 Time to Open6-12 monthsOpening prep
Time to Open6-12 monthsOpening prepHow To Start A Virtual Surgery Simulation Training Business In 6-12 Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open6-12 monthsOpening prep  Launch Sequence5 stagesValidate first
Launch Sequence5 stagesValidate first Key BottleneckContent approvalClinical review
Key BottleneckContent approvalClinical review First Revenue StepPaid pilotDeposit received
First Revenue StepPaid pilotDeposit received


To launch a VR surgical training business, validate one clinical use case, build or license the first simulation module, secure medical advisor review, test headset delivery, and run paid pilots with hospitals, medical schools, or residency programs A realistic planning window is 6 to 12 months, with the main bottleneck being credible surgical content and institutional adoption The researched model assumes Year 1 pricing of $2,500 per month for academic customers, $5,000 for hospitals, and $12,000 for device partners, plus one-time setup fees Treat those as planning assumptions to test through pilots, not guaranteed revenue
Time to Open6-12 monthsOpening prepLaunch Sequence5 stagesValidate firstKey BottleneckContent approvalClinical reviewFirst Revenue StepPaid pilotDeposit receivedLaunch timeline
This is a short web summary of the launch plan; the XLSX export holds the detailed Gantt chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8Month 9Month 10Month 11Month 12
Clinical content
- Procedure scope review
- Learning outcomes map
- Module storyboard
- Expert review
VR technology
- Hardware spec
- Prototype build
- Stress testing
- Latency tuning
Compliance
- Privacy review
- Liability review
- Consent workflow
- Policy signoff
Pilot partnerships
- Target list
- Outreach calls
- Pilot terms
- Schedule pilots
Staffing training
- Core hires
- SME onboarding
- Instructor training
- Support playbooks
Commercial launch
- Pricing package
- Sales deck
- Lead pipeline
- Go-live checklist
Want to pressure-test the launch plan before spending?
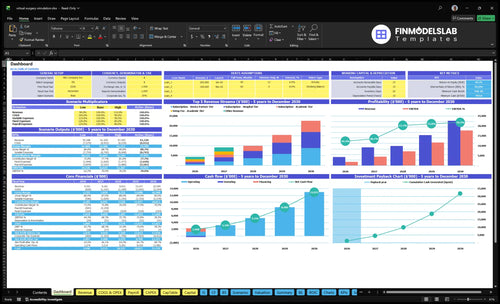
Open the Virtual Surgery Simulation Training Financial Model Template to test launch timing, revenue ramp, staffing, runway, and break-even fast.
Financial model highlights
- 60/30/10 Year 1 mix
- $2,500 to $12,000 tiers
- $15k to $50k fees
- CAC starts at $1,500
- Pilots to contracts
What mistakes derail a VR surgical training launch?
The biggest launch mistakes are clinical claims before validation, slow hospital sales, weak instructor support, and messy hardware logistics. For Virtual Surgery Simulation Training, lock advisor review, training-only claims, privacy rules, support workflows, and pilot success metrics before opening up. With $27,000 in monthly fixed overhead, 23% Year 1 revenue-linked costs, and $1,500 CAC, a long onboarding cycle can crush pilot conversion fast.
Launch mistakes
- Skip clinical validation first
- Undershoot hospital sales cycles
- Understaff instructor support
- Ignore hardware setup and latency
What to lock
- Use advisor review before launch
- Sell training-only, not outcome claims
- Set privacy and support workflows
- Define pilot success metrics early
How do you get customers for VR surgical training?
Get first customers by selling paid pilots to residency programs, medical schools, simulation centers, surgical departments, device companies, and continuing medical education partners. Start with one procedure module, a clear assessment rubric, and a pilot price test; if you need launch-cost context, How Much To Launch Virtual Surgery Simulation Training Business? helps frame the spend.
Talk to the economic buyer, the clinical champion, and the simulation center director. In year 1, aim for a sales mix of 60% academic, 30% hospital, and 10% device partner customers, then prove value with usage, completion, assessment data, and instructor feedback.
Early buyers
- Residency programs buy outcomes.
- Medical schools need repeatable practice.
- Simulation centers want measurable gains.
- Surgical departments want safer training.
Pilot to sale
- Test $15,000 to $50,000 fees.
- Test $2,500 to $12,000 monthly plans.
- Use one module and rubric.
- Show usage, completion, and feedback.
How long does it take to launch a VR surgical training company?
Launching a Virtual Surgery Simulation Training company usually takes 6 to 12 months. That window depends on clinical review, scenario build, interaction testing, headset logistics, hospital procurement, and pilot scheduling, so don’t promise an exact launch date too early.
Build phase
- Validate procedure choice first.
- Confirm learning outcomes early.
- Build the minimum viable module.
- Test headset delivery and setup.
Launch phase
- Sign pilots with institutions.
- Train instructors before rollout.
- Prepare renewal or contract conversion.
- Expect delays from legal, haptics, or procurement.
Confirm the business is ready to serve clinical training customers
Launch readiness checklist
Use this go-live approval checklist before opening the virtual surgery simulation training business.
Regulatory
- Training-only claim approvedCritical
Prevents clinical claims from outrunning the product; FDA clearance is not assumed for training software.
- Clinical rubric signed offCritical
A scoring rubric is the first blocker; without it, pilot feedback stays subjective.
- Patient-data flow reviewedHigh
HIPAA exposure depends on patient data use, so map data paths before launch.
- Liability coverage boundCritical
Coverage should be active before demos, pilots, or headset deployment.
Entity
- Entity setup completeCritical
You need a clear legal home before contracts, payroll, and vendor deposits.
- Advisor agreements executedHigh
Advisor terms keep clinical and technical guidance usable in diligence.
- Medical director authority setHigh
One person should own medical signoff so scope stays tight.
- IP ownership terms signedHigh
IP terms prevent disputes over scenarios, code, and assets.
Curriculum
- Curriculum review approvedCritical
Curriculum review keeps the content tied to training goals and skill levels.
- Simulation modules pass QACritical
QA should catch broken scenarios before the first pilot session.
- Software stability confirmedCritical
Stable builds reduce demo failures and support load.
- Instructor support guide readyHigh
Instructor guides keep handoffs and feedback consistent.
Hardware
- Headset deployment testedCritical
Unstable hardware is a launch blocker, so test each headset in demo use.
- Haptic kits work in demoHigh
Prototype haptics must work in live sessions, not just in the lab.
- Backup hardware securedHigh
Backup gear protects pilot days from avoidable failures.
- Hosting and storage confirmedMedium
Storage and hosting need enough room for media and session data.
Pilot
- Pilot buyer signedCritical
No pilot buyer means no first revenue, so lock one before go-live.
- Pilot agreement executedCritical
Pilot terms should define scope, success criteria, and fees.
- Sales collateral approvedHigh
Sales assets must explain the training-only offer in plain terms.
- Billing path testedHigh
A working billing path avoids delays when the pilot converts.
- Onboarding workflow testedHigh
Onboarding should move a buyer from signed to active without confusion.
Finance
- Runway covers launch burnCritical
Use the model to cover $27k monthly fixed overhead and Year 1 salary base of $815k.
- Model assumptions reviewedHigh
Check $27k fixed overhead, $815k salary base, 23% revenue-linked costs, and $150k marketing budget.
- Go-live signoff completeCritical
Go-live should wait until cash, pricing, risk, and launch ownership are signed off.
Which launch drivers matter most?
1Clinical Validation
6-12 moSurgeon-reviewed flow and scoring make the product look like training, so pilots clear the first buyer trust test.
2Simulation Content
1 moduleA single sellable module speeds pilot setup and keeps pricing tied to real curriculum use.
3VR Reliability
StableStable headset setup and low latency cut demo failures and reduce support escalations.
4Compliance Ready
Legal gateLegal review, disclaimers, and insurance keep procurement moving and avoid approval delays.
5Pilot Pipeline
$1.5K CACNamed champions and a clear pilot scope turn interest into paid pilots faster.
6Support Ops
1 CSMSupport and onboarding keep instructors active, so pilots finish and renewals start from proof, not confusion.
Clinical Validation And Learning Outcomes
Clinical Validation
Clinical validation is the first launch gate for this VR surgical training business. If surgeons do not review the procedure flow, curriculum fit, scoring, and learning outcomes, buyers may see it as entertainment, not training. That slows pilot approval and can push back opening because the product is live, but not credible enough to sell.
The key dependency is proof from real clinical input before sales expansion. A weak validation package can stall procurement, weaken first-day adoption, and delay paid department contracts. In a hospital sale, trust comes first; without it, even a polished demo can sit in review.
Build the proof file
Start with 4 items: recruit medical advisors, map procedure steps, define assessment rubrics, and test with target learners. Keep the first validation set tight and documented so it is easy for surgeons and simulation directors to review. That gives you something concrete to show before you ask for a pilot or a budget line.
Write down what changed, what improved, and what score was used. If the learning outcome is not documented, the buyer will ask for more proof and the launch slows. The goal is simple: make the training look like training on day one, not a demo that still needs explanation.
1
- Recruit advisors first for surgeon review.
- Map every procedure step before build lock.
- Define one scoring rubric for learner performance.
- Test with target learners before broad sales.
- Document outcomes for pilot approval packets.
- Use the same evidence in every procurement meeting.
Simulation Content Development
Ship One Sellable Module First
Opening on time depends on one sellable module that works end to end. For virtual surgery training, that means a single procedure flow with realistic scenarios, tested interactions, and curriculum fit. If the first module is half-finished, pilot sites cannot schedule training, price the offer, or use it on day one.
The main trap is building a full content library before demand is proven. Get advisor review before broad release, and only add haptics if the first module still holds up. Weak content pushes pilot dates, raises rework, and turns a training product into a demo that can’t support live classes.
Lock The First Module Before Scaling
Pick one procedure with clear curriculum demand, then map every step, define the scoring rubric, and test interaction quality with target learners. Keep the scope narrow enough to install, teach, and sell without extra custom work. That gives you faster pilot readiness, simpler onboarding, and cleaner pricing for academic, hospital, or device partner use.
- Select one procedure first.
- Test the full flow before release.
- Review content with advisors.
- Expand only after pilot demand.
2
VR Platform Reliability And Hardware Setup
VR Setup Readiness
This launch gate decides whether the platform works in a real classroom or fails on setup day. The key dependency is customer environment readiness: headset compatibility, network access, room layout, and device settings. If the first session needs ad hoc fixes, the pilot can stall before users even judge the clinical value.
Readiness means stable software, tested headset deployment, acceptable latency, and simple onboarding. One bad install can turn a paid pilot into a support ticket, and that hurts renewal talks fast because instructors remember friction more than the demo.
Test The Full Stack First
Lock the hardware list, then test the full stack in the same room type the customer will use. Check headset setup, device management, network connection, update process, and remote support steps before go-live. If any part needs manual work, document the fix before the first session so day-one users do not depend on one person.
- Verify headset compatibility first.
- Run classroom checks on target networks.
- Document remote support and updates.
- Train facilitators before the pilot.
If Year 1 support is effectively one Customer Success Manager at $85,000 annual salary, the setup has to be simple enough that one person can handle rollout questions without rescuing every classroom.
3
Compliance, Privacy, And Liability Readiness
Compliance gate before launch
Hospitals and residency programs will not clear a training-only VR product if the claims, data use, or contracts are loose. For a medical training business, the launch gate is legal review of positioning, disclaimers, insurance, and institutional terms. If protected health information is used, a HIPAA review is needed; FDA review is use-case dependent, so don’t assume it applies. Weak paperwork can delay procurement and push pilot approvals past launch.
Here’s the quick math: disclosed compliance overhead is $5,000/month for legal and patent maintenance plus $4,000/month for insurance and liability, or $9,000/month before any sales support. What this hides is timing risk: if contracts, data handling, and customer-site rules are not settled, the first pilot may be ready clinically but still blocked administratively.
Lock the legal setup first
Get counsel to confirm the product stays in training-only scope, with clear disclaimers, data handling rules, and customer-specific terms. The founder should map which settings use only de-identified data, which trigger HIPAA review, and which institutional requirements apply before a site visit. That keeps the launch plan honest and avoids last-minute redlines that slow first revenue.
- Confirm contract language before demos.
- Collect insurance certificates early.
- Document data flow and retention.
- Assign one owner for vendor forms.
Build the launch file with contracts, privacy language, and a simple approval checklist. If any hospital or university needs extra forms, chase them before the pilot date. One clean packet speeds pilot approvals; one missing document can hold up day-one access even when the software is ready.
4
Institutional Pilot Pipeline
Institutional Pilot Pipeline
Hospitals do not buy VR surgical training on interest alone. This launch driver matters because the business opens on time only if it has a real pilot path: named clinical champions, an economic buyer, a simulation center director, a defined scope, and success metrics. Without those pieces, demos stall and first revenue slips.
The bottleneck is budget authority. A residency program may like the product, but if procurement starts late or the pilot lacks approval steps, day-one selling turns into waiting. That slows paid pilots, delays department contracts, and can push opening past the point where the team is ready to support active users.
Pilot Setup Before Opening
Build the funnel around residency programs, medical schools, surgical departments, device partners, and continuing medical education groups. The source funnel assumes 50% visitor-to-lead and 100% lead-to-paid conversion in Year 1, with $1,500 CAC starting out. Here’s the quick math: if leads are not tied to a funded pilot, the pipeline looks active but cash does not land.
Before launch, lock the pilot packet: scope, users, timeline, success metrics, and procurement steps. One clean one-liner: no budget owner, no pilot. If the hospital asks for proof points, be ready to show how the pilot is measured and who signs off, so the team can move from interest to paid use without reopening the plan.
- Confirm champion and budget owner.
- Define pilot scope and dates.
- Write success metrics before demos.
- Map procurement steps early.
- Track each lead to paid pilot.
5
Onboarding And Customer Support Operations
Post-Sale Pilot Support
VR surgical training can be sold and still miss launch if instructors cannot use it on day one. The real readiness gate is installation support, facilitator guides, user training, and troubleshooting so pilots complete, usage stays high, and the buyer sees training value instead of setup pain.
This is also where the handoff to contract revenue happens. Usage reporting, renewal check-ins, and pilot-to-contract handoff tasks need clear ownership, or weak adoption from confused instructors can stall conversion even when the product is already paid for.
Build the Support Cadence Before Go-Live
Set the support flow before the first pilot starts: instructor training, hardware logistics, help desk routing, and reporting templates. For Year 1, the staffing plan calls for 1 Customer Success Manager at $85,000 annual salary, or about $7.1k per month, so the launch budget has to cover more than sales and software.
- Train instructors before first use.
- Test hardware setup in customer sites.
- Document help desk response steps.
- Send usage reports on a fixed cadence.
- Schedule renewal check-ins early.
What this hides: if onboarding drags, the pilot can still fail after sale, which hurts testimonials and slows the shift from pilot to contract. The support workflow should be ready before opening so the team can handle day-one questions without scrambling.
6
Related Products
- Virtual Surgery Simulation Training Porter's Five Forces Analysis
- Virtual Surgery Simulation Training BCG Matrix
- Virtual Surgery Simulation Training Business Model Canvas
- What Are The 5 KPIs For Virtual Surgery Simulation Training Business?
- Virtual Surgery Simulation Business Plan Template in Pre-Written Word
- How Increase Virtual Surgery Simulation Training Profitability?
- What Are Operating Costs For Virtual Surgery Simulation Training?
- Virtual Surgery Simulation Startup Costs: $797K Launch Funding
- Virtual Surgery Simulation Financial Model Template in Excel
- How Much Can a Virtual Surgery Simulation Owner Make at $43M
- How To Write A Business Plan For Virtual Surgery Simulation Training?
- Virtual Surgery Simulation Training Marketing Mix
- Virtual Surgery Simulation Training Marketing Plan
- Virtual Surgery Simulation Training Business Proposal
- Virtual Surgery Simulation Training PESTEL Analysis
- Virtual Surgery Simulation Training Pitch Deck Example Editable PPTX
- Virtual Surgery Simulation Training Business SWOT Analysis
- Virtual Surgery Simulation Training Value Proposition Canvas
Frequently Asked Questions
Start with one validated training use case, not a full library Build or license the first module, secure surgeon advisor review, test VR delivery, and structure paid pilots The model assumes a 6 to 12 month launch path, Year 1 academic pricing of $2,500 per month, and a $15,000 academic setup fee