 Owner income$240k
Owner income$240kHow Much Veterinary Critical Care Hospital Owners Make at $2696K/Month

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$240k  Net margin52.6%-73.8%
Net margin52.6%-73.8% Revenue for target pay$325k-$457k
Revenue for target pay$325k-$457k Business difficultyHard
Business difficultyHard


You’re modeling a high-stakes hospital, not a small daytime clinic, so owner income depends on volume, staffing, debt, and reserves This page uses a five-year planning model with $269,600 monthly Year 1 revenue, $136M monthly Year 5 revenue, listed payroll, direct costs, fixed overhead, and scenario logic, but it excludes tax advice, guaranteed distributions, individual veterinarian wages, and one-off acquisition outcomes
Owner income$240kNet margin52.6%-73.8%Revenue for target pay$325k-$457kBusiness difficultyHardWant to test your owner pay?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
Want to check the full hospital model?
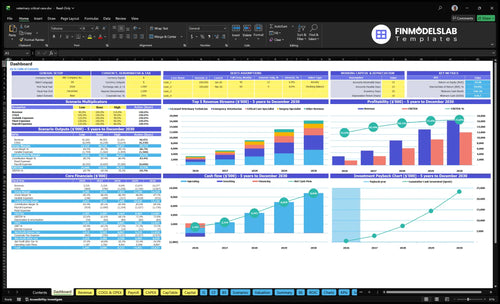
The Veterinary Critical Care Hospital Financial Model Template shows revenue, operating profit, owner salary, cash cushion, and pay assumptions so you can open the model and test it fast.
Owner-income model highlights
- Dashboard income first
- Revenue and margin charts
- Scenario testing by payroll
How do emergency vet hospital labor costs affect profit margin?
Labor is the main margin swing factor for a Veterinary Critical Care Hospital because 24/7 coverage needs doctors, critical care technicians, reception, triage, and relief staff; see How Much To Start A Veterinary Critical Care Hospital Business?. Year 1 payroll is $795,000 a year, or about $66,250 a month, before any separate pay for revenue-producing veterinarians not shown in the wage table. Staffing scales from 4 to 12 emergency veterinarians and 10 to 26 licensed veterinary technicians, so if coverage grows faster than case volume, owner take-home compresses fast.
Labor pressure points
- $795,000 Year 1 payroll
- 24/7 coverage drives staffing
- 4 to 12 emergency veterinarians
- 10 to 26 licensed veterinary technicians
Margin guardrails
- Match coverage to case volume
- Watch relief shifts closely
- Do not understaff critical care
- Protect owner take-home from overspend
How does owner role change 24/7 veterinary hospital profitability?
For a 24/7 Veterinary Critical Care Hospital, the owner’s role can make or break profit: an owner-clinician can take the $240,000 Medical Director salary and avoid hiring that role, while an absentee owner still has to carry it as a cost before any distributions. The money work then shifts to scheduling, referral flow, pricing, collections, and capacity; if the owner covers too many clinical shifts, burnout risk climbs fast because night coverage, technician ratios, and admin depth all limit income.
Owner-clinician model
- $240,000 can stay in-house.
- Skip a hired medical director.
- Focus on referral flow.
- Manage pricing and collections.
Absentee owner model
- Keep $240,000 as a cost.
- Clinical coverage stays tight.
- Night shifts cap owner income.
- Burnout risk rises with overload.
How much revenue does an emergency vet hospital need to pay the owner?
Veterinary Critical Care Hospital needs about $269,600 in monthly revenue in the Year 1 model, but that is not the owner’s pay. After $51,224 in direct and variable costs and $94,850 in payroll plus fixed overhead, the model leaves about $123,526 before debt, reserves, taxes, and distributions. So the real answer is: revenue must first cover operations, and only the leftover can flow to the owner.
Revenue base
- $269,600 monthly Year 1 revenue
- Built from emergency and critical care
- Includes surgery, technician, imaging
- Fee-for-service drives the model
Owner payout math
- $51,224 direct and variable costs
- $94,850 payroll and fixed overhead
- $123,526 left before other uses
- Owner pay comes after those claims
Want to see the six income drivers?
1
$270K-$1.36M/moCase Volume
More emergency cases spread the $28.6K fixed load and lift owner take-home before taxes and reserves.
2
$350-$2.6KCase Mix
A heavier share of surgery and critical care raises invoice size fast, so income moves up without the same jump in visits.
3
18-46 FTEStaffing Load
Hiring to the right FTE level keeps capacity high, but overstaffing can eat EBITDA before demand catches up.
4
35%-70%ICU Use
Higher ICU use keeps beds, monitors, and critical care time earning instead of sitting idle.
5
$28.6K/moFixed Overhead
The lease, utilities, insurance, software, and cleaning bill must be covered first, so this base cost sets the cash floor.
6
14.5%Supply Cost
Medical supplies, medications, waste, and outreach are the easiest cost lines to trim, and small cuts flow straight to take-home.
Veterinary Critical Care Hospital Core Six Income Drivers
Emergency Case Volume And Intake
Emergency Case Volume
This driver turns 24/7 coverage into billable work. At 120 monthly treatments per emergency veterinarian, 4 doctors in Year 1 at 45% utilization imply about 216 treatments a month; at 12 doctors in Year 5 and 75% utilization, that rises to about 1,080. More intake lifts revenue and spreads fixed payroll, but only if the team can safely treat the cases.
Nights, weekends, holidays, referral ties, and local competition decide how many calls become patients. More calls do not add income if triage is slow, doctor time is full, or ICU space is packed. One clean rule: volume helps only when staff, cages, and monitoring can absorb it without cutting care quality.
Track Intake by Source and Time
Measure calls, consults, admits, and turn-away reasons by hour, especially after 5 p.m., weekends, and holidays. Compare referral cases against walk-ins, then watch how many reach treatment. If conversion rises but capacity stays tight, add staffed hours before chasing more demand. That protects cash flow and keeps owner pay tied to real output, not lost calls.
Set trigger points for triage, doctor, and ICU load. When any one hits its cap, extra demand should route to a waitlist, transfer partner, or added shift. The key is not more calls; it is usable case volume that the team can handle without overtime spikes or rushed care.
- Track call-to-admit conversion.
- Split nights, weekends, holidays.
- Log turn-aways by capacity.
- Match staffing to booked cases.
- Watch ICU load before scaling.
1
Average Invoice And Case Mix
Average Invoice And Case Mix
This driver is the average billed amount per case, shaped by how many pets need emergency visits, critical care, surgery, imaging, or technician services. In Year 1, prices run from $120 technician services and $350 emergency visits to $850 critical care, $600 imaging, and $2,200 surgery. By Year 5, those rise to $140, $410, $970, $680, and $2,600.
Higher-acuity cases can lift revenue per case, but they also use more supplies, drugs, lab work, imaging, and staff time. So the owner only wins if collections and care standards hold. If clients cannot approve treatment or pay deposits, the invoice may look strong while cash flow and owner draw stay weak.
Track Cash, Not Just Billings
Measure case mix, average invoice, direct cost per case, and collection rate together. A richer mix should raise contribution margin, not just top-line sales. If surgery and critical care are growing, also watch imaging use, lab spend, technician hours, and write-offs so you can see whether extra acuity is actually adding profit.
- Track billed versus collected revenue.
- Review discounts and write-offs monthly.
- Use deposits on high-ticket cases.
- Require payment approval before discharge.
One clean rule: if average invoice rises but bad debt, overtime, or supply cost rises faster, owner pay stalls. The best case mix is the one that improves cash collected per case without breaking care quality or slowing treatment approval.
2
Clinical Staffing And Coverage Model
Clinical Staffing Cost
This driver is the payroll needed to keep a 24/7 critical care hospital safe and open. As coverage scales from 4 to 12 emergency veterinarians, 2 to 4 critical care specialists, 1 to 2 surgery specialists, 10 to 26 licensed veterinary technicians, and 1 to 2 imaging specialists, support payroll rises from $795,000 to $1,331,000 a year.
That is a $536,000 jump, or about $44,667 a month, before relief doctors, overtime, and benefits. Payroll protects care quality, but if case flow does not support the added headcount, it can absorb owner distributions fast and leave less cash for debt, taxes, and profit draw.
Staff to Case Flow
Estimate staffing from actual intake by shift, not from hoped-for revenue. The inputs are doctor count, specialist count, technician count, relief coverage, overtime, benefits, and cases by daypart. Here’s the quick math: every added paid hour only helps if it creates more billable cases or safer throughput.
- Track cases per doctor.
- Track overtime by role.
- Track relief-doctor spend.
- Track paid hours versus used hours.
If nights, weekends, and holidays run hot, add coverage there first. If the schedule is thin, freeze hiring and trim overtime before adding full-time staff. What this estimate hides: benefits and last-minute relief shifts can push labor above plan even when headcount looks right on paper.
3
ICU Capacity And Utilization
ICU Utilization
ICU utilization is the share of cages, monitoring slots, specialist hours, technician time, and imaging time that is actually used for admitted pets. In this model, critical care specialist capacity rises from 35% in Year 1 to 70% in Year 5, technician capacity from 50% to 80%, and imaging from 40% to 70%, so more used hours support more billable high-value care and better owner profit.
The ceiling is real: oxygen cages, monitoring equipment, treatment space, and length of stay can fill up before demand does. Here’s the quick math: if ICU is full but staff or cages are not, revenue is left on the table; if you push past safe capacity, outcomes slip and refunds, write-offs, and staff burnout can hurt cash flow and distributions.
Track Bed Turns and Staff Load
Measure occupancy by shift, average length of stay, and the ratio of specialist, technician, and imaging hours used to hours available. Those are the inputs that show whether the ICU can take more cases without breaking care standards. If demand is strong but one piece hits 100%, that is the bottleneck, not the market.
- Track occupied cage hours daily.
- Match staffing to admission mix.
- Watch imaging queue time.
- Limit unsafe overcapacity.
Use these numbers to forecast case intake and owner draw. Higher utilization lifts revenue only when the ICU can safely absorb the work, so the goal is productive fill, not max fill. If length of stay rises without extra capacity, the hospital can look busy while profit and cash conversion weaken.
4
Fixed Overhead And Equipment
Fixed Overhead And Equipment
Fixed costs set the break-even floor before owner pay. Here, the monthly base is $28,600 from $18,000 lease, $2,500 utilities, $3,200 equipment maintenance, $1,800 liability insurance, $900 software, and $2,200 cleaning. That is $343,200 a year before any draw, so slower months still burn cash even when case volume dips.
The equipment burden is also heavy: a $250,000 CT scanning system plus an $85,000 digital radiography unit means $335,000 in visible capital needs. One line matters most: higher volume spreads fixed costs across more cases. If monthly cases rise, overhead per case falls; if intake slows, rent, upkeep, and insurance squeeze profit fast.
Track Fixed Cost Per Case
Measure fixed overhead per case every month: $28,600 ÷ monthly cases. At 100 cases, fixed overhead is $286 per case; at 200 cases, it drops to $143. That is the quick check for whether volume is high enough to support owner pay after staffing and supplies.
Track these items together: lease, utilities, equipment upkeep, insurance, and equipment downtime. If case volume softens, cut waste fast and delay owner draws before missing bills. Keep a separate reserve for large equipment replacement or financing, because a busy month only helps if the hospital can keep the scanner and imaging unit working.
- Review overhead per case monthly
- Watch equipment downtime and repairs
- Hold cash for lease and insurance
5
Pricing, Collections, And Payment Policy
Realized Revenue From Collections
Emergency hospitals don't pay staff with invoice totals; they pay with collected cash. If you bill $350 for a visit, $850 for critical care, or $2,200 for surgery, the real driver is what gets collected after deposits, pet insurance, third-party financing, write-offs, and compassionate discounts. Weak collections can cut owner pay even when case volume looks strong.
The inputs are written estimates, payment timing, bad debt, and discount policy. A clear workflow improves cash flow, but it should not turn pricing into the only lever. In emergency care, clients may be under stress and unable to pay right away, so the collections policy has to support care standards and staff safety.
Tighten Payment Workflow
Track invoice revenue, cash collected, discounts, write-offs, and days to collect on every case. That shows whether a $350 exam or $600 imaging job is actually funding the hospital. If you see more unpaid balances, tighten estimate approval and deposit rules before treatment starts.
- Collect deposits at intake
- Use written estimates early
- Separate insurance and financing
- Log write-offs monthly
- Set a clear discount policy
Use one written rule for compassionate discounts and one for unpaid balances. That keeps decisions consistent, reduces staff conflict, and makes realized revenue easier to forecast. If the hospital expects more high-acuity cases, collections discipline matters more, because larger bills only help income when they turn into cash.
6
Compare low, base, and high owner-income scenarios
Owner income scenarios
Owner income climbs as utilization fills emergency, ICU, surgery, and imaging capacity, but payroll and fixed costs stay heavy. Listed-cost operating profit is revenue after direct, variable, fixed, and payroll costs.
| Scenario | Low CaseLow Case | Base CaseBase Case | High CaseHigh Case |
|---|---|---|---|
| Launch model | Year 1 ramp keeps owner income on the low side while utilization climbs. | Year 3 scale lifts owner income as volume and pricing both step up. | Year 5 maturity produces the strongest owner-income path as the hospital runs near full service-line capacity. |
| Typical setup | About $269,600 monthly revenue, 30% to 50% utilization, $28,600 fixed overhead, and about $66,250 listed monthly payroll support a modest take-home path. | About $753,720 monthly revenue, 50% to 70% utilization, and a larger specialist mix push listed-cost operating profit to about $505,484 monthly. | About $1.36M monthly revenue, 65% to 80% utilization, and the model's strongest EBITDA path point to roughly $1.0M monthly before debt service, reserves, taxes, and reinvestment. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $123,526/moLow Case | $505,484/moBase Case | $1.0M/moHigh Case |
| Best fit | Use this for a cautious Year 1 ramp and to test early cash flow. | Use this as the core planning case for steady mid-scale hospital operations. | Use this to test upside if case flow stays strong and the hospital keeps reinvesting. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Veterinary Critical Care Hospital Porter's Five Forces Analysis
- Veterinary Critical Care Hospital BCG Matrix
- Veterinary Critical Care Hospital Business Model Canvas
- What 5 KPIs Matter For Veterinary Critical Care Hospital Business?
- Veterinary Critical Care Hospital Business Plan Template in Pre-Written Word
- How Increase Veterinary Critical Care Hospital Profitability?
- What Does It Cost To Run A Veterinary Critical Care Hospital?
- Veterinary Critical Care Hospital Startup Costs: $565K+ CAPEX
- Veterinary Critical Care Hospital Financial Model Template in Excel
- How To Open A Veterinary Critical Care Hospital With A 24/7 Launch Plan
- How Do I Write A Business Plan For A Veterinary Critical Care Hospital?
- Veterinary Critical Care Hospital Marketing Mix
- Veterinary Critical Care Hospital Marketing Plan
- Veterinary Critical Care Hospital Business Proposal
- Veterinary Critical Care Hospital PESTEL Analysis
- Veterinary Critical Care Hospital Pitch Deck Example Editable PPTX
- Veterinary Critical Care Hospital Business SWOT Analysis
- Veterinary Critical Care Hospital Value Proposition Canvas
Frequently Asked Questions
The clearest modeled pay figure is the $240,000 annual Medical Director salary if the owner fills that role Any extra distribution comes after payroll, $28,600 monthly fixed overhead, direct costs, debt service, reserves, and taxes The listed-cost operating profit is about $148M in Year 1, but it is not the same as owner take-home