 Time to Open6 monthsSetup window
Time to Open6 monthsSetup windowHow To Open A Veterinary Critical Care Hospital With A 24/7 Launch Plan

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open6 monthsSetup window  Launch Sequence6 stagesCompliance first
Launch Sequence6 stagesCompliance first Key BottleneckStaffing gapProvider coverage
Key BottleneckStaffing gapProvider coverage First Revenue StepUrgent casesTriage ready
First Revenue StepUrgent casesTriage ready


You’re opening a high-acuity animal hospital, so the launch plan has to prove clinical readiness before demand arrives This guide covers licensing, ICU setup, staffing, equipment, referrals, and first-revenue planning using a first-year operating model with 4 emergency veterinarians, 2 critical care specialists, and 10 licensed veterinary technicians Use it to sequence the launch, then validate timing, staffing, and case ramp before opening month
Time to Open6 monthsSetup windowLaunch Sequence6 stagesCompliance firstKey BottleneckStaffing gapProvider coverageFirst Revenue StepUrgent casesTriage readyLaunch timeline
Short web summary of the launch plan; the XLSX export has the detailed Gantt Chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8Month 9Month 10
Licensing / compliance
- Permit review
- License filings
- Safety inspections
- Compliance signoff
Facility buildout
- Space layout
- ICU buildout
- Medical gas
- Final walk-through
Equipment / IT
- Equipment quotes
- Imaging install
- Lab setup
- Calibration checks
Staffing / training
- Key hires
- ER roster
- Technician training
- Shift drills
Vendors / SOPs
- Vendor contracts
- SOP drafting
- Triage protocols
- Reorder rules
Marketing / opening
- Referral list
- Outreach launch
- Soft opening
- Ramp-up review
Why test the launch plan before opening month?
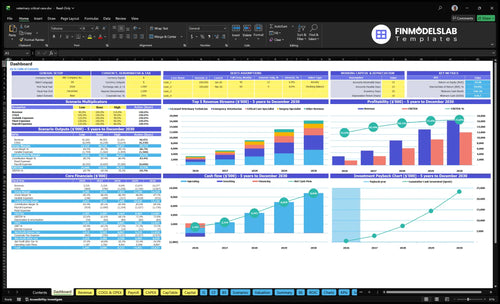
Before opening month, the Veterinary Critical Care Hospital Financial Model Template shows revenue, costs, cash needs, assumptions, and break-even logic.
Financial model highlights
- Year 1 staffing load
- ER and ICU mix
- Cash runway and breakeven
What do you need to open a veterinary critical care hospital?
To open a Veterinary Critical Care Hospital, you need state veterinary compliance, licensed medical leadership, ER-trained staffing, ICU-grade equipment, pharmacy controls, triage workflows, vendor accounts, phone intake, and referral channels; this How To Launch Veterinary Critical Care Hospital? guide fits that checklist. Year 1 readiness means covering 24/7 urgent intake, treatment authorization, ICU monitoring, overnight handoffs, and discharge communication before marketing demand arrives.
Core requirements
- Meet state veterinary facility rules
- Set controlled-substance pharmacy controls
- Install oxygen, monitors, diagnostics
- Build triage and phone intake
Year 1 team
- 4 emergency veterinarians
- 2 critical care specialists
- 1 surgery specialist
- 10 licensed veterinary technicians
How do emergency vet hospitals get patients?
A Veterinary Critical Care Hospital gets patients first from urgent calls and referral handoffs, not broad ads; in Year 1, a realistic outreach assumption is 30% of revenue. For startup budgeting and readiness, see How Much To Start A Veterinary Critical Care Hospital Business?. The win is simple: build trust, answer fast, and send clean medical updates.
Referral network
- Build ties with general practice veterinarians
- Share transfer forms with partners
- Set after-hours communication rules
- Keep phone scripts clear and short
Launch readiness
- Keep local search details accurate
- Accept only staffed services at launch
- Match first cases to equipment on hand
- Use referral trust over broad advertising
What mistakes delay opening a veterinary critical care hospital?
Delays usually come from staffing and process gaps, not the building itself. For a Veterinary Critical Care Hospital, the common launch mistakes are underestimating 24/7 staffing, opening before intensive care unit (ICU) systems are tested, weak referral communication, incomplete controlled-substance logs, and poor overnight handoffs. Test Year 1 capacity against real coverage: 45% ER, 35% critical care, 30% surgery, 50% technician, and 40% imaging—not hoped-for demand.
Big launch risks
- Understaff nights and weekends
- Open before ICU tests pass
- Skip referral call testing
- Miss controlled-substance logs
What to test first
- Run mock triage
- Check oxygen supply
- Audit pharmacy records
- Limit opening-month capacity
Confirm the hospital is ready to open safely before the first patient arrives
Launch readiness checklist
Use this go-live approval checklist to confirm the hospital is ready to open before the launch plan moves into execution.
Compliance
- State vet rules clearedCritical
The hospital cannot open until state veterinary rules are cleared.
- Facility permits confirmedCritical
Any required facility permits should be in hand before patient intake starts.
- DEA registration activeCritical
Controlled drugs need active registration before pharmacy use begins.
- Controlled-drug logs setHigh
Drug logs protect inventory, patient safety, and audit readiness.
- Medical records workflow readyHigh
Records must support treatment notes, transfers, and controlled-drug tracking.
ICU
- ICU monitors installedCritical
ICU monitoring must work before any critical patient admission.
- Oxygen supply testedCritical
Oxygen loss would stop critical care, so test it before opening.
- Ventilators commissionedCritical
Ventilators must be ready before respiratory emergencies arrive.
- Surgical suite readyHigh
The surgical room must be ready for urgent procedures and transfers.
- Imaging uptime verifiedHigh
CT, radiography, and ultrasound need stable uptime for triage and care.
Supplies
- Pharmacy vendor contractedCritical
Medication supply must be secure before the first emergency case.
- Consumables reorder points setHigh
Supplies and consumables need reorder rules to avoid stockouts.
- Waste pickup scheduledHigh
Biohazard waste must leave the site on a fixed, compliant schedule.
- Lab service contract liveHigh
Lab turnaround times affect diagnosis speed and treatment decisions.
Staffing
- Emergency vet roster filledCritical
Year 1 needs 4 emergency veterinarians to match the plan.
- Critical care coverage filledCritical
Year 1 needs 2 critical care specialists for ICU coverage.
- Surgery coverage filledHigh
Year 1 needs 1 surgery specialist to cover urgent procedures.
- Technician roster filledCritical
Year 1 calls for 10 licensed veterinary technicians at opening.
- Night shift protocol setCritical
Missing overnight rules are a launch blocker for emergency care.
Referrals
- Transfer forms approvedHigh
Transfer forms help referring clinics hand off cases without delay.
- Intake phone liveCritical
Direct calls are a first-revenue path, so the phone line must work.
- Search visibility liveMedium
Search visibility helps pet owners and clinics find the hospital fast.
- Emergency triage script readyCritical
A triage script keeps urgent cases moving to the right care path.
- After-hours callback rules setHigh
After-hours rules reduce missed emergencies and staff confusion.
Finance
- Cash runway modeledCritical
Minimum cash hits $611k in Month 2, so runway needs to cover the early dip.
- Year 1 margin reviewedHigh
Year 1 revenue is $3.235M and EBITDA is $1.702M, so the opening plan must hold margin.
- Opening-month burn coveredCritical
Lease, payroll, and equipment timing can still pressure cash in Month 1.
- Go-live signoff completeCritical
Final signoff should confirm staff, systems, vendors, and referral flow are ready.
Want the six drivers that decide launch readiness?
1Clinical Staffing Coverage
18 core staffSigned overnight and weekend shifts, backed by 4 ER vets, 2 critical care specialists, and 10 techs, keep referrals safe.
2Facility ICU Buildout
6-step flowA tested arrival-to-ICU path prevents unstable pets from getting stuck in a pretty but weak layout.
3Licensing Compliance
License gateDocumented ordering, storage, and wasting of controlled drugs keeps day-one care legal and inspections cleaner.
4Equipment Readiness
85/60/15Working monitors, oxygen, labs, and service agreements cut transfers caused by missing tools.
5Referral Intake
30% revA live urgent-call workflow and clear transfer updates turn referral trust into steadier first cases.
6Operating Runway Controls
$611K floorMock cases that finish estimates, drugs, and handoffs help hold cash burn as volume ramps.
Clinical Staffing Coverage
Clinical Staffing Coverage
24/7 emergency care only opens on time if the shifts are already covered. This hospital needs secured veterinarians, critical care coverage, surgery access, licensed veterinary technicians, assistants, front desk triage support, and leadership coverage before demand arrives. The readiness signal is a signed shift schedule with overnight and weekend coverage in place.
Year 1 source plan calls for 4 emergency veterinarians, 2 critical care specialists, 1 surgery specialist, 10 licensed veterinary technicians, and 1 diagnostic imaging specialist. If referrals start before these roles are locked, the hospital can end up declining cases, slowing triage, and delaying treatment starts. No schedule, no launch.
Lock the shift grid before referrals
Build the launch plan around actual names, not open roles. Verify who covers triage, who covers ICU, who handles surgery, and who leads overnight handoffs. Then test the schedule against the first week of demand, especially overnight and weekend coverage. The goal is simple: the first call should reach a staffed team, not a promise.
- Confirm 24/7 coverage by role.
- Match skills to each shift.
- Document handoffs before opening day.
- Hold referrals until coverage is signed.
What this hides: staffing gaps do not just slow care, they can force case declines and strain the first-day patient flow. If the schedule is thin, the hospital may open with capacity on paper but not enough live coverage to safely receive unstable pets.
1
Facility And ICU Buildout Readiness
ICU Buildout Readiness
A 24/7 critical care hospital cannot open on time if the room layout looks finished but cannot move unstable pets fast. The buildout has to support arrival to discharge: triage, diagnostics, oxygen, ICU monitoring, procedure, and release, with exam rooms, isolation space, ICU cages, and imaging placed for clean flow.
The big risks are medical gas, electrical load, equipment placement, waste flow, and staff line of sight. If those fail, day one turns into delays, case transfers, and a site that is attractive on paper but not usable for critical patients.
Test the Patient Path
Before opening, walk a real emergency through the space and document every handoff. Confirm gas, power, drains, suction, storage, and imaging placement are ready for the services you will offer at launch. One clean floor plan is not enough; the team has to prove it works under pressure.
- Map lobby to discharge.
- Check line of sight at beds.
- Verify oxygen and power loads.
- Stage waste and clean routes.
- Run mock cases before move-in.
If buildout finishes before utility signoff, the hospital still cannot receive unstable patients. That pushes the opening date, burns cash, and can force a soft launch with fewer ICU beds and less procedure capacity than planned.
2
Licensing And Controlled-Substance Compliance
Licensing and Drug Control
A critical care hospital cannot open on time if the state veterinary board approvals, facility permits where required, and individual veterinarian licenses are not in place. If the hospital will use controlled drugs, DEA registration, secure storage, drug logs, and pharmacy procedures must be ready before the first patient arrives, or opening-day treatment can get blocked.
This driver also covers medical records, OSHA practices, and biohazard procedures. The readiness test is simple: one person is clearly assigned to order, receive, dispense, waste, and reconcile controlled medications. If that responsibility is vague, inspections get messy and day-one care slows down.
Lock the Compliance Chain
Map every approval and control step to a named owner before launch. Verify the state-specific license path, confirm whether a facility permit is required, and check that controlled-drug handling is documented from ordering through reconciliation. One missed approval can push back opening and force cases to be turned away.
Use a launch checklist with licenses, permits, drug logs, secure storage, medical records, and biohazard procedures. Test the process as if an inspector walked in on day one. Clean paperwork and tight drug control are what keep treatment legal and the first inspection clean.
3
Equipment And Vendor Readiness
Equipment and Vendor Readiness
For a 24/7 emergency veterinary hospital, the launch date only works if the core tools are on site, installed, and tested. Monitors, infusion pumps, oxygen systems, lab diagnostics, and pharmacy stock have to match the services you promise on day one; if ventilatory support or radiology is sold, those systems must also be live, not just ordered.
The setup is not just buying gear. Readiness shows up in stocked supplies, working diagnostics, tested oxygen, and service agreements in place. The Year 1 variable assumptions point to 85% medical supplies, 60% pharmaceuticals, and 15% waste disposal, so weak vendor setup can push case transfers when a needed tool, drug, or service is missing.
Lock the launch scope to the equipment in hand
Build the opening checklist around the exact services you can support on day one. Here’s the quick test: if a pet arrives unstable, can you monitor, start fluids, give oxygen, run diagnostics, and keep the case in-house without waiting on a missing delivery or repair? If the answer is no, the service should wait.
- Confirm install dates before hiring ramps.
- Test oxygen and backup power first.
- Stock fast-moving consumables in full.
- Get service agreements in writing.
- Match inventory to launch services.
- Set reorder points before opening.
One broken supply chain link can turn a treatable emergency into a transfer. That hurts patient flow, slows first revenue, and creates avoidable stress for staff and owners on opening week.
4
Referral Network And Patient Intake
Referral Intake Readiness
Day-one case flow depends on whether nearby clinics know exactly when and how to send emergencies. Referral outreach is assumed to drive 30% of year-one revenue, so the hospital cannot open on time with vague handoffs, broken call coverage, or an incomplete website. A live intake path has to capture history, set expectations, and route urgent cases fast.
The key dependency is clinical capacity matching what you promise. If the hospital advertises ICU, surgery, or after-hours care but cannot accept those cases immediately, trust drops fast. Slow callbacks and unclear transfer updates push primary care veterinarians to send the next case elsewhere. One missed handoff can cost more than one lost patient.
Build the referral path before opening
Set up the intake workflow before the first case arrives. Confirm the phone script, transfer form, website hours, local search listings, and after-hours backup so the team can answer urgent calls without scrambling. That is the readiness signal: a live phone workflow that can take history, set expectations, and route the case to the right clinician.
- Test urgent-call routing end to end.
- Match intake hours to real staffing.
- Document transfer steps and callbacks.
- Keep website services fully accurate.
- Assign one owner for referral updates.
Run mock calls before launch and check that the hospital can accept the case level it promises. If callbacks slip or updates stall, referral retention weakens quickly. Fast, clear communication steadies the first cases and protects the local reputation that year-one volume depends on.
5
Operating Protocols And Runway Controls
Operating Protocols And Runway Controls
For an emergency vet hospital, launch speed depends on whether staff can run a full case without gaps. The day-one test is simple: a mock patient moves from call to triage, estimate, treatment authorization, drugs, discharge, and overnight handoff without missing a step. If that flow breaks, opening on time gets risky and the first cases slow down.
This driver also protects cash runway, which means the cash left before you need more money. The model assumes 45% ER, 35% critical care, 30% surgery, 50% technician, and 40% imaging capacity in Year 1. That makes the opening pace matter, because staffing burn should rise only as demand proves it can support the team.
Mock Cases Before Opening
Build the SOPs first: triage script, treatment approval form, estimate template, discharge sheet, overnight handoff log, and inventory count process. Then run mock cases with the real phone flow, drug access, and charting steps. One clean test from call to discharge is the readiness signal; if approvals, drugs, or handoffs are missed, the opening plan is not ready.
Keep the ramp controlled. Match hiring and schedule load to the stated Year 1 capacity assumptions, and do not staff ahead of demand unless the case flow supports it. That helps avoid cash surprises, because fixed labor and stocked supplies hit before revenue does. Track the first weeks by case volume, handoff errors, and supply use, then tighten the process before adding more shifts.
- Test call-to-discharge with real scripts.
- Assign one owner per approval.
- Reconcile drugs at each handoff.
- Set inventory par levels before open.
- Ramp shifts only with case demand.
6
Related Products
- Veterinary Critical Care Hospital Porter's Five Forces Analysis
- Veterinary Critical Care Hospital BCG Matrix
- Veterinary Critical Care Hospital Business Model Canvas
- What 5 KPIs Matter For Veterinary Critical Care Hospital Business?
- Veterinary Critical Care Hospital Business Plan Template in Pre-Written Word
- How Increase Veterinary Critical Care Hospital Profitability?
- What Does It Cost To Run A Veterinary Critical Care Hospital?
- Veterinary Critical Care Hospital Startup Costs: $565K+ CAPEX
- Veterinary Critical Care Hospital Financial Model Template in Excel
- How Much Veterinary Critical Care Hospital Owners Make at $2696K/Month
- How Do I Write A Business Plan For A Veterinary Critical Care Hospital?
- Veterinary Critical Care Hospital Marketing Mix
- Veterinary Critical Care Hospital Marketing Plan
- Veterinary Critical Care Hospital Business Proposal
- Veterinary Critical Care Hospital PESTEL Analysis
- Veterinary Critical Care Hospital Pitch Deck Example Editable PPTX
- Veterinary Critical Care Hospital Business SWOT Analysis
- Veterinary Critical Care Hospital Value Proposition Canvas
Frequently Asked Questions
Start with clinical readiness, not ads or décor Confirm state veterinary requirements, facility readiness, controlled-substance procedures, and a staffing plan The Year 1 planning case uses 4 emergency veterinarians, 2 critical care specialists, and 10 licensed veterinary technicians Then test triage, oxygen, diagnostics, pharmacy, referral intake, and overnight handoffs before the first urgent case