How Much House Call Doctor Owners Make: $103M Year 1 Profit
A house call doctor service owner can make strong income only if completed visit volume, collections, and staffing stay disciplined In the researched assumptions, Year 1 revenue is about $218M, with $103M operating profit after supplied variable costs, fixed costs, and a $280k Medical Director salary By Year 5, modeled revenue reaches $2421M and operating profit reaches $1962M, but that figure excludes taxes, debt service, reserves, reinvestment, and any provider payroll not included in the data Treat these as planning assumptions, not wages, guaranteed distributions, tax advice, or a substitute for a full financial model
Owner income$199-$232/visitNet margin40%-73%Revenue for target pay$2.2MBusiness difficultyMedium
Want to test your owner pay?
Owner income calculator
Estimate owner take-home and the target-pay gap from monthly revenue, margin, costs, reserves, and target pay.
!
Planning note: Research-based planning estimate only; not guaranteed salary, tax advice, or owner distribution advice.
Want the six main income drivers?
1
Visit Volume
916-8.7k/mo
More completed visits drive most of the revenue, scaling from 916 monthly visits in Year 1 to 8,679 in Year 5.
2
Visit Value
$199-$232
A higher net collection per visit lifts take-home fast because the gain multiplies across every completed house call.
3
Staffing Mix
3-25 FTE
The split between physician time, nurse practitioners, and other clinicians sets labor cost and visit capacity.
4
Payer Timing
Cash lag
Insurance lag ties up cash, while faster reimbursement keeps more of each visit available for payroll and owner draws.
5
Route Efficiency
5%-6%
A tighter service area lets each clinician fit more visits into a day and keeps fuel and vehicle costs near the 5% to 6% range.
6
Overhead Reserve
$36.7K/mo
Fixed overhead totals $36.7K a month, and the $832K cash trough in Month 2 means reserve discipline protects owner pay.
How do you check owner income in the House Call Doctor Service model?
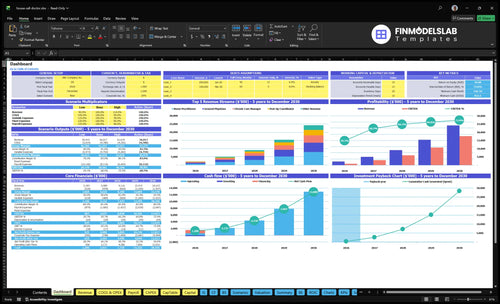
This dashboard shows revenue, margin, costs, reserves, and owner take-home assumptions; open the model.
Owner-income model highlights
Owner pay split clearly
Revenue and margin charts
3 to 15 physicians
4 to 25 nurse practitioners
50% to 90% utilization
$367k monthly overhead
How much can a house call doctor charge per visit?
For a House Call Doctor Service, use net collections, not sticker price: Year 1 visits can range from $150 for chronic care management to $300 for geriatric specialist visits, and the weighted average collection is about $199 per completed visit, rising to about $232 by Year 5. What you actually keep shifts with cash-pay, concierge, Medicare, Medicaid, commercial insurance, employer contracts, and facility contracts, plus geography, coding, credentialing, medical necessity, patient responsibility, and collection rate. So the quote is only step one; the real number is the collected amount.
Year 1 to Year 5
$150 to $300 per visit.
$199 average collection in Year 1.
$232 average collection by Year 5.
Count completed visits, not billed charges.
What moves the number
Cash-pay and concierge speed cash.
Medicare and Medicaid change rules.
Commercial, employer, and facility contracts vary.
Geography and coding move collections materially.
How many house call visits per day to be profitable?
There’s no universal daily visit count, but this House Call Doctor Service model starts at 916 completed visits per month, or about 31 visits per day across all providers over 30 days; see How Increase House Call Doctor Service Profits? for the profit levers. The count depends on collections, travel time, visit length, no-shows, staffing, and how tightly routes are scheduled.
Visit math
Start with 916 visits/month
Run about 31 visits/day
Spread across all providers
Track completed visits, not bookings
Profit levers
Year 1 revenue: $1,819k/month
Fixed overhead: $367k/month
Medical Director: $280k/year
Protect quality and provider workload
What are the main house call doctor business expenses?
House Call Doctor Service costs split into two buckets: visit-linked costs and fixed overhead. For a quick read, the How Much To Start House Call Doctor Service? page helps frame the setup, but the biggest operating drag is still the recurring base cost. Year 1 visit-linked costs are 20% of revenue, and fixed overhead is listed at $367k per month.
Visit-linked costs
20% of revenue
45% supplies
55% lab and diagnostic fees
60% fuel and vehicle maintenance
Fixed overhead
$367k per month total
$12k malpractice
$85k vehicle fleet lease
$65k admin hub rent
Billing and claims fees make up the rest of the variable load at 40%, so the visit margin can look healthy on paper. But owner take-home still gets squeezed after provider payroll, reserves, taxes, and reinvestment.
Other monthly overhead
$45k marketing
$22k software
$18k IT
$12k licensing
What this means
Gross margin can look strong
Fixed costs stay high each month
Payroll cuts owner cash fast
Reserves and taxes matter
Key Takeaways
Completed visits drive most revenue growth.
Net collections per visit shape revenue quality.
Payer mix changes cash timing and denial risk.
Overhead and reserves decide owner take-home.
Owner income scenario table objective
Owner income scenarios
Owner income moves fast here because visit volume, collections per visit, staffing load, and fixed overhead all rise and fall together.
Compare downside, modeled, and scale cases for owner income.
Scenario
Low CaseStaffing and payer risk
Base CaseModeled run rate
High CaseScale with timing risk
Launch model
This is the downside case, with fewer visits, weaker collections, and thinner route productivity.
This is the source Year 1 case, with 916 monthly visits and $199 average collections.
This is the Year 5 scale case, with 8,679 monthly visits and higher collections.
Typical setup
Visits run below Year 1 capacity, collections slip, marketing rises, and payroll stays heavy for the volume.
The model runs 3 General Physicians, 4 Nurse Practitioners, 1 Geriatric Specialist, 2 Chronic Care Managers, and 1 Post Op Coordinator at Year 1 capacity.
Staffing expands to Year 5 capacity, collections improve, and the model pushes more volume through the same service mix.
Cost drivers
Lower visit volume
slower collections
higher marketing spend
more payroll per visit
weaker route efficiency
916 monthly visits
$199 average collections
20% variable costs
$280k Medical Director salary
$2.183M annual revenue
8,679 monthly visits
$232 average collections
16% variable costs
higher staffing load
$24.215M annual revenue
Owner income rangeBefore owner reserves
Below $867kPressure case
$867kCore plan
$17.7MUpside case
Best fit
Use this to test weak referrals, slower claims, and underused clinicians.
Use this for budget, hiring, and lender planning.
Use this to test expansion upside, staffing depth, and payer timing strain.
!
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
House Call Doctor Service Core Six Income Drivers
Completed visit volume
Completed Visit Volume
Completed visit volume is the main revenue capacity lever here, because the model counts capacity-adjusted visits, not theoretical appointment slots. It runs from 916 visits per month in Year 1 to 8,679 per month in Year 5, so the business can scale only if providers actually finish more house calls. Each completed visit adds collected revenue, so missed visits hit owner pay fast.
What can shrink volume: travel gaps, documentation delays, complex cases, no-shows, a wide service radius, and provider burnout. More visits help income only if clinical quality stays safe. If the schedule gets tighter but care gets rushed, you can lose revenue later through rework, complaints, and churn. One clean rule: more completed visits should mean more cash, not more risk.
Track and Protect Visit Capacity
Track completed visits per provider per day, not booked slots. Break it down by ZIP code, visit type, no-show rate, drive time, and documentation time, so you can see where capacity leaks. Here’s the quick math: moving from 916 to 8,679 monthly visits is about a 9.5x jump, so small process gains matter a lot.
Use routing, reminder calls, and same-day charting to keep visits moving. If one provider is carrying too many complex cases or too much windshield time, volume drops and owner income follows. The target is simple: keep the schedule full, keep care safe, and keep the visit actually closed out.
Route efficiency and service area density
Route Density
When house calls are spread across a wide area, the service can look full but still pay poorly. In the model, fuel and vehicle maintenance run at 60% of revenue in Year 1, which means only 40% is left before fixed overhead; by Year 5, that falls to 50%, so margin improves if routes stay tight.
Here’s the quick math: every $100,000 of revenue leaves about $40,000 in Year 1 and $50,000 by Year 5 before overhead. The inputs are completed visits, miles per stop, paid windshield time, ZIP code mix, visit type, and provider skill. Dense routes raise cash by fitting more billable care into the same day.
Cluster by ZIP and visit type
Track visits per route hour, miles per completed visit, and % of stops in the same ZIP. Group appointments by ZIP code first, then by visit type and provider skill. That cuts drive time, lowers empty miles, and helps patients get seen on time. Dense routing only helps if it does not stretch clinical quality or create rushed visits.
Measure windshield time daily.
Cluster stops before booking.
Match visit type to skill.
Test tighter service zones.
What this changes is owner pay: less time driving means more completed visits and less variable cost, so more cash is left after visit labor and vehicle costs. Broad geography can hide weak economics until fuel, maintenance, and late arrivals start eating the month.
Overhead, reserves, and reinvestment
Overhead Before Owner Draw
In this house call model, overhead is the cash wall between collected revenue and owner take-home. Fixed costs total $367k per month, led by $85k for vehicle fleet lease, $65k for admin hub rent, $45k for marketing, and $12k for malpractice. Owner pay only works after working capital, reserves, taxes, debt service, software, compliance support, supplies, and reinvestment are covered.
This matters because cash timing can break the link between profit and spendable income. Claims lag and vehicle repairs can hit in the same month, so a strong revenue month can still leave the owner short if reserves are thin. The real test is not just profit on paper; it’s whether collected cash clears the $367k fixed base and still leaves room for delay and downtime.
Protect Cash Before Paying Yourself
Track the monthly fixed-cost base, days of claims outstanding, fleet repair spend, and reserve balance. If the practice cannot cover the full $367k plus near-term timing gaps, owner draw should wait. That keeps one bad billing month or one broken vehicle from turning into a cash crunch.
Forecast overhead by line item monthly.
Separate reserves from operating cash.
Set owner draw after taxes and debt.
Watch claims lag and repair spikes.
Reinvest before increasing personal pay.
Payer mix and reimbursement timing
Payer Mix and Cash Timing
Payer mix changes both revenue per visit and cash timing. Cash-pay and concierge visits usually collect faster, but they can narrow demand. Medicare, Medicaid where applicable, and commercial plans may widen volume, but they add coding, medical necessity proof, credentialing, denials, and billing lag.
For the owner, this driver changes how fast visits turn into take-home pay. Model collections per visit, days to cash, denial rate, and patient responsibility, not billed charges. Employer or facility contracts can improve scheduling density, but payer mix should stay a sensitivity, not a promise.
Track Collections, Not Charges
Split visits by payer bucket and compare collected cash, days to cash, and denials each month. That shows whether a higher-volume payer is actually improving owner income or just delaying it.
Measure collections by payer monthly.
Track denial reasons and appeals.
Watch patient balances by visit type.
Test contract terms before scaling.
If billing lag grows, cash flow tightens even when visit volume looks fine. More visits do not equal more pay unless the money clears fast enough to cover payroll, overhead, and owner draw.
Net collections per completed visit
Net collections per completed visit
Net collections per completed visit is the cash you actually keep for each house call, not the charge on the claim. In year 1, the weighted average is about $199 per completed visit, with service prices from $150 to $300. By year 5, the average rises to about $232 as higher-priced visit types take a bigger share.
This drives owner income because every collected dollar lifts gross margin and pay. Use collected cash, not billed charges, because denials, patient balances, payer contracts, and claim timing all change what lands in the bank. A $10 move across 916 monthly visits changes annual revenue by about $109,920 before costs.
Track cash, not charges
Measure cash collected ÷ completed visits each month, then split it by payer, visit type, denial rate, patient responsibility, and days to cash. That tells you whether pricing, payer mix, or billing lag is hurting take-home income. If collections per visit drift down, the owner's draw usually follows.
Completed visits by visit type
Collected cash by payer
Denials and patient balances
Days to cash
Price mix across visit types
Push higher-priced visit types only when the billing team can collect cleanly. The year 5 benchmark of $232 depends on a richer mix, not wishful pricing. If claims slow down, keep more working capital before increasing owner pay.
Clinical staffing model
Clinical staffing mix
Staffing is the main cap on owner income here. The model scales nurse practitioners from 4 to 25 and general physicians from 3 to 15 over five years, so each hire can raise completed visits and collections. But pay only improves if each clinician is fully loaded and the schedule stays tight; empty travel time or slow credentialing turns payroll into drag.
Early owner-physician delivery can keep payroll lean, but it also caps visits. Once employed clinicians come in, model provider payroll, supervision, licensing compliance, scheduling support, and quality checks separately from owner draw. The supplied $280k Medical Director salary is one input; it does not replace the rest of clinical labor costs.
Track clinician capacity fast
Track visits per clinician per day, paid travel time, no-shows, and case mix. Here’s the quick math: if more staff do not lift completed visits faster than payroll grows, owner income falls. Use one schedule view for demand, one for capacity, and one for credentials so you can see when the next hire actually adds margin.
Before adding staff, test whether the role will improve cash, not just volume. Watch collections per visit, labor as a share of revenue, and days to fill the schedule after hiring. If onboarding takes too long, the practice can look busier and still pay the owner less.