How Much Mobile Urgent Care Owners Make at 462+ Monthly Visits
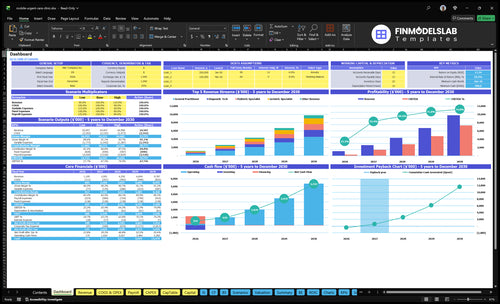
A mobile urgent care owner can model a first-year owner salary of $150,000, plus possible distributions if the business keeps enough cash after costs and reserves Using the researched assumptions, first-year revenue is about $11M from roughly 462 completed visits per month at about $199 collected per visit First-year operating profit before taxes, debt service, reserves, and any unlisted provider compensation is about $449,000 Treat that as planning math, not a guaranteed salary or reimbursement outcome
Owner income$150kNet margin23%Revenue for target pay$645kBusiness difficultyHard
Want to test your owner pay?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
!
Planning note: This is a researched planning estimate only. Actual owner income is not guaranteed and is not tax advice or owner distribution advice.
Want the six drivers that move owner income most?
1
Visits per Day
462/mo
More completed visits push owner income fast because each extra stop adds revenue while fixed costs stay mostly flat.
2
Revenue per Visit
$199
A higher collected amount per visit lifts margin on every call, so pricing and coding drive take-home cash.
3
Provider Labor
60%
Year 1 capacity is only 60%, so filling clinician time is the main way to spread overhead and raise profit.
4
Payer Mix
17%
Cleaner payer mix and billing keep the Year 1 variable clinical and mobile cost load near 17%, so more of each visit becomes cash.
5
Route Utilization
4%
Vehicle fuel and maintenance start at 4%, so tighter routing helps keep travel from eating the visit margin.
6
Overhead Control
$11.5K
The $11.5K monthly fixed base and the $150K owner salary only work if reserves hold through the Month 6 cash dip.
Want to stress-test owner income in Mobile Urgent Care?
Open the Mobile Urgent Care Financial Model Template to test the dashboard, revenue build, staffing, cost assumptions, cash flow, profit forecast, and owner income outputs. It stress-tests visit volume, payer mix, practitioner count, 60% to 85% capacity, and $150 to $280 pricing, with $11,500 monthly overhead and listed payroll, so owner salary stays secondary to income planning.
Owner-income model highlights
Owner salary stays secondary
Revenue and margin outputs
Test 60%-85% capacity
How many visits does a mobile urgent care need to pay the owner?
Mobile Urgent Care needs 462 completed visits per month to support a $150,000 owner salary in Year 1, or about 15 visits per day if open 30 days; What Is The Current Growth Trend Of Mobile Urgent Care? helps frame the demand side. Here’s the quick math: $92,100 monthly revenue, less 17% for supplies, lab, vehicle, and malpractice costs, then $11,500 fixed overhead and payroll.
Visit Target
462 completed visits per month
15 completed visits per day
$199 revenue per completed visit
Booked visits don’t pay bills
Cost Math
$92,100 monthly revenue
17% variable care costs
$11,500 fixed overhead
$12,500 monthly owner pay target
What is the profit margin for a mobile urgent care clinic?
For Mobile Urgent Care, the first-year operating margin is about 41% before taxes, debt service, reserves, and any unlisted provider pay. Gross margin stays near 90% after medical supplies and lab fees, but costs from fuel, maintenance, malpractice, fixed overhead, and payroll push profit down; see How Much Does It Cost To Open, Start, And Launch Your Mobile Urgent Care Business?.
Margin math
90% gross margin after supplies
Lab fees are included there
41% operating margin first year
Before taxes and debt service
Cost pressure
Route time cuts visit density
Vehicle coverage adds fixed cost
Insurance and dispatch add overhead
Billing work also takes margin
How much revenue does a mobile urgent care make per visit?
Mobile Urgent Care collects about $199 per visit in Year 1 on average. Listed prices run from $150 for diagnostic tech visits to $250 for mental health visits, but actual collections move with payer mix, employer contracts, cash-pay rules, claim denials, and ancillary services.
Year 1 pricing
$199 average collected per visit
$150 diagnostic tech visit price
$250 mental health visit price
General, pediatric, geriatric included
What changes collections
Payer mix shifts collected revenue
Employer contracts change paid amounts
Cash-pay rules affect take-home
Denials and add-ons move totals
Key Takeaways
Completed visits drive revenue and spread overhead.
Average collection per visit lifts revenue without extra costs.
Provider staffing raises capacity but adds labor and supervision.
Cash timing, routes, and overhead decide take-home.
Compare low, base, and high mobile urgent care owner income scenarios
Owner income scenarios
Owner income moves with visit volume, capacity, and staffing. Year 1 is lean, Year 3 is base, and Year 5 is high as more providers spread fixed costs.
Lean, base, and high income views by operating scale.
Scenario
Lean CaseLean
Base CaseBase
High CaseHigh
Launch model
This is the lean Year 1 path with 462 monthly visits, about $199 per visit, and 60% capacity.
This is the Year 3 modeled path with 1,701 monthly visits and a fuller operating rhythm.
This is the Year 5 upside path with 3,631 monthly visits and the strongest capacity fill.
Typical setup
It assumes a smaller provider mix, about $11M revenue, a $150,000 owner salary, and about $449,000 operating profit before taxes, reserves, debt service, and unlisted provider compensation.
It reflects 72.5% capacity, more staffing, and about $43M revenue as the schedule fills and fixed costs are spread over more visits.
It assumes 85% capacity, a larger team, and about $98M revenue with more visits flowing through the same fixed base.
Cost drivers
visit volume
60% capacity
owner salary
vehicle and insurance costs
smaller provider mix
visit volume
72.5% capacity
staffing scale
supply use
fixed overhead spread
visit volume
85% capacity
larger team
supply spend
support overhead
Owner income rangeBefore owner reserves
$449,000Lean income
$2.8MBase income
$7.3MHigh income
Best fit
Founders testing a conservative opening month or slower referral ramp.
Operators using Year 3 as the working budget and normal ramp case.
Teams stress-testing scale, staffing, and cash use when demand is strong.
!
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Mobile Urgent Care Core Six Income Drivers
Completed Patient Visits Per Operating Day
Completed Patient Visits Per Day
Booked visits don’t pay bills until they’re completed and collected. In Year 1, the model assumes 462 completed visits per month at 60% capacity, or about 15 visits per day over 30 days. At the stated $199 average collected revenue per visit, that is about $91,938 per month before the $11,500 fixed overhead load.
This driver shapes profit fast. More completed visits spread rent, insurance, software, marketing, and admin across more revenue, so owner pay improves. If cancellations, long drive times, wide service radius, or schedule gaps cut completions, cash flow weakens even when the calendar looks full.
Track the Visits That Actually Finish
Track completed visits per operating day, not just bookings. Break it out by zip code, provider, and time block, then compare booked, arrived, completed, and collected. If completions fall below the Year 1 pace of 15 per day, the business has less revenue to cover fixed cost and less room for owner draw.
Improve density by tightening the service area, grouping calls by route, and filling same-day openings fast. Watch no-shows, late cancels, and drive minutes per visit. The goal is simple: keep each operating day full of paid care, not dead time on the road.
Average Collected Revenue Per Visit
Average Collected Revenue Per Visit
A $199 collected average per visit is the cash the business actually keeps, not the sticker price. With 462 completed visits per month, that is about $91,938 in monthly collected revenue. If the same route work, fuel, and staffing stay steady, a $10 lift in collected revenue per visit adds about $4,620 a month to cash for overhead and owner pay.
The mix matters: $150 diagnostic visits pull the average down, while $250 mental-health visits lift it. Better employer accounts, cleaner cash-pay pricing, and fewer billing write-offs can improve revenue per route. What this hides is payor delay; a claim that looks strong on paper still hurts draw if cash lands late.
Track Net Collected Revenue Per Visit
Measure charges, allowed amounts, and cash collected separately, then review by visit type. Track the share of $150, $200, $220, and $250 visits, plus denial rate and patient balance write-offs. One clean number to watch: collected revenue per completed visit. If it slips, the route can look busy while owner income stalls.
Visit type mix
Collected cash per visit
Denials and write-offs
Employer or cash-pay pricing
Test pricing and scheduling together. A route with more higher-paying visits can raise cash without adding the same labor and travel load, but only if completion stays high and collections are clean. If cash collection takes longer than the visit cycle, owner pay gets squeezed even when bookings are full.
Provider Staffing And Clinical Labor Model
Clinical Staffing Load
Staffing sets both capacity and cash burn. The model scales clinical roles from 7 in Year 1 to 35 in Year 5, so each hire has to create enough completed visits to cover salary, supervision, and admin time. If labor grows faster than booked and completed visits, owner take-home drops because payroll rises before route density does.
The payroll shown in the model covers CEO, operations, medical director, and patient coordination costs only. Do not treat owner-clinician labor as free. Supervision, training, coverage gaps, and compliance work all cut into margin, so the real test is completed visits per staffed shift, not headcount alone.
Match Hires to Paid Visits
Track completed visits per provider shift, not just scheduled visits, plus no-shows, travel gaps, and after-hours coverage. Here’s the quick test: if a new clinician does not raise completed visits enough to absorb added payroll and oversight, take-home income falls even when revenue looks stronger.
Build the forecast with provider count, shift hours, supervision time, training time, and compliance work. Keep a staffing plan that shows when each hire turns into more collected revenue, because the first extra dollar should cover labor strain before it reaches owner pay.
Completed visits per shift
No-show and cancel rate
Supervision hours
Training hours
Coverage gap time
Compliance work
Payer Mix, Billing, And Collections Timing
Payer Mix and Collection Timing
Cash flow here depends on whether visits are cash pay, employer-paid, insurance-based, Medicare, Medicaid, or mixed. The model should use collected revenue, not billed charges, because denials, patient balances, billing fees, and A/R delays can shrink owner pay. One clean rule: a claim is not cash until it clears the bank.
In Year 1, average collected revenue is about $199 per visit, with pricing shown at $150 diagnostic, $200 general, $220 pediatric and geriatric, and $250 mental health visits. At 462 visits per month, that supports about $91.9k in monthly collections before costs. If collection timing slips, reported revenue can look fine while owner distributions stay tight.
Track Cash, Not Charges
Measure collected dollars per completed visit, not just scheduled or billed visits. Break it out by payer type so you can see which mix pays fast and which mix slows cash. Also track days in accounts receivable (A/R, the time between service and payment), denial rate, and patient balance collections, since those are the levers that change take-home income.
Track collections by payer type.
Watch days in A/R weekly.
Bill cleanly and fast.
Collect patient balances early.
Forecast owner pay from cash.
If billing is slow, even strong visit volume won’t fund the owner’s draw. Keep the model tied to cash collected per month, then stress-test it against denials, unpaid balances, and lagged reimbursements before you count on profit.
Fixed Overhead And Cash Reserves
Fixed Overhead Pressure
Fixed overhead is the monthly bill that must be paid before owner pay: technology licenses, office rent, insurance, marketing, professional services, fleet insurance, and data hosting. At $11,500 per month, it sets the cash floor. If Year 1 collected revenue is $91,938 per month (462 visits × $199), overhead alone uses about 12.5% of sales.
Owner take-home drops when collections are late or volume dips, because accounting profit is not cash. Vehicles, payroll timing, debt payments, taxes, and growth spending all need cash on hand. Cash profit isn’t spendable profit.
Hold the Cash Floor
Track monthly collected revenue against the $11,500 overhead line, not booked sales. Here’s the quick math: $11,500 ÷ monthly collections shows how much revenue is already committed before the owner takes anything. If billing delays rise, the reserve needs to rise too, even when the income statement looks fine.
Keep owner draws tied to cash after payroll, fleet costs, and billing lags. Review the reserve before every distribution so a slow month does not force cuts or debt. Use this simple control list:
Reconcile overhead every month
Separate booked and collected revenue
Set a cash reserve floor
Review vendor contracts quarterly
Vehicle, Route, And Service-Area Utilization
Route Density
This driver is about how many paying visits each route can finish after drive time, fuel, maintenance, and vehicle coverage. If the service area is too wide, the team spends more time driving and less time treating patients, so completed visits per day fall and owner pay shrinks. The model shows fuel and maintenance at 4% of revenue in Year 1 and 35% by Year 5.
Here’s the quick math: more deadhead miles, meaning unpaid drive time, lower revenue per route hour. Tight zip-code density protects margin because it lifts completed visits while keeping travel costs flat. Wide coverage does the opposite, even if booked demand looks strong.
Track Miles Per Visit
Measure completed visits per operating day, miles per completed visit, cancelation rate, and fuel plus maintenance as a share of revenue. Those four inputs tell you whether the route is earning enough to cover travel, vehicle wear, and the clinical team’s time. If those numbers drift, owner distributions usually drift with them.
Group visits by zip code.
Cut long, low-density routes.
Watch deadhead miles weekly.
Reprice far-out service areas.
Test denser dispatch windows before expanding the map. If the route can’t stay compact, the same visit count will produce less cash and less room for owner pay.