How To Open A Home Health Care Agency With A 12-Clinician Launch Plan
You’re opening a regulated care business, so the launch path starts with state licensing, service scope, qualified leadership, policies, referral outreach, and intake readiness The model period runs from Month 1 to Month 60, with a Year 1 launch team of 3 skilled nurses, 2 physical therapists, 1 occupational therapist, 1 speech therapist, and 5 home health aides Before go-live, validate census ramp, payer mix, payroll pressure, and cash runway
Time to Open6 monthsSetup windowLaunch Sequence6 stagesCompliance firstKey BottleneckLicense gateState rulesFirst Revenue StepBillable visitsIntake ready
Launch timeline
Short web summary of the launch plan; the XLSX export holds the detailed Gantt Chart.
Do you need a license to start a home health agency?
Yes, start a Home Health Care Agency as if licensing, registration, or certification applies before marketing or intake; skilled home health, non-medical care, Medicaid, and Medicare certification can follow different paths, so confirm state rules and track What Is The Most Critical Indicator To Measure The Success Of Your Home Health Care Agency? once operations begin.
Check first
Verify state home health agency licensing
Confirm administrator requirements
Review clinical supervision rules
Check 50-state rule differences
Do before intake
Write required policy documents
Bind required insurance
Prepare for state survey expectations
Review Medicare rules under 42 CFR Part 484
What are the common mistakes starting a home health agency?
The biggest mistakes starting a Home Health Care Agency are underestimating licensing, hiring clinical leadership too late, and opening without strong referral sources or tested documentation workflows. Year 1 fixed overhead is about $75k per month before payroll, and an agency director adds another $100k per year if billing lags or census grows slowly, so cash pressure shows up fast. Prove compliance first, staff to real capacity, then sell into referral channels.
Compliance first
Don’t treat licensing as simple.
Hire clinical leadership early.
Use complete policies from day one.
Test documentation workflows before launch.
Cash and referrals
Open only with real referral sources.
Watch $75k monthly overhead closely.
Plan for the $100k director cost.
Match staffing to actual census.
How long does it take to open a home health agency?
A Home Health Care Agency usually takes several months to open, not one fixed date. The model may start in Month 1, but that is setup time, not approval time, and delays grow when state licensing review, policy work, staffing, payer enrollment, or billing testing run late. If Medicare certification is required, the timeline can stretch further.
Main delay drivers
State licensing review can slow launch.
Policies and procedures must be ready.
Hire an administrator and clinician early.
Recruit nurses and therapists before outreach.
What must work first
Finish accreditation or survey readiness.
Complete payer enrollment before referrals scale.
Set up the EHR and billing workflow.
Test claims before taking live volume.
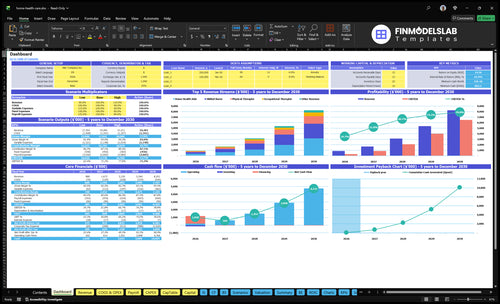
Home Health Care Agency Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Confirm what must be ready before accepting patients
Launch readiness checklist
This is a go-live approval checklist before opening a home health care agency.
1Licensing
State licenses approvedCritical
The agency cannot bill or open without the right state and service licenses.
Entity and tax setup doneCritical
Clean entity and tax setup avoids delays in banking, payroll, and contracts.
Insurance policies boundCritical
General and liability coverage should be active before the first patient visit.
2Clinical rules
Policies and procedures signedCritical
Written rules keep care, documentation, and escalation steps consistent.
HIPAA privacy controls liveCritical
HIPAA privacy rules protect patient data before intake and charting start.
Incident reporting definedHigh
Clear incident steps reduce risk when care events or complaints happen.
3Staffing
Administrator hiredCritical
The agency needs one person accountable for daily execution from day one.
Clinical supervisor hiredCritical
Clinical oversight must be in place before staff take patient assignments.
Backup coverage scheduledHigh
Backup coverage protects visits if a nurse, therapist, or aide cancels.
4Systems
EHR configuredCritical
The EHR (electronic health record) must work before any patient chart opens.
Eligibility and intake testedHigh
Tested intake and eligibility checks help avoid bad starts and denied claims.
Billing and claims testedHigh
A clean billing flow is needed to collect cash after the first visits.
5Referrals
Referral list builtHigh
A live referral list matters because home care demand starts with local partners.
Scheduling workflow readyHigh
Scheduling must match staff capacity so visits do not stack up or slip.
First care starts mappedMedium
The first patient path should be clear before marketing or outreach begins.
6Cash and go-live
Cash runway reviewedCritical
The model shows minimum cash of $862k in Month 2, so runway needs review.
Overhead budget approvedCritical
Fixed payroll and office costs must be funded before the agency opens.
Go-live signoff completeCritical
Do not launch if licenses, documentation, billing, or staffing coverage are still open.
Want the six launch drivers that decide go-live readiness?
1Licensing
License gate
Written approval and complete policies keep intake closed until survey-ready, cutting rejected referrals.
2Staffing
12 staff
Year 1 team of 12 field clinicians and supervision determines who you can see first.
3Clinical Ops
Visit docs
Tested forms and EHR templates turn visits into billable records and cut compliance risk.
4Referral Pipeline
799 visits
Named referral sources and fast follow-up support the 799 monthly visit target.
5Billing Stack
Claims live
Tested intake, eligibility, scheduling, and claims flow turn visits into cash sooner.
6Cash Runway
$862K
Minimum cash is $862K, so slow census can squeeze payroll before collections stabilize.
Licensing, Certification, And Compliance Path
Licensing Comes First
Home health agency licensing is the first gate, not an admin task. Whether the agency will serve skilled care, non-skilled care, or seek Medicare or Medicaid participation changes the launch path, the policy set, and the survey work needed before first patient intake.
The real launch risk is starting outreach before approval. If the state license, insurance, written policies, and survey readiness are not locked, referrals can get rejected and opening can slip. No patient intake before authorization is the clean rule here.
Verify Before You Market
Build the launch file around written confirmation of requirements, a complete application, approved policies, and an assigned compliance owner. That means the founder knows the state’s rules, service scope, payer path, and any survey step before promising start dates to hospitals, physicians, or discharge planners.
The readiness signal is simple: documents submitted, policies approved, insurance in place, and no open questions on licensure. Once that is true, launch can start with safer go-live timing and fewer denied referrals. If any part is missing, hold marketing and intake.
1
Qualified Leadership And Staffing
Qualified Staffing Readiness
Staffing is a launch gate, not a back-office task. For a home health agency, the mix of 3 skilled nurses, 2 physical therapists, 1 occupational therapist, 1 speech therapist, and 5 home health aides is what makes licensure, first visits, and day-one scheduling possible. Add the agency director at $100,000 a year, and the model only works if those roles are filled, credentialed, and ready before referrals turn into start-of-care visits.
One missing discipline can stall the whole opening. If referrals land before staff can visit patients, the agency can miss first-patient dates, strain quality, and create compliance risk. The real bottleneck is schedule capacity by discipline, not just headcount. Qualified clinical supervision, backup coverage, and clean credential files have to be in place before go-live, or the agency may open on paper but not in practice.
Build Coverage Before Taking Referrals
Verify every license, credential, and start date first. Confirm the staffing files, onboarding, supervision plan, and backup coverage for each discipline before marketing hard. Here’s the quick math: the Year 1 model needs 11 clinical staff plus 1 director, so one gap can block visits, not just reduce volume. That is the difference between opening on time and scrambling after the first referral call.
Test the schedule, not just the org chart. Make sure each discipline has real visit capacity for week 1, week 2, and the first month, because a full roster with weak availability still delays care. Use a simple readiness check: credential files complete, supervision assigned, onboarding done, backup names listed, and open slots confirmed by discipline. If those items are late, first-day service slips fast.
Complete credential files for every hire.
Assign backup coverage by discipline.
Document qualified clinical supervision.
Finish onboarding before first referral.
Confirm visit slots for week one.
2
Policies, Procedures, And Clinical Operations
Clinical Workflows That Run
Policies and procedures only help if staff can use them on the first visit. For a home health agency, that means intake, care planning, visit notes, infection control, incident reporting, supervision, HIPAA practices, quality checks, and discharge steps all have to match the way nurses, therapists, and aides work in the field.
Readiness shows up when training is done, forms are tested, EHR templates work, and escalation rules are clear. If documentation is weak, billing slows and compliance risk rises, which can delay cash from a $150 skilled nursing visit, a $120 physical therapy visit, or a $60 home health aide visit in Year 1.
Test Before First Admission
Before opening, verify that every workflow can be done without guesswork. That means a new patient can be admitted, a care plan can be assigned, a visit can be documented, and a supervisor can review exceptions the same day. If any step breaks, day-one capacity drops and the launch slips.
Train staff on each workflow.
Test forms in the EHR.
Assign one escalation owner.
Run a sample audit.
Check discharge and incident steps.
One clean note matters more than a binder. If the first chart can pass review, the agency is much closer to serving patients on time and getting paid without avoidable rework.
3
Referral Pipeline And Launch Marketing
Referral Pipeline Readiness
Referral marketing should start before go-live, but only after the compliance path and service scope are locked. If you open outreach too early, you can create demand you cannot admit, which slows first revenue and damages trust with hospitals, physicians, and discharge planners.
The first pipeline should cover hospitals, physicians, discharge planners, rehab facilities, assisted living communities, senior service organizations, and case managers. Weak referral depth makes the Year 1 target of about 799 monthly visits harder to hit, so day-one readiness depends on a clean list, clear geography, and a fast intake path.
Build the Referral List First
Before launch, verify a named referral list, outreach cadence, service area, intake script, response time, and follow-up owner. Here’s the quick test: if a planner calls today, can the team answer, screen, and route a compliant admission the same day?
Keep first clients tied to compliant admissions, not just interest. Document who owns each source, what gets sent, and when follow-up happens, because delayed responses can push the first visit date out and leave staff underused at opening.
Lock service area before outreach.
Test intake script with referrals.
Set same-day response ownership.
Track follow-up after every contact.
4
Intake, Scheduling, EHR, Billing, And Payers
Billing and Intake Readiness
If intake, scheduling, and billing are not wired together before go-live, visits can pile up without turning into cash. For a home health agency, the first real gate is not census; it’s whether referrals can be entered, eligibility checked, care scheduled, and notes turned into clean claims or invoices on day one.
That matters because the EHR system, the electronic health record, must support the full path from referral to payment. Modeled system fees equal 40% of Year 1 revenue, so weak setup is a launch and cash problem, not just an IT issue. If documentation is sloppy, billing slows and payroll pressure rises even when visits start coming in.
Test the Claim Path Before Opening
Before launch, verify the full workflow: referral intake, eligibility checks, visit scheduling, care documentation, billing codes or invoice rules, claim review, denial tracking, and the collections dashboard. One weak link can delay first revenue and create rejected claims, which is especially painful when services include $150 skilled nursing visits, $120 physical therapy visits, and $60 home health aide visits.
Load payer setup before first referral.
Test notes against billing rules.
Assign denial follow-up to one owner.
Track cash timing against payroll dates.
Make the EHR workflow live only after a dry run shows clean handoff from intake to claim. If billing lag starts while census grows, cash can tighten fast, so the launch plan should include a tested collections dashboard and clear rules for who fixes missing documentation, who resubmits claims, and how fast payer issues get escalated.
5
Cash Runway And Patient Ramp Assumptions
Cash Runway Before Go-Live
This launch driver matters because payroll, overhead, and care coverage start before collections settle. At steady early capacity, modeled monthly revenue is about $73,295 from about 799 visits, but direct and variable costs run at 150% of revenue before payroll, so cash can drain fast if intake or billing lags.
The opening risk is simple: if census builds slowly, the agency still has to fund a $7,500 monthly overhead base and an agency director at $100,000 per year before the visit stream is stable. That makes the cash buffer and staffing plan a day-one issue, not a back-office detail.
Verify Runway, Then Pace Hiring
Before opening, validate payer mix, billing lag, clinician utilization, and the monthly visit ramp tied to that 799-visit model. Here’s the quick math: if revenue is delayed while costs start now, the business can’t rely on early collections to fund wages, coverage, or fixed overhead.
Build the cash plan around the slow case, not the best case. Confirm the minimum runway needed to cover overhead, director pay, and starting clinical coverage, then tie hiring and schedule depth to actual referral flow so you do not overstaff before visits convert.
Start with state licensing research, service scope, entity setup, insurance, policies, qualified leadership, EHR, billing, and referral outreach The modeled Year 1 launch team has 12 field care staff At steady early capacity, the plan supports about 799 monthly visits and $733k monthly revenue before payer delays, payroll, and collections timing
Plan for several months, not a fixed date State licensing, Medicare certification, survey readiness, administrator hiring, clinical staffing, policy preparation, payer setup, and billing testing can all move the timeline The model runs Month 1 through Month 60, but Month 1 is an operating label, not a guaranteed approval date
Not always, but the agency needs qualified clinical leadership and compliant supervision The Year 1 staffing plan includes 3 skilled nurses, 2 physical therapists, 1 occupational therapist, 1 speech therapist, and 5 home health aides If the owner is non-clinical, hiring the right administrator and clinical supervisor becomes a launch-critical step
Licensing gaps, incomplete policies, late clinical hiring, weak billing setup, and payer enrollment delays cause the most pain Fixed overhead in the model starts at $75k per month before wages, and the agency director adds $100k per year Delays matter because cash leaves before visits become collected revenue
First revenue starts with compliant admissions that lead to documented, billable visits Build referral relationships with hospitals, discharge planners, physicians, rehab centers, senior communities, and case managers before go-live In the Year 1 model, visit pricing ranges from $60 for home health aide services to $150 for skilled nursing visits
About the author
Eric Dawson
Startup Cost Researcher
Eric Dawson is a startup cost researcher at Financial Models Lab who writes practical guides for founders planning their first business. He focuses on break-even planning and comparing business ideas by cost and effort, with an emphasis on realistic small business planning. Eric’s work keeps attention on useful numbers, clear assumptions, and realistic expectations for business plans.
Choosing a selection results in a full page refresh.