Cost To Start An Altitude Sickness Prevention Service: $826K Plan
You’re planning a regulated travel health service, so the opening budget needs to cover clinical setup, telehealth systems, medication access workflows, insurance, launch marketing, and working capital In the researched base model, startup CAPEX is $235K, minimum cash need is $826K in Month 2, and first-year revenue is $855K These are planning assumptions, not vendor quotes or guarantees
Calculate Fuding Needs
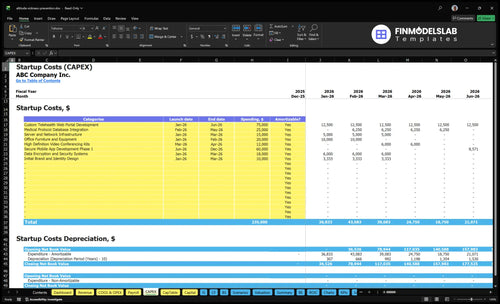
Startup cost summary
This table shows startup CAPEX and excluded operating cash needs for a telehealth service that prevents high-altitude illness.
Highlighted CAPEX$235,000Base planning example
Excluded cash needs$826,000Outside CAPEX total
Funding need$1,061,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Patient-facing telehealth web portal build
$75,000
Portal design, build, and launch setup
Yes
Medical protocol database setup
$25,000
Clinical content and protocol integration
Yes
Secure mobile app development phase 1
$60,000
Mobile workflow build and release
Yes
Data encryption and security systems
$18,000
Security controls and data protection
Yes
Clinical infrastructure, office, and brand setup
$57,000
Server, furniture, video kits, and brand design
Yes
Operating reserve
$826,000
Month 2 cash runway for payroll and fixed costs
No
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
This estimates capitalized startup assets only for an altitude sickness prevention service.
!
Funding note This block covers capitalized startup assets only. It excludes working capital, payroll runway, deposits, inventory runway, monthly ad spend, medication replenishment, recurring software subscriptions, debt service, and other operating costs. Base asset subtotal is $235k before contingency, and total funding need should be checked separately against the $826k minimum cash floor.
Costs shift fast because a telehealth-only launch can defer office spend, while an office-enabled or multi-state setup adds capex, legal work, clinician coverage, and more working capital.
Lean, Base, and Full cost bands for an altitude illness prevention service.
Scenario
Lean LaunchLowest fixed footprint
Base LaunchOffice-enabled launch
Full LaunchBroader state coverage
Launch model
Telehealth-only launch with deferred office spend and tight clinical oversight.
Office-enabled launch using the modeled staffing, capex, and operating plan.
Multi-state launch with broader clinician coverage, stronger compliance, and more working capital.
Typical setup
Use secure consult workflows, remote prescribing, malpractice coverage, and pharmacy coordination.
Open a small office, run HIPAA-compliant software, and support Year 1 staffing and marketing.
Expand coverage, add legal review and cyber controls, and carry more staff before demand catches up.
Cost drivers
Secure workflow build
clinical oversight
malpractice insurance
pharmacy coordination
Office lease and buildout
HIPAA software
Year 1 payroll
marketing and referrals
cash runway
Multi-state legal review
clinician coverage
cyber controls
insurance load
extra working capital
Planning rangeCAPEX only
$500,000 - $800,000Lower cash need
$1.0M - $1.1MModel case
$1.5M - $2.0MHigher cash need
Best fit
Solo clinical operators who want the lowest fixed footprint and can start with a small remote team.
Local travel health service founders who want the model case and can fund a staffed launch.
Funded teams planning multi-state coverage and able to absorb higher compliance and staffing costs.
!
Planning note: These scenario ranges are researched planning assumptions, not exact quotes or vendor bids.
What are the hidden costs of starting an altitude sickness prevention service?
Starting an Altitude Sickness Prevention Service has two cost buckets: pre-opening setup and working capital. The hidden pre-opening items include legal review, consent forms, clinical protocols, pharmacy workflows, patient education, cyber setup, and insurance deposits, while the monthly burn can quickly stack up with $25K software, $45K rent, $15K IT and cybersecurity, $12K legal, $1K accounting, $800 liability insurance, and $400 telecom; see How To Write A Business Plan For Altitude Sickness Prevention Service?. Add merchant fees, license renewals, customer acquisition testing, and delays in clinician or pharmacy onboarding, and the cash need can reach $826K minimum.
Pre-opening costs
Legal review of state rules
Consent forms and protocols
Pharmacy workflow setup
Patient education and cyber setup
Runway costs
$25K monthly software
$45K rent and $15K IT
$12K legal plus $1K accounting
$826K cash need if delays hit
How to fund an altitude sickness prevention service startup?
For the Altitude Sickness Prevention Service, fund the build in tranches: $235K in CAPEX across Months 1-12, but raise to cover a $826K Month 2 cash need once you add $445K of Year 1 payroll, $119K monthly fixed overhead, and launch marketing at 9% of revenue plus 3% referral commissions. Base-case revenue is $855K in Year 1 and $2.306M in Year 2, so the plan should assume a Month 2 breakeven run, not a smooth burn.
Funding plan
$235K CAPEX over 12 months
$826K minimum cash in Month 2
$445K Year 1 payroll load
9% marketing plus 3% referrals
Downside cases
30% to 50% lower role capacity
Slower consult volume than plan
Higher malpractice premiums
Delayed pharmacy coordination
How much money do I need to start an altitude sickness prevention service?
You need about $1.061M to start a base hybrid Altitude Sickness Prevention Service: $235K CAPEX plus $826K minimum Month 2 cash. Tie the raise to Month 2 breakeven, 15-month payback, and $855K Year 1 revenue; track the operating levers in What Are The 5 KPIs For Altitude Sickness Prevention Service Business?.
Base funding
$235K asset spend
$826K Month 2 cash need
$1.061M total funding logic
$855K Year 1 revenue target
Model choices
Telehealth trims office costs
Keep clinical oversight funded
Budget secure technology and insurance
Staff 4 first-year roles
Key Takeaways
Clinical setup needs legal review and medical governance.
Tech setup is $205K upfront, plus monthly SaaS.
Malpractice starts at $550 per consultation in Year 1.
Launch channels run 12% of Year 1 revenue.
Altitude Sickness Prevention Service Core Five Startup Costs
Clinical Setup Startup Expense
Clinical oversight
Clinical setup pays for the medical director, state-by-state practice rules, protocols, consent forms, compliance files, and governance. Use $210K for 1 medical director in Year 1, then add altitude medicine physicians, nurse practitioners, expedition medical specialists, physician assistants, and corporate travel medical advisors as capacity needs. Legal review is ongoing; budget $12K per month as operating support, not CAPEX.
Cost inputs
This cost depends on states served, clinician employment versus contractor model, scope of medication guidance, and whether corporate travel clients need separate protocols. Build the estimate from headcount, market licenses, policy drafting, and review time. Here’s the quick math: one director at $210K plus legal at $12K monthly shapes the core fixed load.
List every service state.
Define prescribing limits early.
Separate travel-client protocols.
Control the spend
Keep the first version tight: one governance owner, one clear protocol set, and only the states you can support well. The main mistake is expanding geography before compliance is documented. If contractor coverage is allowed, it can reduce fixed payroll pressure, but assumptions need professional validation. What this estimate hides: license timing, review cycles, and added protocol work.
Start with fewer states.
Standardize consent forms.
Review scope before launch.
Governance checklist
Budget this line as the control layer, not just a hiring cost. It covers medical oversight, legal review, compliance documentation, and protocol ownership for altitude care. Use the $210K medical director baseline to anchor staffing capacity, then align every form and workflow to state requirements. Do not treat these assumptions as legal advice.
Insurance Startup Expense
Coverage Mix
Professional liability, general liability, cyber liability, and workers’ compensation if you hire all sit in this line. General liability is $800 per month, while malpractice runs $550 per consultation in Year 1 and $450 by Year 5. Premiums shift by state, clinician structure, telehealth model, coverage limits, and whether medication dispensing is involved.
Cost Build
Budget for policy deposits, first-month premiums, and the per-visit risk load. Here’s the quick math: at 567 consultations per month, Year 1 malpractice load is about $311,850 monthly, plus $800 for general liability. That makes utilization and claim control matter as much as sales volume.
Cyber Support
Cyber risk is not just the premium. The control stack includes $18K for data encryption and security systems plus $15K a month for IT and cybersecurity. That spend supports underwriting, but it does not replace cyber liability. Keep consent, records, and prescribing workflows tight so claims stay contained.
Price Drivers
Start with carrier quotes for your states, then test staffing, scope, and coverage limits. If you add clinicians, ask about workers’ compensation and any higher deposit tied to headcount. If you add medication guidance or dispensing, expect tighter underwriting and higher premiums. The cheapest policy is the one that still matches how you actually practice.
Launch Readiness Startup Expense
Launch build
$10K for brand and identity design plus $75K for the custom telehealth portal sit in CAPEX. That covers the pre-opening website, educational content, SEO, paid test ads, referral materials, and brand launch assets, but not monthly marketing or payroll. Clean separation matters so the opening budget doesn’t blur into operating spend.
Acquisition spend
Year 1 acquisition runs at 9% for digital marketing and search engine marketing plus 3% for referral commissions. On $855K of revenue, that is $102.6K in variable launch-channel spend. Here’s the quick math: $855K × 12% = $102.6K. This is ongoing operating spend, not startup CAPEX.
Onboarding setup
Budget for onboarding 1 patient care coordinator, staff training, and support process design before launch. That work should cover intake scripts, escalation rules, customer support paths, and clinical handoff steps. One clean line: if the team cannot answer a new patient fast, paid traffic just buys service friction.
Go-live split
Keep the opening budget in two buckets: one-time build for brand, website, and content, and ongoing spend for ads, referral fees, and payroll. That keeps the launch plan readable and helps you compare pre-opening cash needs against the first months of patient demand without mixing setup with run-rate costs.
Medication Access Startup Expense
Prescribing flow
For Acute Mountain Sickness (AMS) prevention, the cost starts with clinician review, consent, state rules, and e-prescribing. Use acetazolamide only as a planning example for a prescription workflow, not as unlicensed dispensing. The real expense is the time and controls needed to make each consult safe, documented, and legally clean.
Setup inputs
This cost covers pharmacy partner onboarding, patient education, medication counseling, refill rules, and adverse-event escalation. Separate pharmacy coordination from inventory; stock only matters if the service is properly licensed to dispense or handle medication. Estimate it from states served, e-prescribing integration, and the number of protocols and handouts you need.
Cost control
Keep this lean by using one standard prescribing path, one counseling script set, and one pharmacy coordination process. Don’t build inventory before licensing is clear. That keeps setup focused on workflow, not product holding. The main mistakes are state creep, extra handouts, and too many partner pharmacies with different rules.
Volume and risk
At 567 consultations per month, medication access work scales fast. Here’s the quick math: that is about 6,804 visits a year, and the stated malpractice load is $550 per consultation. What this estimate hides is the real cost of clean refill rules, escalation steps, and tight clinical review when prescribing is repeated at volume.
Telehealth Technology Startup Expense
Telehealth stack
This stack covers booking, patient intake, secure messaging, video visits, e-prescribing, records, payments, and HIPAA privacy controls. The main split is one-time build versus recurring software, because the portal and security tools are sunk costs, while SaaS and IT support scale with monthly visit volume.
Setup cost
One-time CAPEX totals $205K: $75K custom web portal, $60K secure mobile app phase 1, $25K medical protocol database integration, $15K server and network infrastructure, $18K data encryption and security systems, and $12K video conferencing kits. That is the launch base before monthly software starts.
$205K total build
Separate hardware from SaaS
Quote security last
Monthly run rate
Recurring tech spend is $25K per month for HIPAA-compliant software plus $15K for IT support and cybersecurity, or $40K monthly before transaction fees. If you hold that for 12 months, software and support alone run $480K; this is the line item to stress-test against booked consults.
$40K monthly base
$480K yearly run rate
Scale with consult volume
Per-visit cost
The Year 1 telehealth transaction fee is $450 per consultation, so the variable tech cost rises with each booked visit. The clean model is setup cost + monthly SaaS + $450 per visit, which keeps the tech budget tied to real patient flow instead of idle capacity.