How Much Home Health Care Agency Owners Make On $879K-$825M Revenue
A home health care agency owner can plan around a $100,000 director-level salary in this model if the owner fills that role, but true owner take-home cannot be proven from the supplied research because direct clinician and caregiver wage rates are not included Revenue grows from $73,295 per month in the first year to $687,600 per month in the mature year Non-labor variable costs run from 150% of revenue in the first year to 122% in the mature year, before direct care payroll, reserves, debt service, and personal taxes High billings do not equal owner income
Owner income$100kNet margin35%–79%Revenue for target pay$216k–$224kBusiness difficultyHard
Want to test your owner pay?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
!
Planning note: This is a researched planning estimate, not guaranteed salary, tax advice, or owner distribution advice. Actual owner income will move with revenue, margins, payroll, reserves, and billing timing.
Want the full forecast view for a Home Health Care Agency?
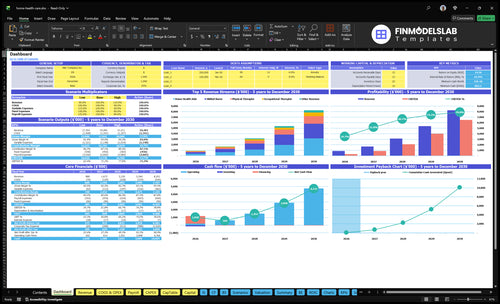
See the full forecast in the Home Health Care Agency Financial Model Template; the dashboard shows revenue, margin, cash, and owner pay, while assumptions let users change payer mix, census ramp, staffing, treatment volume, prices, capacity, overhead, and reserves. Open the model.
Owner pay and forecast highlights
$73,295 first-year monthly revenue
$687,600 mature-year monthly revenue
Low, base, high pay charts
How much revenue can a home health care agency make?
A Home Health Care Agency can reach about $879,540 in year 1 and $8,251,200 in a mature year, or roughly $73,295 to $687,600 per month. That is revenue, not owner income, so payroll, denials, and overhead can pull take-home down fast. Growth comes from skilled nurse visits, physical therapy, occupational therapy, speech therapy, and home health aide volume, plus pricing and capacity.
Revenue levels
Year 1 revenue: $879,540
Mature-year revenue: $8,251,200
Monthly range: $73,295 to $687,600
Revenue is not profit: keep it separate
Capacity drivers
Skilled nurses: 15 in mature year
Physical therapists: 9 in mature year
Occupational therapists: 6 in mature year
Speech therapists: 4; aides: 25
How many clients does a home health care agency need?
A Home Health Care Agency doesn’t need one magic client count; it needs enough active census to create 799 billable treatments/month, or about $73,295/month at $92 per billable treatment—and What Is The Most Critical Indicator To Measure The Success Of Your Home Health Care Agency? should be tracked alongside census. Count a client only when care is staffed, billable, authorized, and collectible; otherwise, it’s demand, not revenue.
Use treatments first
Model starts with billable treatments
First year: 799/month
Monthly revenue: $73,295
Average treatment revenue: $92
Know break-even
Fixed overhead plus director: $190,000/year
Revenue floor before care labor: $223,529/year
Non-labor contribution margin: 85.0%
Direct care payroll raises break-even
What profit margin can a home health care agency make?
You can’t calculate a true profit margin for a Home Health Care Agency from this data alone. Non-labor costs already run at 150% of revenue in year 1 and 122% in a mature year, so the model is negative before direct care labor; see How Much Does It Cost To Open And Launch A Home Health Care Agency? for the startup-cost side. The missing driver is direct care labor, so net profit and owner distributions can’t be calculated yet.
Cost load
150% of revenue in year 1
122% of revenue in a mature year
80% to 66% for supplies and transport
70% to 56% for EHR and insurance
Missing margin
$7,500 monthly fixed overhead
$100,000 annual Director salary
Direct care labor is not provided
Net profit cannot be solved yet
Home Health Care Agency Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
What drives owner income most?
1
Referral Flow
$880K-$8.25M
More active clients and referrals drive more billable visits, so owner take-home rises fast as census fills.
2
Payer Mix
High
Better reimbursement keeps more of each visit after write-offs, so the same staff base earns more profit.
3
Visit Volume
450%-850%
Higher billable hours and visits scale revenue with limited extra overhead once teams are in place.
4
Labor Efficiency
60%-85%
Keeping nurses and aides close to planned capacity cuts paid idle time and protects margin.
5
Compliance Overhead
$7.5K/mo
Admin, office, and compliance costs hit profit every month, so overruns go straight to owner income.
6
Cash Collections
$862K
Slow billing or weak collections can trap cash, even when EBITDA looks strong on paper.
Home Health Care Agency Core Six Income Drivers
Active Census And Referrals
Active Census and Referrals
Active census is the number of qualified patients or clients actually on staffed, billable care. In this model, monthly revenue rises from $73,295 with 12 total care workers in year one to $687,600 with 59 workers in the mature year, so referrals only help income when authorizations, staffing, documentation, and collections all hold. More leads without started care do not pay the payroll.
Track Started Care, Not Lead Count
Measure each source by profitably started care, not inquiry volume, for hospitals, physicians, discharge planners, community partners, and private-pay channels. If a source fills the pipeline but stalls on authorization or staffing, it adds work without revenue. With $7,500 in monthly fixed overhead and $100,000 in annual director pay, weak conversion cuts cash fast and lowers owner draw.
1
Payer Mix And Reimbursement
Payer Mix
Payer mix is the share of visits paid by Medicare, Medicaid, private insurance, VA programs, and private pay. It changes revenue per visit, authorization limits, denial risk, and cash timing. In year one, reimbursement ranges from $60 for home health aide treatments to $150 for skilled nurse treatments, so the same visit volume can produce very different income.
By mature year, prices range from $68 to $170. That spread can move gross profit fast, but only if the agency can actually get paid on time. Here’s the quick math: a $90 gap between low and high visits means payer mix, not just visit count, can decide whether owner pay is tight or healthy.
Track reimbursement by payer and service line
Build the model so reimbursement can change by service line and payer. Track approved visits, denial rate, days to collect, and cash received per visit. If one payer pays less or slows cash, it can squeeze payroll and delay owner draws even when census looks full.
Measure the mix by what is actually started and paid, not just by referrals. Use a simple view: visits × reimbursement × collection rate. Then test how a shift toward higher-paying, lower-denial payers changes take-home income after staffing and overhead. What this hides: authorizations can cap volume even when demand is strong.
Split revenue by payer.
Split revenue by service line.
Track denial and delay rates.
Watch cash before owner draws.
2
Billable Care Volume And Productivity
Billable Visit Conversion
This driver is the share of scheduled care that turns into billable visits or hours. Owner income rises when more of the day is billable, because revenue grows faster than fixed overhead. Billable activity is not the same as total staff hours, so a full calendar can still miss revenue if cancellations, travel gaps, or documentation time eat the day.
First-year capacity runs from 450% for speech therapy to 650% for home health aides. Mature-year capacity reaches 650% to 850%. That spread matters because every unused slot lowers gross margin and cash available for owner draw.
Track Billable Yield Daily
Measure billable hours ÷ scheduled hours by service line, clinician, visit type, and payer. That shows where the schedule leaks. If one payer, visit type, or clinician group runs low, the fix is usually in routing, authorizations, travel load, or visit mix—not just hiring more staff.
Track these inputs: scheduled hours, billable hours, cancellations, travel time, documentation time, and underfilled slots. Empty time does not pay. Tightening same-week rebooking and trimming travel gaps can lift revenue without adding headcount, which protects profit and owner income.
3
Direct Care Labor Costs
Direct Care Labor Costs
Direct care labor is the biggest swing factor in home health profit. This includes wages, payroll taxes, overtime, mileage, recruiting, training, retention, and contractor premiums. The model has clinician counts, but not wage rates, so owner income can look strong on paper while labor quietly eats the margin.
Do not chase margin by understaffing care. Test take-home only after safe coverage, supervision, and quality standards are funded. With staffing scaling from 12 workers in year 1 to 59 in the mature year, even small wage or overtime changes can swing monthly profit and cash available for owner pay.
Measure Labor Before You Draw Profit
Track labor as a share of revenue by service line, role, and payer. Here’s the quick check: if a visit brings in cash, but you still pay overtime, mileage, and contractor premiums, the true margin is lower than the billed rate suggests. Owner pay should come after all direct care hours are covered.
Track wages by clinician type.
Separate overtime from base pay.
Log mileage and contractor premiums.
Watch recruiting and training spend.
Compare staffed hours to billable hours.
What this estimate hides is simple: a fully staffed plan can still lose money if the team is paid above the visit economics. If labor runs hot, cash flow tightens fast, and the owner may need to delay draws until payroll, supervision, and care quality are fully funded.
4
Compliance And Administrative Overhead
Compliance Overhead
When volume is thin, compliance overhead eats owner pay first. Baseline fixed overhead is $7,500 per month, and the Agency Director salary adds $100,000 a year or about $8,333 a month. That means the agency needs about $15,833 a month before any owner distribution just to stay current.
Then the revenue-linked costs hit. Electronic health record fees run 30% to 40% of revenue, and liability insurance runs 26% to 30%. So compliance and admin load can take 56% to 70% of sales before direct care labor. If collections slip, take-home pay shrinks fast.
Cover overhead before draws
Build the model from collected monthly revenue, director pay, the $7,500 fixed base, EHR fee rate, and liability premium. Compliance is not optional, so owner draws should start only after these costs are covered and cash reserves are set.
Track revenue by payer and service line.
Track EHR and insurance as % revenue.
Track cash after payroll and overhead.
Hold draws until coverage is proven.
5
Collections, Reserves, And Cash Timing
Collections, Reserves, And Cash Timing
Profit is not the same as cash you can pay yourself. In home health, payroll and overhead can come due before insurers, Medicare, Medicaid, or private payors send money. If claims are denied, billed wrong, or paid late, owner draws can stop even when revenue looks strong.
This driver includes collections timing, accounts receivable, denial rate, and reserve policy. For this model, recurring fixed burden is at least $7,500 per month in overhead plus $100,000 per year for the director, or about $15,833 per month before any care labor is paid.
Hold Cash Before Owner Pay
Track cash, not just booked revenue. Measure days to collect, denied claims, and the cash balance needed to cover payroll, compliance, and growth. If collections slip, the owner’s take-home should wait until reserves are funded, because fixed costs still hit every month.
Set a payroll reserve first.
Model payer delays by source.
Watch AR aging every week.
Hold back draws until cash clears.
Here’s the quick math:$7,500 monthly overhead plus $100,000 director pay means the business needs steady collections just to fund recurring fixed costs. If receivables lag, distributable profit can look fine on paper while cash is tied up in unpaid claims.
6
Home Health Care Agency Business Plan
30+ Business Plan Pages
Investor/Bank Ready
Pre-Written Business Plan
Customizable in Minutes
Immediate Access
Compare lean, base, and high owner income cases
Owner income table
Owner pay stays at the director salary until care wages, reserves, debt service, and taxes are clear enough to support distributions. Higher revenue improves room for upside, but it does not guarantee take-home pay.
Low, base, and high cases show how staffing and care volume affect owner pay.
Scenario
Low CaseDownside case
Base CaseModeled case
High CaseUpside case
Launch model
This is the weaker earnings path, where the owner mainly takes the director salary.
This is the middle path with scaled care volume and a fuller clinical team.
This is the stronger earnings path, with mature-year volume and better fixed-cost spread.
Typical setup
First-year staffing supports $879,540 in annual revenue, or $73,295 a month, with 150% non-labor variable costs and $7,500 in monthly fixed overhead; owner pay is the $100,000 director salary, not distributions.
$3,119,940 in annual revenue with 136% non-labor variable costs and a larger clinical team still leaves owner income at the $100,000 director salary until extra cash is proven.
$8,251,200 in annual revenue, or $687,600 a month, with 122% non-labor variable costs and mature-year staffing, but owner income still starts with the $100,000 director salary before distributions are counted.
Cost drivers
First-year staffing
150% non-labor variable costs
$7,500 fixed overhead
$100,000 director salary
$73,295 monthly revenue
$3,119,940 annual revenue
136% non-labor variable costs
larger clinical team
director salary
cash still tied up in care delivery
$8,251,200 annual revenue
122% non-labor variable costs
mature-year staffing
$687,600 monthly revenue
director salary
Owner income rangeBefore owner reserves
$100,000 salarySalary only
$100,000 salaryModeled salary
$100,000 salaryUpside salary
Best fit
Use this to stress-test the first operating year and check cash pressure before distributions.
Use this as the core planning case for budgets, staffing, and lender talks.
Use this to test scale and see when distributions could start after wages, reserves, debt service, and taxes.
!
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
The researched model supports a $100,000 Agency Director salary if the owner fills that role Distributions are not calculable from the supplied data because skilled nurse, therapist, and aide wage rates are missing Revenue ranges from $879,540 in the first year to $8,251,200 in the mature year, but revenue is not take-home
Profit timing depends on census ramp, staffing, collections, and labor cost The model reaches $73,295 monthly revenue in the first year, with $7,500 monthly fixed overhead and $100,000 annual director salary That looks promising before direct clinical payroll, but the real profit date needs wage rates, payer timing, and reserve targets
Not necessarily, but payer mix changes the model Medicare, Medicaid, private insurance, VA programs, and private pay can carry different rates, authorization rules, denial risk, and cash timing This forecast uses service prices from $60 to $170 per treatment, but it does not provide billing, certification, coding, or reimbursement-rule advice
Owner pay is most affected by active census, reimbursement, billable volume, direct labor, overhead, and collections In this model, non-labor variable costs fall from 150% to 122% of revenue, fixed overhead is $7,500 monthly, and director pay is $100,000 annually Direct care payroll remains the largest missing input
Improve staffed, collectible volume before adding overhead Raise capacity, reduce cancellations, tighten billing, and match clinicians to profitable care plans The model grows monthly revenue from $73,295 to $687,600 as staffing and capacity rise, but owner draws should wait until payroll, reserves, compliance costs, and reimbursement delays are covered
About the author
James Carter
Startup Guide Author
James Carter is a startup guide author at Financial Models Lab who focuses on startup budget assumptions for founders working with limited capital. He studies common expenses, revenue drivers, and launch requirements to help readers plan for rent, staff, equipment, and supplies. His small business startup guides connect business ideas with realistic startup budgets in a clear, practical way.
Choosing a selection results in a full page refresh.