House Call Doctor Service Startup Costs: $85K CAPEX Plus Runway
This guide covers a researched house call doctor startup budget for the first operating year, including $85,000 in portable diagnostic equipment, $36,700 in monthly fixed overhead, and $761,000 in Year 1 wages It separates CAPEX from pre-opening expenses and working capital so you can size the opening funding need without treating planning ranges as vendor quotes
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimate the one-time capitalized startup assets for a physician home-visit practice, including equipment, vehicle setup, and launch hardware only.
!
What's excluded This calculator covers capitalized startup assets only. It excludes inventory, payroll runway, deposits, debt service, working capital, rent, insurance premiums, marketing, subscriptions, consumables, taxes, licensing, and other operating expenses.
Calculate Fuding Needs
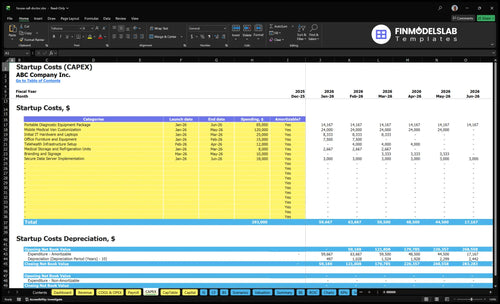
Startup cost summary
This table summarizes the main startup equipment, setup, and launch cash needs for a house call medical practice.
Highlighted CAPEX$250,000Base planning example
Excluded cash needs$832,000Outside CAPEX total
Funding need$1,082,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Portable diagnostic equipment package
$85,000
In-home exam tools and portable diagnostics
Yes
Mobile medical van customization
$120,000
Vehicle fit-out for house calls and storage
Yes
Initial IT hardware and laptops
$25,000
Field devices for care, billing, and coordination
Yes
Telehealth infrastructure setup
$12,000
Remote visit setup and secure scheduling tools
Yes
Medical storage and refrigeration units
$8,000
Safe storage for supplies and temperature-sensitive items
Yes
Opening cash buffer
$832,000
Month 2 cash trough from $761k Year 1 wages and $36.7k fixed overhead
Startup cost swings are driven by provider count, vehicle coverage, and working capital. Lean, Base, and Full help match launch scope to the market and payer mix.
Lean, Base, and Full launch scenarios for a house call doctor service
Scenario
Lean LaunchFounder-Led
Base LaunchBase Multi-Provider
Full LaunchExpanded Coverage
Launch model
A founder-physician starts with one tight service area and keeps the team lean.
This is the researched anchor model with a full core team and standard launch scope.
This version adds more providers, broader coverage, and stronger patient outreach.
Typical setup
It uses fewer hires than the source model, lower vehicle coverage, and tighter marketing.
It uses $85,000 of CAPEX, $36,700 of monthly fixed overhead, and $761,000 of Year 1 wages.
It pulls forward later staffing, including Year 2 counts of 5 General Physicians and 8 Nurse Practitioners, plus larger working capital.
Cost drivers
Founder coverage
fewer hires
lower vehicle use
tighter marketing
lean working capital
$85k CAPEX
$36.7k monthly overhead
$761k Year 1 wages
standard fleet
core provider mix
More providers
broader coverage
stronger marketing
larger working capital
pulled-forward staffing
Planning rangeCAPEX only
Lower funding bandLower cash need
Base funding bandModel anchor
Higher working-capital bandMore cash need
Best fit
Best for a founder-physician testing one area with tight cash.
Best for an operator-ready launch with steady demand and a standard metro footprint.
Best for a larger market with strong referral flow, payer support, and enough cash for faster staffing.
!
Planning note: These scenario ranges are researched planning assumptions, not exact quotes or vendor bids.
How should founders fund a house call doctor financial plan?
For a House Call Doctor Service, founders should fund the plan as a launch cash need, not just a vehicle or software buy. Here’s the quick math: start with $85,000 CAPEX, add quoted pre-opening costs, then add runway months against the operating base of $36,700 in fixed overhead plus about $63,400 in monthly wages. Keep receivables reserve separate for reimbursement lag, and tie the total to credentialing, payer mix, vehicle readiness, and patient ramp.
Build the funding base
$85,000 CAPEX first
Add pre-opening expenses
Add runway months next
Use $100,100 monthly base
Keep cash risks separate
Show reimbursement lag separately
Reserve cash for collections delay
Link funding to visit ramp
Test timing in a financial model
What staffing costs drive a physician home visit startup budget?
For the House Call Doctor Service, staffing is the main Year 1 cost: the plan totals $761,000 in wages, or about $63,400 per month. That covers 3 General Physicians, 4 Nurse Practitioners, 1 Geriatric Specialist, 2 Chronic Care Managers, and 1 Post Op Coordinator, plus a $280,000 Medical Director, $95,000 Practice Administrator, and core support roles. A founder-physician start can lower burn, but hired coverage gives faster patient access and still needs billing and dispatch support from day one.
Clinical coverage
Founder-led start lowers payroll.
Hired clinicians raise monthly burn.
3 physicians and 4 NPs add capacity.
Unused provider time can linger early.
Back office burn
$280,000 Medical Director anchors cost.
$95,000 Practice Administrator adds control.
Billing support keeps claims moving.
Dispatch coverage helps visits flow.
What hidden costs should a house call doctor service budget for?
A House Call Doctor Service needs to budget for both setup delays and monthly burn. The hidden hits are malpractice deposits and premiums, payer credentialing delays, billing setup, and unused clinician time; if launch slips while staff are already hired, you can still carry about $100,100 per month in payroll and fixed overhead before visit revenue. For a quick owner view, see How Much Does An Owner Make From House Call Doctor Service? and remember recurring costs like $12,000 malpractice, $1,200 licensing and dues, $2,200 EHR and scheduling, and $1,800 telecom and IT support.
Pre-open costs
Malpractice premiums start at $12,000 monthly.
Plan for payer credentialing delays.
Budget for billing setup and claims rules.
Cover HIPAA documents and clinical policies.
Ongoing drag
$1,200 monthly licensing and dues.
$2,200 for EHR and scheduling.
$1,800 for telecom and IT support.
40% Year 1 billing and claims fees.
Key Takeaways
Licensing and credentialing start before claims pay.
Equipment is CAPEX; supplies and fees vary.
Software, billing, and tech create monthly cash burn.
Dense routing beats simply hiring more clinicians.
House Call Doctor Service Core Five Startup Costs
Licensing, Credentialing, And Compliance Startup Expense
Pre-Opening Scope
Treat licensing and credentialing as pre-opening cash, not CAPEX. Budget for entity formation, state medical board steps, NPI, Medicare, Medicaid, commercial payer enrollment, HIPAA, legal review, clinical policies, and provider files. The only fixed line here is $1,200 per month for professional licensing and dues starting Month 1.
Quote The Setup
Use quote fields for legal counsel, payer enrollment support, compliance documentation, and credentialing administration because setup fees are not provided. Start with the $1,200 monthly licensing line, then add one-time vendor quotes. This sits in startup cash, before visits bill.
Legal counsel quote
Payer enrollment quote
Compliance docs quote
Credentialing admin quote
Watch The Gap
Credentialing delay is the cash-risk item. Payroll and fixed overhead can start before claims are paid, so the gap can burn cash fast. Track submission dates, follow-up dates, and payer status weekly. If enrollment slips, hold extra runway for wages, software, and insurance.
Front-Load Compliance
Set aside time and cash for board filings, payer paperwork, and policy review before the first visit. That keeps the launch billable sooner and avoids a common mistake: hiring before enrollment is active and then waiting on receivables with no claims in flight.
Staffing Readiness, Travel Operations, And Launch Marketing Startup Expense
People and vehicles
For a house-call launch, this bucket covers people, cars, and outreach, not clinical gear. The anchor is $761,000 in Year 1 wages, plus $4,500 a month for marketing and patient outreach and $8,500 a month for fleet lease; fuel and maintenance add another 60% in Year 1.
Budget inputs
Build the budget from headcount, months of coverage, and launch channels. Include contractor onboarding, route planning, branded materials, website, local search setup, referral outreach, call answering, mileage systems, launch campaigns, and dispatcher workflows. Here’s the quick math: $4,500 x 12 = $54,000 for outreach, and $8,500 x 12 = $102,000 for vehicles.
Use signed quotes for setup fees.
Separate lease, fuel, maintenance.
Track visits per routed mile.
Route first
Keep this lean by opening in dense zip codes and using one dispatch flow for calls, mileage, and routing. Don’t add clinicians before the schedule fills; the real lever is dense routing, not just more clinicians. Tie staffing to visit capacity using the Year 1 assumptions: 650% General Physicians, 600% Nurse Practitioners, 500% Geriatric Specialists, 700% Chronic Care Managers, and 550% Post Op Coordinators.
Cash timing
What this estimate hides is timing: wages, fleet, and outreach start before visit revenue does, so contractor onboarding and call coverage must be ready before launch week. If routing stays thin, fuel and maintenance rise fast and clinician time gets wasted.
Medical Equipment And Portable Diagnostics Startup Expense
What It Covers
$85,000 covers the durable portable diagnostic package from Month 1 through Month 6: exam bags, stethoscopes, blood pressure cuffs, pulse oximeters, otoscopes, thermometers, ECG or point-of-care testing if offered, sharps containers, PPE, storage, and replacement kits. Classify this as CAPEX; buy disposables as startup supplies or working inventory.
Budget Inputs
Use units × unit price, vendor quotes, and months of coverage to set the budget. The mix changes by visit type, clinician count, service radius, and whether diagnostics are done in-house or sent out. One line matters most: separate equipment from consumables, because Year 1 medical supplies and disposables are modeled at 45% of revenue.
Quote each device, not one lump sum.
Track in-house test volume separately.
Match stock to visit demand.
Keep Cash Tight
Don’t load up on spare inventory before visit volume is clear. Use replacement kits and consumables for the first six months, then reorder to actual use. If testing is sent out, keep the 55% laboratory and diagnostic fee line separate so equipment spend does not hide operating cost. That keeps cash tied to care, not idle stock.
Stage purchases by route density.
Reorder only after usage checks.
Keep send-out fees off equipment.
Model the Mix
Here’s the clean split: durable tools sit in CAPEX, while disposables flow through startup supplies and working inventory. Then model Year 1 at 45% medical supplies and disposables and 55% laboratory and diagnostic fees. If your service radius grows or in-house testing rises, the stock and fee mix will move fast.
Malpractice, Business Insurance, And Risk Management Startup Expense
Coverage Stack
Treat insurance as a recurring cash need, not a one-time setup fee. The anchor is $12,000 per month for malpractice starting Month 1, plus professional liability, general liability, cyber liability, workers’ compensation if you hire, and commercial auto or non-owned auto coverage.
Quote Drivers
Build the estimate from quote inputs, not guesses. Use specialty, claims history, state, visit type, provider mix, hiring plan, and vehicle use to size the premium. Add policy deposits, legal review, and compliance setup so your opening cash plan shows the full monthly run rate.
Separate each coverage line
Ask for deposit amounts
Track provider mix changes
Control Risk
Shop multiple carriers early, but do not strip out cyber or auto coverage to save cash. The cleanest savings come from better loss data, tight scope of practice, safe driving rules, and accurate staffing plans. What this estimate hides is simple: a bad claims record or a new state can move pricing fast.
Compare limits, not only price
Keep driving rules tight
Update quotes after hiring
Funding Burn
A staffed launch can burn about $100,100 per month before variable costs and claim collections once malpractice, vehicles, software, rent, and payroll are live. If funding only covers the first premium, cash gets tight before receivables start to catch up.
EHR, Billing, Scheduling, And Mobile Technology Startup Expense
Tech stack cost
For a house-call practice, the tech line starts with $2,200 a month for EHR and scheduling plus $1,800 a month for telecom and IT support. Add separate setup fees for billing or revenue-cycle management, integrations, and secure messaging. One clean rule: treat subscriptions, setup, devices, and transaction fees as four different buckets.
What to buy
Classify tablets, laptops, printers, and scanners as device CAPEX. Keep payment processing and the 40% Year 1 billing and claims processing fee as transaction cost, not hardware. Estimate it with unit count × unit price, then add quoted setup fees and months of software coverage. That keeps startup cash needs honest.
Count devices by user
Get written setup quotes
Separate CAPEX from fees
Close notes fast
Home-visit cash gets stuck when notes are thin or coding is off. Use visit templates, same-day charting, and a billing review before claims go out. Missing home details can delay payment, so build the workflow around complete notes, diagnosis codes, and telehealth backup if the visit shifts to video.
Chart before end of day
Check codes before submit
Track denials every week
Monthly tech burn
The base monthly tech burn is $4,000 before claims fees, devices, and one-time setup. That means launch budget should split recurring subscriptions from cash you spend once. If you lump them together, you lose sight of burn rate and can’t tell whether growth pain is software cost or collections lag.