 Owner income$2.1M-$17.9M
Owner income$2.1M-$17.9MHow Much Can a Virtual Surgery Simulation Owner Make at $43M

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$2.1M-$17.9M  Net margin49%-79%
Net margin49%-79% Revenue for target pay$445k
Revenue for target pay$445k Business difficultyHard
Business difficultyHard


A virtual surgery simulation training owner could plan for a modeled $220,000 annual CEO and Medical Director salary, with any extra take-home depending on retained cash, taxes, debt, and reinvestment needs In the researched base model, the business reaches $4331 million in Year 1 revenue and $1919 million in EBITDA, after payroll that includes that owner role By Year 5, revenue reaches $22545 million and EBITDA reaches $17688 million Those are planning assumptions, not guaranteed income
Owner income$2.1M-$17.9MNet margin49%-79%Revenue for target pay$445kBusiness difficultyHardWant to test your owner pay?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate, not guaranteed salary, tax advice, or owner distribution advice. Actual owner income depends on revenue, margin, payroll, taxes, debt, reserves, and reinvestment needs.
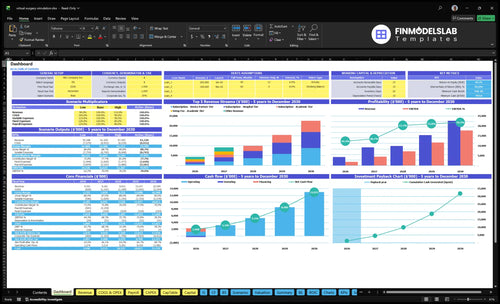
How do I check owner income in the model?
This screenshot shows revenue, EBITDA, cash, break-even, payback, and minimum cash; open the Virtual Surgery Simulation Training Financial Model Template. It’s a planning tool, not a salary promise.
Owner-income model highlights
- Revenue drives take-home
- EBITDA shows margin
- Scenarios test coverage
How much can a virtual surgery simulation training owner take home?
For a Virtual Surgery Simulation Training owner serving as CEO and Medical Director, modeled take-home pay is $220k in Year 1, with $1.919M EBITDA left after that salary on $4.331M revenue. For startup cost context, see How Much To Launch Virtual Surgery Simulation Training Business?, but don’t treat revenue as income; distributions still depend on reserves, taxes, debt service, capex, and reinvestment.
Owner Take-Home
- Modeled salary: $220k/year
- Year 1 revenue: $4.331M
- EBITDA after salary: $1.919M
- Month 2 cash need: $797k
Cash Stays In
- Fund engineering work
- Pay 3D art production
- Cover surgeon advisor review
- Support sales, success, and demos
Is a VR surgical simulation training business scalable?
Virtual Surgery Simulation Training can scale if it moves from founder-led custom work to repeatable subscriptions and renewals. With plans priced at $2,500 to $12,000 per month in Year 1 and $3,000 to $15,000 per month by Year 5, annual revenue can grow from about $4.331M to $22.545M while fixed overhead stays near $324k per year. The real choke points are long procurement, pilots, budget cycles, faculty adoption, and complex buying groups.
Scale drivers
- Reuse modules across institutions.
- Turn custom work into subscriptions.
- Grow renewals, not one-offs.
- Keep overhead near $324k.
Key risks
- Procurement can drag for months.
- Pilots can stall without clear proof.
- Faculty adoption can slow sales.
- Decision-maker sets are often complex.
What margins can a VR surgical simulation training business earn?
Virtual Surgery Simulation Training can earn strong margins: delivery gross margin is 86% in Year 1 and 90% in Year 5, while contribution margin is 77% to 83% after commissions and medical expert review fees. For startup cost context, see How Much To Launch Virtual Surgery Simulation Training Business? because the margin profile depends on how much hardware and custom setup you bundle in.
Margin drivers
- 86% delivery gross margin in Year 1
- 90% delivery gross margin in Year 5
- 77% contribution margin in Year 1
- 83% contribution margin in Year 5
What moves margin
- Reusable software licensing protects margin
- Custom builds and bundled hardware lower it
- Quality assurance and expert input add cost
- EBITDA margin rises from 443% to 785%
Want the six main income drivers?
1
$2.5K-$12KContract Value
Higher monthly tier prices set the revenue ceiling, and the hospital and partner deals lift owner income fastest.
2
$4.3M-$22.5MCustomer Count
More active customers scale recurring revenue from Year 1 to Year 5, so sales volume is the next big driver.
3
86%Gross Margin
A strong margin leaves more cash after cloud and hardware costs, and that cash is what pays the team and the owner.
4
$815KPayroll Load
Year 1 payroll is already heavy, so hiring pace and role mix decide how much profit reaches take-home.
5
5xRenewals
Sticky contracts smooth cash and help revenue compound from Year 1 to Year 5 instead of resetting each cycle.
6
14%-10%Module Reuse
Reusing simulations keeps direct costs down, which protects margin as the content library grows.
Virtual Surgery Simulation Training Core Six Income Drivers
Institutional Contract Value
Institutional Contract Value
This driver is the annual contract value before costs. Here’s the quick math: 0.6 × $2,500 + 0.3 × $5,000 + 0.1 × $12,000 = $4,200 per month, or $50,400 a year in subscription revenue before setup fees.
One-time fees add real cash: $15k academic, $25k hospital, and $50k device partner. At the stated mix, Year 1 contract value is about $71,900 per account. A higher hospital or device partner mix raises revenue fast, while mostly academic deals keep contract value lower and slow owner take-home pay.
Price the mix, not just the seat
Track each deal by per-seat, per-site, enterprise, module-based, and custom implementation pricing. The monthly jump is large: $2,500 academic, $5,000 hospital, and $12,000 device partner. That gap changes cash flow more than small volume changes do.
- Measure mix by customer type.
- Separate subscription and setup fee.
- Test hospital and device pricing first.
If the pipeline skews academic, revenue stays thinner. If hospital and device partner share rises, contract value and gross profit improve without needing the same number of new logos. That makes it easier to cover fixed payroll and still pay the owner.
1
Number of Active Customers
Active Customers
Active customers are the signed institutions that are live and paying, not just in talks. In Year 1, $150k of marketing at a $1,500 CAC implies about 100 acquired customers, but owner income only rises after onboarding and sales costs clear. If those institutions move into paid use faster, subscription cash flow improves and the owner can draw more profit.
Here’s the catch: procurement, pilots, budget cycles, and committee reviews can delay revenue even after a deal is signed. By Year 5, $700k of marketing at a $1,200 CAC implies about 583 acquired customers. That scale helps, but only if a larger share becomes active fast enough to cover payroll, support, and fixed overhead without long cash gaps.
Track live conversion speed
Measure the path from visitor to lead to paid institution. The funnel improves from 5% visitor-to-lead and 10% lead-to-paid in Year 1 to 7% and 15% in Year 5, so the same traffic produces more active customers later. One clean rule: track days from first meeting to go-live, because slow onboarding ties up cash and delays owner pay.
Watch these three numbers each month: CAC, time to activation, and active accounts by institution type. If pilots keep slipping past budget approval, signed deals still won’t fund the business on time. Push for shorter procurement steps, standard onboarding, and clear launch dates so more contracted customers turn into revenue instead of sitting in the pipeline.
2
Reusable Module Library
Module Reuse
The income lift comes from selling the same surgical module to more schools, hospitals, and training centers instead of rebuilding it each time. Custom work uses engineer time, 3D artist time, medical expert review, and QA, so reuse raises gross margin and shortens payback on development. The key inputs are module count, reuse share, and custom-build hours; what this hides is that every one-off tweak still burns expert and QA capacity.
Track Reuse Rate
Measure how many contracts use an existing module versus a new build, then watch the labor hours tied to review and QA. That is what protects owner pay. With 1 lead VR engineer and 2 3D artists in Year 1, and 2 engineers plus 5 3D artists by Year 5, wider curriculum breadth only helps if it supports renewals and larger contracts.
- Track reused-module share by contract.
- Log custom build hours by role.
- Price one-off edits separately.
- Review gross margin each month.
3
Gross Margin And Delivery Costs
Gross Margin And Delivery Costs
What matters here is the gap between revenue and delivery COGS before fixed overhead hits. In Year 1, 6% cloud hosting and data storage plus 8% hardware provisioning and logistics leaves an 86% gross margin. By Year 5, 4% cloud and 6% hardware lifts gross margin to 90%. That means every $1.0M of revenue keeps about $860k to $900k before overhead.
Don’t stop at delivery COGS. If you also carry 5% commissions and 4% to 2% medical expert review, contribution drops to roughly 77% to 79% in Year 1 and 81% to 83% in Year 5, before fixed costs. Hardware bundling, deployment labor, and support tickets can push that lower, so owner pay depends on keeping service work from eating the spread.
Track Variable Cost Per Contract
Measure margin by contract type, not just by total company average. Track cloud cost, hardware shipped, commission rate, expert review time, and support hours on each deal. Here’s the quick math: gross profit = revenue minus delivery COGS, then subtract other variable costs to see what is left for fixed overhead and owner draw.
Use one simple rule: if a deal needs heavy setup, price it up or separate it. Pass through hardware, cap deployment labor, and bill for custom review when usage rises. Watch these inputs monthly:
- Cloud and storage per active user
- Hardware kits per contract
- Support tickets per site
- Commission as a percent of sales
- Expert review hours per module
4
Renewal And Utilization
Renewal And Utilization
Renewal is not guaranteed recurring revenue here. If residents, faculty, and training cohorts keep using the platform inside the curriculum, the subscription looks like a budgeted teaching tool; if they don’t, it behaves like a one-year pilot and revenue resets to selling again.
Track active users, session frequency, module completion, and renewal rate together. The calculator should let the owner edit renewal rate, because no renewal percentage is provided in the source data. Higher usage supports cash flow and owner pay by reducing replacement-sales pressure on a $4,200 monthly weighted Year 1 subscription base.
Raise Renewal Through Usage
Build renewal around curriculum integration, not demo use. Ask each account how many residents, faculty, and cohorts use the modules each month, then compare that against the seats sold. Low adoption is a warning sign: renewal risk rises fast when the product never becomes part of required training.
Use a simple rule in forecasting: more usage means more stable revenue, less churn, and less pressure on new sales to cover payroll and overhead. Track which modules are used most, where onboarding stalls, and which accounts need faculty buy-in. One clean metric: active training sessions per account per month.
- Track renewal rate by account.
- Measure sessions by cohort.
- Flag low-use accounts early.
- Tie usage to curriculum slots.
5
Owner Role And Payroll Structure
Payroll Load and Owner Pay
Payroll protects delivery quality, but it also cuts the cash the owner can take home. Year 1 payroll is $815k, including $220k for the CEO and Medical Director, $180k for the lead VR engineer, $190k for two 3D artists, $140k for sales, and $85k for customer success. Add $324k a year of fixed overhead, and owner pay depends on gross profit after staff costs.
Split owner salary from employee payroll and profit draws. That keeps the model clean when you forecast cash. Founder-led sales can save cash early, but it can also slow scale if the founder is the main seller and manager at the same time. By Year 5, payroll is shown at $1.815M, so the business needs stronger contract volume before distributions can grow.
Track Payroll Against Recurring Revenue
Measure payroll against signed institutional revenue, not just headcount. Track how much of payroll is tied to delivery, sales, and customer success, because custom module work pulls engineer and artist time. The key inputs are active contracts, onboarding load, support tickets, and module backlog. If payroll rises faster than subscription revenue, owner take-home income gets squeezed fast.
- Separate owner pay from staff payroll.
- Track contract revenue per payroll dollar.
- Watch sales cycle time and close rate.
Test whether founder-led sales is really cheaper. If the founder owns too much selling, delivery and product work can slip, which hurts renewals and expansion. A lower salary may help cash in the short run, but the bigger risk is slower growth and thinner profit for distributions.
6
Compare owner-income scenarios using the researched model periods
Owner income scenarios
Owner income moves with ramp, scale, and the size of the hospital mix. Year 1 is still building; Year 3 and Year 5 show much larger EBITDA, but distributions still depend on reserves, taxes, debt, and reinvestment.
| Scenario | Low CaseEarly ramp | Base CaseScale year | High CaseMature upside |
|---|---|---|---|
| Launch model | Year 1 is the ramp case: $4.331M revenue, $1.919M EBITDA, and a $220k owner salary before any draw. | Year 3 is the scale case: $9.912M revenue and $7.205M EBITDA create a stronger owner-income path. | Year 5 is the mature case: $22.545M revenue and $17.688M EBITDA support the strongest owner-income path. |
| Typical setup | Academic sales lead at 60%, marketing is $150k, payroll is $815k, and the team is still building conversion. | Hospital sales reach 40%, marketing rises to $400k, and operating leverage improves as the funnel matures. | Hospital sales reach 50%, payroll climbs to $1.815M, and marketing reaches $700k while margins stay high. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | Salary-led, limited drawEarly ramp | Scaled salary plus drawScale year | High distribution capacityUpside case |
| Best fit | Use this to stress-test the first operating year. | Use this as the midpoint planning case. | Use this to test upside if growth stays strong and reinvestment stays controlled. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or actual distributions.
Related Products
- Virtual Surgery Simulation Training Porter's Five Forces Analysis
- Virtual Surgery Simulation Training BCG Matrix
- Virtual Surgery Simulation Training Business Model Canvas
- What Are The 5 KPIs For Virtual Surgery Simulation Training Business?
- Virtual Surgery Simulation Business Plan Template in Pre-Written Word
- How Increase Virtual Surgery Simulation Training Profitability?
- What Are Operating Costs For Virtual Surgery Simulation Training?
- Virtual Surgery Simulation Startup Costs: $797K Launch Funding
- Virtual Surgery Simulation Financial Model Template in Excel
- How To Start A Virtual Surgery Simulation Training Business In 6-12 Months
- How To Write A Business Plan For Virtual Surgery Simulation Training?
- Virtual Surgery Simulation Training Marketing Mix
- Virtual Surgery Simulation Training Marketing Plan
- Virtual Surgery Simulation Training Business Proposal
- Virtual Surgery Simulation Training PESTEL Analysis
- Virtual Surgery Simulation Training Pitch Deck Example Editable PPTX
- Virtual Surgery Simulation Training Business SWOT Analysis
- Virtual Surgery Simulation Training Value Proposition Canvas
Frequently Asked Questions
The researched model includes a $220,000 annual CEO and Medical Director salary The company also shows $1919 million in Year 1 EBITDA on $4331 million of revenue, but EBITDA is not owner cash Distributions depend on reserves, taxes, debt, capex, and how much cash stays inside the company