consignment or vendor-managed inventory where you can, especially for controllers and consumables. That keeps cash from sitting in shelves before revenue starts. The big mistake is funding a full year of stock up front when some items can be billed through to the hospital or payer as used. Keep launch cash separate from monthly procurement.
- Push for consignment terms
- Track deposit versus refill
- Buy backup units only as needed
Budget Split
What this estimate hides: device spending is not one clean line. Some costs are upfront equipment, some sit in inventory, and some move as pass-through procurement. So the opening budget should show one-time deposits separately from recurring replacement stock, or you’ll overstate startup cash and understate monthly working capital.
Regulatory, Certification, and Compliance Startup Expense
Compliance Run-Rate
For a VAD program, the base compliance load is $65k per month: $55k for regulatory oversight, $4k for quality assurance monitoring, and $6k for legal and Centers for Medicare & Medicaid Services (CMS) liaison. Treat this as operating or pre-opening readiness spend, not capital equipment.
What It Covers
This cost covers state licensing, accreditation readiness, CMS-related certification prep where needed, policies, protocols, audits, HIPAA compliance, and quality reporting systems. The estimate depends on state, payer, hospital partner, and service model. Here’s the quick math: $65k each month across the readiness window.
- Licensing and accreditation work
- HIPAA and audit controls
- Quality reporting setup
How To Keep It Tight
Use one policy set, one audit calendar, and one reporting stack across sites where rules allow. Start with the partner hospital’s current controls, then fill gaps only where VAD service rules demand it. Avoid paying for duplicate legal review or extra certification work that the payer or facility does not require.
- Reuse hospital policies first
- Limit duplicate audits
- Confirm scope before counsel time
Budget Rule
Budget this as recurring readiness spend, then separate any one-time filing, training, or document build costs from monthly compliance support. What this estimate hides is timing: if onboarding slips, the burn stays at $65k per month while revenue starts later.
Technology and Revenue-Cycle Startup Expense
Platform build
The custom telehealth platform is a one-time build at $250k. It should cover EHR handoffs, device data intake, secure messages, billing rules, coding fields, payer enrollment, and reporting dashboards. Price it from the vendor quote, the number of integrations, and the workflow scope. Keep this separate from monthly software and support.
Core systems
The base tech stack also includes a $45k medical-grade server cluster and $30k of office technology infrastructure. Budget from user count, uptime needs, storage, and device endpoints. This is setup spend, not run-rate. One line worth remembering: build for clinical access first, then pay for speed.
- Count clinician workstations.
- Price backup and redundancy.
- Map device data volume.
Monthly run-rate
Cloud infrastructure maintenance runs at $35k per month, and telehealth platform data and security equal 30% of Year 1 revenue. Separate the one-time setup fee from SaaS, support, cybersecurity, and revenue-cycle work. If claims, coding, and payer enrollment sit in the monthly stack, cash burn climbs fast.
- Split build and support contracts.
- Track months of coverage.
- Match spend to active patients.
Workflow control
Keep the platform tied to clinical and revenue-cycle work: EHR workflows, device data workflows, secure communications, cybersecurity, billing, coding, payer enrollment systems, and reporting dashboards. The cleanest budget split is implementation fees on day one, then monthly SaaS and support, then ongoing revenue-cycle operating costs. That keeps vendor quotes comparable and stops hidden scope creep.
Staffing Readiness and Pre-Opening Payroll Startup Expense
Staffing base
The staffing base is 2 cardiothoracic surgeons, 4 VAD coordinators, 2 perfusionists, 3 telehealth nurses, and 2 clinical specialists. The nonclinical wage base is $915k per year, or about $76.3k per month, before recruiting, credentialing, training, medical director time, billing support, and on-call coverage.
Cost build
This startup cost covers pre-opening payroll, not equipment or buildout. Estimate it by multiplying headcount by loaded monthly pay, then add months of ramp before first full case load. Use separate lines for clinical staff, nonclinical staff, recruiting, credentialing, training, and billing cov erage so the opening budget shows cash timing clearly.
Cost control
Keep this lean by hiring in waves, not all at once. Start the core coverage team first, then add support roles as procedure volume rises. Don’t push payroll into CAPEX; it belongs in pre-opening expense or working capital. The main mistake is understaffing credentialing or on-call coverage, which can slow launch and hurt compliance.
Opening cash need
Plan for staffing cash before revenue catches up. If the program needs several months of overlap for recruiting, credentialing, and training, payroll becomes a working-capital drain fast. The clean budget move is to hold enough cash for the launch team plus medical director time, billing staff, and on-call coverage until utilization stabilizes.
VAD Services Startup Cost Scenarios Table
VAD launch scenarios
Startup cost swings with owned clinical capacity, staffing ramp, and how much of implantation and follow-up stays in-house. More owned control means higher capex, cash need, and compliance burden.
| Scenario | Lean LaunchPartner model | Base LaunchAffiliated model | Full LaunchOwned service line |
|---|---|---|---|
| Launch model | Use a management-only or partner-hospital model with contracted facility access and a light on-site team. | Use the affiliated implantation and follow-up model with the modeled $645,000 capex and a phased cash buffer. | Build a high-acuity service line with owned or expanded clinical infrastructure, emergency readiness, and a faster staffing ramp. |
| Typical setup | Keep implantation access outside the company and focus on coordination, telehealth follow-up, and referrals. | Run core clinical operations in-house, then add staffing and support as volume grows through the month-6 cash trough. | Add more owned capacity for complex cases, broader support coverage, and tighter quality monitoring across the full care path. |
| Cost drivers |
|
|
|
| Planning rangeCAPEX only | Under $645,000Lower cash | $645,000Base case | Above $645,000Higher burn |
| Best fit | Best for teams with contracted hospital access and a partner-owned procedure path. | Best for operators who have hospital alignment, can fund the launch gap, and want a balanced in-house model. | Best for groups that need full control, can carry more working capital, and will keep patient care costs separate from reimbursement assumptions. |
Planning note: These ranges are researched planning assumptions, not exact vendor quotes or reimbursement promises.
Related Products
- Ventricular Assist Device Services Porter's Five Forces Analysis
- Ventricular Assist Device Services BCG Matrix
- Ventricular Assist Device Services Business Model Canvas
- What 5 KPIs Should Ventricular Assist Device Services Track?
- Ventricular Assist Device Services Business Plan Template in Pre-Written Word
- How Increase Ventricular Assist Device Services Profitability?
- What Are The Operating Costs For Ventricular Assist Device Services?
- Ventricular Assist Device Services Financial Model Template in Excel
- How Much VAD Services Owners Can Make From $30M Year 1 Revenue
- How to Open Ventricular Assist Device Services in 9 to 18+ Months
- How To Write A Business Plan To Launch Ventricular Assist Device Services?
- Ventricular Assist Device Services Marketing Mix
- Ventricular Assist Device Services Marketing Plan
- Ventricular Assist Device Services Business Proposal
- Ventricular Assist Device Services PESTEL Analysis
- Ventricular Assist Device Services Pitch Deck Example Editable PPTX
- Ventricular Assist Device Services Business SWOT Analysis
- Ventricular Assist Device Services Value Proposition Canvas
Frequently Asked Questions
The base model needs about $113M before launch stability That is $645k in CAPEX plus $483k of minimum cash needed in Month 6 It excludes separate patient treatment costs, malpractice claim reserves, and any device purchases that are passed through, consigned, or funded under a different contract