How Much Multiple Sclerosis Treatment Center Owners Make On $49M Revenue
You’re estimating owner take-home for an MS-focused medical center, not a guaranteed physician salary Under the provided first-year model, revenue is $489M, operating profit is about $290M before taxes, debt, reserves, and distributions, and the Medical Director Neurologist salary is $280k This excludes personal taxes, financing terms, owner lifestyle draws, and exact local payer rates
Owner income$280k+Net margin66%–85%Revenue for target pay$427kBusiness difficultyHard
Want the six drivers that move owner income?
1
Active Volume
$4.9M-$30.8M
More treated patients drive the biggest jump in owner income, with revenue rising from Year 1 to Year 5 as the clinic scales.
2
Payer Mix
$350-$3K
Reimbursement rates swing take-home fast, because lower-paid visits pull down margin across neurologic care and infusion services.
3
Infusion Economics
$2.5K-$3K
Infusion visits carry the highest ticket size, so pricing and throughput here have an outsized effect on profit.
4
Provider Output
80-140/mo
Each provider's monthly treatment load sets how much revenue the team can produce without adding wasteful headcount.
5
Staffing Overhead
$34.2K/mo
Lease, insurance, IT, and admin costs sit under every visit, so tight staffing and overhead control protect owner cash.
6
Billing Flow
2.2%-3.0%
Cleaner claims and faster prior authorization reduce leakage, improve cash timing, and keep more collected revenue in the business.
Want to test your MS clinic owner pay?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
!
Planning note: Research-based planning estimate only. Actual owner income depends on collections, margins, payroll, taxes, reserves, and distributions; this is not salary, tax advice, or owner distribution advice.
Want to check owner income in the Multiple Sclerosis Treatment Center model?
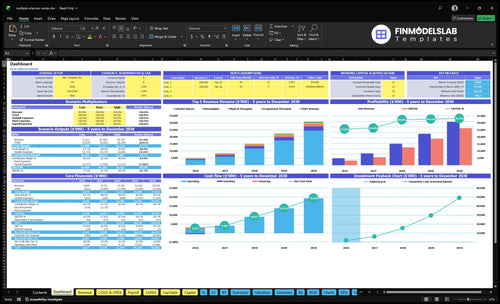
See the Multiple Sclerosis Treatment Center Financial Model Template; dashboard compares Year 1 $489M to Year 5 $3,082M, with revenue build, provider capacity, payer mix, infusion revenue, staffing, fixed costs, variable costs, cash flow, and owner take-home. Open the model.
Owner-income model highlights
Reserve-adjusted owner cash
Operating profit and margin
Scenario tabs compare outputs
How many patients does an MS treatment center need to be profitable?
No single patient count makes a Multiple Sclerosis Treatment Center profitable, because break-even swings with payer mix, staffing, service mix, and collections. In year 1, the capacity plan points to 2 neurologists at 120 monthly treatments each at 65% use, plus 3 infusion nurses at 80 monthly treatments each at 50% use. More volume only helps if authorizations clear, infusion chairs stay full, schedules stay productive, and overhead does not outrun cash collected.
What sets break-even
Payer mix changes cash collected
Staffing drives fixed cost base
Service mix shifts margin per visit
Collections can lag clinical volume
Year 1 capacity reality
2 neurologists at 65% use
120 monthly treatments per neurologist
3 infusion nurses at 50% use
Therapy and counseling stay below full use
How much can an MS treatment center owner take home?
A Multiple Sclerosis Treatment Center owner can take home the $280k Medical Director salary in the Year 1 model if they personally hold that role; extra distributions are separate and not guaranteed. The model shows $489M revenue and $290M operating profit, but What Are The Five KPIs For Multiple Sclerosis Treatment Center Business? matter because owner cash comes only after required costs, reserves, debt service, and reinvestment.
Take-home math
$489M Year 1 revenue
$290M operating profit
59.3% operating margin
$280k Medical Director salary
Cash blockers
Pay payroll first
Fund drugs and supplies
Cover rent and malpractice
Hold reserves before distributions
What is a multiple sclerosis treatment center profit margin?
A Multiple Sclerosis Treatment Center does not have one universal profit margin; in the provided Year 1 model, operating margin is about 592% before taxes, debt, reserves, and unlisted costs. Here’s the quick math in the model: $489M revenue, 125% COGS, 70% variable expenses, $4.104M fixed costs, and $629k payroll. If you want the planning context, read How To Write A Business Plan For Multiple Sclerosis Treatment Center?
Margin Drivers
Payer contracts change net revenue fast.
Drug acquisition risk can swing costs.
Denial rates cut collected cash.
Infusion utilization lifts or hurts margin.
Cost Risks
Staffing is a major fixed load.
Malpractice and rent add hard costs.
EHR and billing fees never stop.
Unlisted costs can erase paper margin.
Key Takeaways
Patient volume only pays if staffing and approvals keep up.
Payer mix can swing cash and margin fast.
Infusion revenue is biggest line, but cash risk is real.
Fixed overhead and billing frictions can crush ramp-up profits.
Owner income scenario table objective
Income scenarios
Owner income changes fast here because staffing, capacity use, and service mix scale together. The low, base, and high cases show how much earnings can move from Year 1 to Year 5.
Compare modeled income at ramp, scale, and mature service levels.
Scenario
Low CaseLow
Base CaseBase
High CaseUpside
Launch model
Owner income stays in the Year 1 ramp band while the clinic fills core capacity.
Owner income tracks the Year 3 operating case as utilization and staffing settle in.
Owner income reaches the Year 5 run rate if the center holds strong utilization and full staffing.
Typical setup
Revenue is $4.890M in Year 1 with $3.210M EBITDA, 2 neurologists, 3 infusion nurses, and a heavy fixed cost load.
Revenue reaches $15.183M in Year 3 with $12.586M EBITDA, 4 neurologists, 6 infusion nurses, and broader therapy volume.
Revenue reaches $30.818M in Year 5 with $26.287M EBITDA, 6 neurologists, 10 infusion nurses, and the widest care mix.
Cost drivers
Capacity fill
staffing ramp
claims fees
referral spend
fixed overhead
Capacity use
service mix
payroll growth
claims fees
referral spend
Full capacity
higher pricing
staff scale
claims efficiency
lower marketing ratio
Owner income rangeBefore owner reserves
$3.2MYear 1 ramp
$12.6MYear 3 scale
$26.3MYear 5 run rate
Best fit
Use this if you want a conservative view of opening-year income and overhead drag.
Use this as the middle case for budgeting, hiring, and lender talks.
Use this to test upside, staffing strain, and cash generation at scale.
!
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Multiple Sclerosis Treatment Center Core Six Income Drivers
Patient Volume And Referral Pipeline
Referral Volume
Patient volume is the main revenue engine. Every new MS referral can turn into consults, follow-ups, monitoring, infusion use, therapy visits, and counseling. In year 1, the model assumes 2 neurologists, 3 infusion nurses, 2 physical therapists, 1 occupational therapist, and 1 counselor running at 50% to 65% capacity. If referral flow is thin, those seats stay open and owner income drops.
The quick math is simple: more referrals only help if access, staffing, payer approval, and quality of care hold. If the schedule is full but prior auth stalls or wait times rise, revenue can slip and cash gets tied up. With fixed costs still running, weak referral flow leaves overhead absorbing cash instead of turning it into profit and owner pay.
Track Conversion
Track the funnel, not just referral count. Measure incoming referrals, consult booked rate, show rate, authorization success, and visits completed by service line. That tells you whether volume is real or just paper demand. If consults rise but infusions, therapy, or counseling lag, the center has an access or payer problem, not a marketing win.
Referrals by source
Booked consult rate
Prior auth approval rate
Capacity by provider
Set capacity guardrails before pushing more referrals. The 2 neurologists, 3 infusion nurses, 2 physical therapists, 1 occupational therapist, and 1 counselor should stay within usable capacity, or quality and approvals can slip. Watch days to first visit, no-shows, and denial rates so new demand converts to collections and not just more unpaid work.
Payer Mix And Reimbursement
Payer Mix And Reimbursement
For an MS treatment center, payer mix changes cash more than list price. Commercial insurance, Medicare, Medicaid, and patient responsibility all pay on different rules, so the same visit volume can turn into very different owner income when authorization delays and denials hit.
Model price, collection rate, payer share, and denial assumptions. Don’t promise exact reimbursement; local contracts and write-offs can cut margin and slow cash even when billed revenue looks strong. What matters is net collections, not the schedule rate.
Track net collections by payer
Watch clean-claims rate, days in accounts receivable, denial rate, and patient balances. Those numbers tell you whether billed work turns into cash fast enough to cover payroll, overhead, and owner draw. Here’s the quick test: same patient volume, but slower payment means less take-home income.
Stress-test the model before you hire or expand. If the payer mix shifts toward lower-paying plans, or if authorization rules get tighter, collections can fall even with full chairs and steady demand. Edit assumptions often so staffing, pricing, and owner pay stay tied to real cash, not billed charges.
Billing And Prior Authorization
Billing and Prior Auth
Billing and prior authorization turn MS care into cash the owner can pay themselves from. The plan models billing and claims processing at 30% of revenue, with a stated figure of $1,467k on the revenue base, so every denial, coding error, or auth delay hits take-home income fast.
This includes eligibility checks, payer approval, coding, claim filing, appeals, and patient balances. If treatment is delivered but the claim sits in limbo, revenue is earned but not collected, and cash flow gets tight even when demand stays strong.
Track clean claims and cash speed
Use a small set of hard numbers: clean claims, days in accounts receivable, denial rate, appeal success, and patient balances. The main inputs are visit volume, payer rules, coding quality, and how quickly prior auth comes back before infusion, imaging, or therapy starts.
Submit claims the same day.
Check codes before filing.
Push high-dollar auths first.
Work denials within days.
When auths move faster and denials stay low, cash lands sooner and owner draws are steadier. If A/R stretches or patient balances pile up, the business can look busy but still starve the owner of cash.
Infusion Therapy Economics
Infusion Admin Revenue
This is the fee for giving the infusion, not the drug itself. Using the model assumption, 3 nurses × 80 monthly treatments × $2,500 × 50% capacity × 12 equals $3.6M a year, so chair fill and nursing coverage drive owner income fast. If utilization slips, revenue falls while labor and compliance costs keep running.
What this estimate hides is cash timing. Prior authorizations, procurement, and claims delays can turn a full schedule into weak cash flow. Keep drug margin and inventory risk separate from administration revenue, or the clinic can look busy but still miss owner pay.
Track Chairs, Auths, and Collections
Measure chair utilization, approved treatments, denial rate, and days in accounts receivable. That tells you if the infusion line is turning visits into cash, or just creating work. Here’s the quick math: the same formula at 65% capacity would be $4.68M a year, before payer mix and overhead.
Protect margin by separating infusion administration from drug pass-through, then forecast both. If auths lag or nursing coverage is thin, treat that as a revenue cap, not a small delay. One missed slot a day can cut owner draw more than a modest price increase can fix.
Provider Productivity
Provider Productivity
In an MS clinic, provider productivity means keeping neurologists, infusion nurses, physical therapists, occupational therapists, and counselors scheduled near useful capacity without hurting outcomes. In Year 1, the model assumes 65% for neurologists, 50% for infusion nurses, 60% for physical therapy, 55% for occupational therapy, and 50% for counseling. Low use leaves payroll under-absorbed and cuts owner income.
The key is not just more visits. It’s access, follow-up cadence, payroll per visit, and no-show rates. If schedules get too full, care slips and returns drop; if they stay too open, fixed labor costs eat margin. One clean rule: when payroll per visit rises faster than collected revenue per visit, the owner’s draw gets squeezed.
Track Capacity, Not Just Bookings
Measure each role by utilization, show rate, and visits per labor dollar. That tells you whether extra appointments are actually turning into cash, or just adding staff cost and admin work. For this kind of clinic, the fastest win is usually fixing no-shows and follow-up gaps before adding headcount.
Use a simple review: compare scheduled visits, completed visits, and payroll for each provider type every month. If neurologists sit at 65% and nurses at 50%, look for open slots, referral flow, and authorization delays. If therapists or counseling run below target, compress visit blocks and tighten rebooking so labor supports revenue instead of dragging it down.
Track completed visits by provider.
Watch no-show and rebook rates.
Review payroll per completed visit.
Compare access time to follow-up needs.
Operating Cost Control
Operating Cost Control
The MS treatment center carries $342k/month in fixed overhead, or $4.104M/year, before any variable care costs. The named line items total $180k/month — $18k lease, $65k malpractice insurance, $32k EHR and IT, $28k utilities and maintenance, $12k supplies, and $25k compliance/legal — so the rest needs close review. Year 1 payroll of $629k adds more burn, so slow ramp-up can crowd out owner income.
Owner pay only starts to grow after monthly revenue covers that fixed base. What this estimate hides is the unlisted $162k/month inside overhead, plus startup equipment is separate, so don’t mix one-time spend with ongoing burn when you forecast cash.
Keep Burn Tight
Build the model from the costs you can control: rent, malpractice, EHR and IT, utilities, supplies, compliance/legal, and payroll. Track actual vs budget each month, plus overhead per visit and payroll as a share of revenue. A 5% overhead cut saves $17.1k/month, or $205.2k/year, which drops straight to cash available for owner pay.
Review spend every month.
Delay hires until demand sticks.
Separate capex from burn.
Watch overhead per visit.
The ramp-up risk is simple: fixed costs hit on day one, but patient volume and payer cash often lag. If collections slip or staffing comes in too early, the center funds overhead instead of owner draw.