How Much Altitude Sickness Prevention Owners Make at 567 Visits/Month
You’re estimating whether a US altitude sickness prevention service can pay an owner, not a guaranteed salary Using the researched first-year plan, 567 monthly consultations produce about $713k in monthly revenue, with costs, reserves, and owner pay modeled separately This excludes taxes, legal advice, clinical protocols, and guaranteed earnings
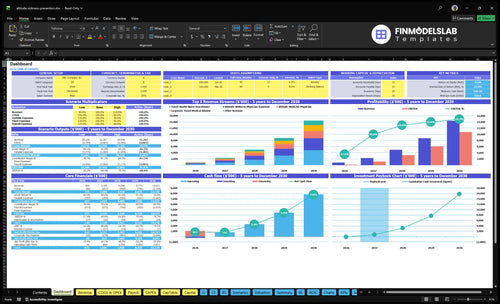
Owner income$137kNet margin18%Revenue for target pay$713kBusiness difficultyHard
Want the six owner income drivers?
1
Traveler Volume
14x
More travelers drive most of the revenue jump, so fixed staff and software get spread over more visits.
2
Visit Price
$126-$150
Higher revenue per traveler lifts top-line dollars fast without the same lift in labor.
3
Fixed Overhead
$419K/mo
The monthly overhead floor is high, so owner income only grows once volume covers rent, software, legal, IT, and admin payroll.
4
Clinical Staffing
$210K
The Medical Director salary alone is a big fixed cost, and rising clinician FTEs can quickly change EBITDA.
5
Acquisition Load
12%
Year 1 marketing and referral costs take 12% of revenue, so cheaper demand creation lifts take-home cash.
6
Fulfillment Costs
No COGS
Medication and fulfillment economics can move margin, but the model does not give drug cost data yet.
Want to test your owner pay target?
Owner income calculator
Estimate owner take-home and the target-pay gap from monthly revenue, gross margin, labor, overhead, marketing, debt service, reserves, and target pay. The base case is anchored to the first-year operating plan.
!
Planning note: This is a researched planning estimate, not guaranteed salary, tax advice, or owner distribution advice. Actual take-home depends on revenue, margin, payroll, overhead, debt, and reserves.
Can an altitude sickness prevention service support a full-time owner?
Yes, an Altitude Sickness Prevention Service can support a full-time owner in the first-year planning case if demand reaches about 512 consultations/month; track demand, margin, and capacity with What Are The 5 KPIs For Altitude Sickness Prevention Service Business?. Target owner pay is not guaranteed, but the planning math uses $126 average revenue, 78% contribution margin, and about $419k fixed overhead.
Owner Pay Math
$126 average revenue per consultation
78% contribution margin after variable costs
$419k annual fixed overhead
$100k target before taxes and reserves
Volume Check
512/month supports the base planning case
$150k known payroll raises the hurdle
555/month is the safer target
567/month researched first-year volume clears it
How does an altitude sickness prevention service scale?
Altitude Sickness Prevention Service scales when it serves more qualified travelers, pushes higher provider capacity, and adds partner-led bookings. The model rises from 567 consultations/month in year 1 to 8,024/month in the mature year, and modeled revenue climbs from $713k/month to $120M/month. Owner-led work can protect early margin, but once staffing grows, compliance, payroll, support, and reinvestment needs rise fast, so scale does not automatically mean bigger distributions.
What drives growth
More qualified travelers
Higher capacity use
Partner-led bookings
Consults rise to 8,024/month
What growth changes
Owner-led care protects early margin
Staffing adds compliance burden
Payroll and support costs rise
Reinvestment can limit distributions
What affects profit margin for an altitude sickness prevention service?
For an Altitude Sickness Prevention Service, margin is mostly driven by service cost mix, marketing, and whether booked visits actually show up. If you want the planning side, How To Write A Business Plan For Altitude Sickness Prevention Service? fits these numbers: first-year direct service costs are 10% of revenue, split 45% telehealth platform fees and 55% malpractice, and marketing plus referrals add another 12%. With $119k/month fixed overhead and $300k/month known payroll in year one, no-show rates, clinician staffing, prescription workflow, pharmacy coordination, and paid search efficiency can move owner take-home fast; reserves should stay separate from profit.
First-year revenue averages about $126 per traveler.
Known payroll and overhead total $419k monthly.
Marketing and referrals consume 12% of revenue.
Compare low, base, and high owner income scenarios
Owner income scenarios
Owner income rises with visit volume, pricing, and staffing capacity. The spread from Year 1 to Year 5 shows how faster growth lifts operating profit while fixed payroll still anchors the downside.
Compare early, modeled, and mature owner income capacity.
Scenario
Low CaseDownside case
Base CaseModel case
High CaseUpside case
Launch model
Lower intake keeps owner income near the early run-rate.
Modeled growth lifts owner income to the mid-cycle run-rate.
Stronger demand and higher capacity push owner income toward the mature-year run-rate.
Typical setup
Year 1 uses 2 physicians, 3 nurse practitioners, 1 specialist, 2 physician assistants, and 1 corporate advisor.
Year 3 reaches about $5.0M revenue and $3.24M EBITDA with a scaled provider mix.
Year 5 reaches about $14.4M revenue and $10.8M EBITDA with the largest provider slate.
Cost drivers
Consult volume
clinician mix
telehealth fees
malpractice cost
fixed payroll
Consult volume
price per consult
staffing scale
marketing spend
platform fees
Consult volume
higher pricing
provider utilization
marketing efficiency
fixed payroll
Owner income rangeBefore owner reserves
~$13k/monthEarly run-rate
~$270k/monthModeled run-rate
~$898k/monthPeak capacity
Best fit
Use this if you want a cautious view of opening-year owner income and slower demand.
Use this as the core planning case for a business that reaches Year 3 capacity.
Use this to test upside if demand, pricing, and utilization stay strong through the mature period.
!
Planning note: These ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Altitude Sickness Prevention Service Core Six Income Drivers
Qualified Traveler Volume
Qualified Traveler Volume
Qualified traveler volume is the number of high-altitude travelers who actually book and show up for a consultation. It is the first gate on revenue and owner pay: the first-year plan serves 567 travelers/month, above the 428 break-even level, so the business clears fixed costs only if bookings stay steady. One line: more qualified travelers means faster break-even and more cash for the owner.
Seasonality is the main risk. Demand rises with ski trips, trekking seasons, mountain tourism, and international high-altitude travel, then drops in the off-season. That matters because a profitable average month can still turn into a tight cash month when volume falls, while fixed overhead and payroll keep running. The model also shows a scale path toward 8,024 monthly consultations in the mature year.
Track Booked Consults
Track leads, booking rate, show rate, and monthly consult volume by source. Those four inputs tell you whether traveler demand is real or just traffic. If booked volume slips below 428/month, each consult has to carry more of the $119k/month fixed overhead and the $300k/month first-year payroll, so owner draw gets squeezed fast.
Forecast volume by season, not by annual average. Push referral and pre-trip outreach before peak travel windows, then staff for the actual month-by-month curve instead of a flat plan. Keep an eye on canceled visits and unused slots; both reduce contribution profit, which is the cash left after direct service costs and the money that can support owner pay.
Clinical Delivery Cost And Staffing
Clinical Staffing Cost
When licensed clinical work is expensive, owner income gets squeezed fast. This model separates clinical care from non-clinical ops, but the disclosed payroll still includes a $210k Medical Director, $95k Operations Manager, and $55k Patient Care Coordinator, with first-year known payroll at $300k/month. Longer visits, contractor rates, and physician oversight all push gross margin down.
Here’s the quick math: revenue must cover provider comp per consult, then payroll, then overhead before the owner can take home anything. Because provider compensation per consultation is not listed, treat it as a separate input and stress-test it by visit length and utilization. If clinical time rises and consult volume stays flat, cash available for owner pay drops first.
Track Labor Per Consult
Measure licensed minutes per consult, provider pay per visit, and admin labor per booking. Keep clinical and non-clinical hours in separate buckets so you can see where margin is leaking. If oversight time keeps growing, the service may look busy but still fail to fund owner draw.
Track cost per completed consult
Separate clinical vs admin payroll
Stress-test contractor rates monthly
Watch utilization against payroll
One clean test: if payroll rises faster than consult volume, gross margin falls. That is the signal to shorten visits, tighten protocols, or raise price before cash flow turns tight. What this estimate hides is the size of provider comp per consult, so build your forecast with that line item explicit.
Customer Acquisition Efficiency
Customer Acquisition Efficiency
Customer acquisition efficiency is how much it costs to book each qualified traveler. Here, first-year digital marketing runs at 9% of revenue and referral commissions at 3%, or about $86k/month on $713k revenue. In mature year, marketing drops to 7% while referrals stay at 3%, so better channel mix leaves more cash for owner pay.
Track qualified leads, booked consultations, and cost per booked traveler. One clean rule: if paid ads rise faster than consult revenue, margin gets squeezed even when bookings grow. SEO, travel agencies, trekking outfitters, ski resorts, universities, and corporate travel programs can cut paid pressure, but only if they book at a lower cost per consult.
Measure CAC by channel
Build customer acquisition cost, or CAC, by source and compare it to contribution profit, not bookings alone. Use the 9% first-year marketing target as the ceiling until partner and referral channels prove cheaper. If a channel needs heavy paid spend to close travelers, it may grow top-line volume but still reduce the owner’s take-home income.
Track cost per booked consult.
Track show rate by channel.
Track referral commission at 3%.
Track revenue per traveler.
Track contribution profit per booking.
If SEO, partner referrals, or corporate travel programs lower CAC below paid search, shift budget there. That matters most in weak off-season months, when a full calendar can still produce thin cash if acquisition spend stays high.
Average Revenue Per Traveler
Average Revenue per Traveler
This is the cleanest pricing lever in the model. The first-year weighted average revenue is about $126 per traveler, based on $100 physician assistant, $110 nurse practitioner, $150 physician, $200 corporate advisor, and $225 expedition specialist visits. At 567 travelers/month, that works out to about $71,442/month in revenue before overhead and marketing.
Bundles, follow-up support, family or group scheduling, and partner referrals can lift revenue per booking without adding the same number of new travelers. Every $10 increase in average revenue adds about $5,670/month at first-year volume, which can flow straight into owner pay after fixed costs are covered. What this hides: longer consults and more support time can eat the gain.
Raise Booking Value
Track average revenue per traveler (ARPT) by service line, not just total bookings. Split out consult fees, follow-up revenue, group scheduling, and referral income so you can see whether the mix is drifting toward $100-$110 visits or higher-value $150-$225 cases. If the mix weakens, revenue can look busy but still leave less cash for the owner.
Price for guidance, coordination, and eligible clinical review, not guaranteed medication outcomes. Use simple add-on scripts for bundles and family bookings, but cap staff time per case so higher ARPT does not get lost to longer visits, extra handoffs, or avoidable follow-up. A steady higher ARPT supports better gross margin and a larger profit draw.
Fixed Overhead, Compliance, And Reserves
Fixed Overhead and Reserve Cash
Fixed overhead is the monthly cost that stays on even when patient volume dips: $119k/month for HIPAA-compliant software, rent, liability insurance, legal, cybersecurity, accounting, and telecom. Add known payroll of $300k/month in year one, and fixed spend hits $419k/month before variable clinical costs. That is the cash hurdle the owner has to clear before taking anything home.
In the mature year, known payroll rises to $483k/month, so fixed load climbs to $602k/month. Reserves are not profit; they’re cash held back for compliance work, insurance, bookkeeping, licenses, and admin. One clean rule: if you pay the owner before those reserves, you’re spending next month’s operating cash.
Track Cash Before Owner Draw
Run owner pay from cash left after overhead, payroll, and compliance reserves. The key check is owner draw = cash after fixed overhead, payroll, and reserves, not accounting profit. If revenue looks fine but legal, cyber, or license costs spike, distributable cash can drop fast.
Fixed overhead by month
Known payroll by role
Reserve balance before draw
At $713k/month revenue, the first-year fixed load of $419k uses 58.7% before variable costs. Keep reserves separate in the forecast and in the bank, so compliance spending does not quietly cut owner income.
Medication And Fulfillment Workflow
Medication Fulfillment Economics
This driver is the step from consult to medicine in the patient’s hands. It includes prescription review, pharmacy partner fees, pickup or shipping coordination, support time, and failed fulfillment. Since the model already includes platform and malpractice costs but excludes medication COGS, shipping cost, and pharmacy margin, these items sit on top of the base margin and can cut owner take-home fast.
What this estimate hides is rework. If a prescription needs a second review, a pharmacy handoff fails, or staff spend extra time on coordination, cash outflow rises before revenue changes. That hurts monthly profit and can turn a busy month into a thin one, especially if the service bills a fixed consult fee but carries variable workflow cost per case.
Track Fill Rate and Support Load
Track fill rate, support minutes per case, partner fee per prescription, and failed fulfillment rate. Split cases by pickup versus shipping, then test which path closes faster and with less staff time. The goal is simple: keep more of each consult fee as contribution profit, not coordination work.
Document the prescription review steps so the team knows who approves, who sends, and who follows up. If a pharmacy partner adds friction, replace the guesswork with a fixed fee schedule and a clear service-level target. That protects margin, keeps refunds and resends down, and leaves more cash for owner pay.