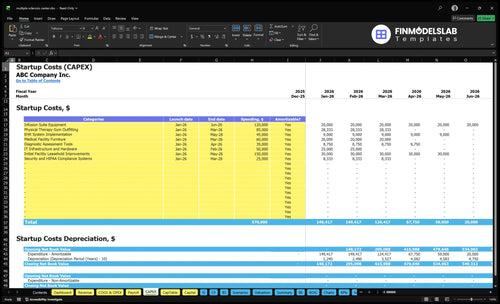
Multiple Sclerosis Treatment Center Startup Costs: $545K CAPEX
In the researched base case, startup CAPEX for a multiple sclerosis treatment center is $545,000 before pre-opening payroll, deposits, drug reserves, and working capital The largest one-time costs are $150,000 for leasehold improvements, $120,000 for infusion suite equipment, $85,000 for physical therapy gym outfitting, and $45,000 for EHR implementation The first operating year also carries $34,200 in monthly fixed overhead and $629,000 in listed annual payroll, so total funding must cover the early ramp-up period and reimbursement lag These are researched planning assumptions, not vendor quotes or guaranteed opening costs
Calculate Fuding Needs
Startup cost summary
Summarizes startup buildout costs and the non-CAPEX cash needed to open the multiple sclerosis center.
Highlighted CAPEX$465,000Base planning example
Excluded cash needs$788,000Outside CAPEX total
Funding need$1,253,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Initial facility leasehold improvements
$150,000
Buildout for treatment, infusion, and rehab space
Yes
Infusion suite equipment
$120,000
Infusion chairs, pumps, and clinical setup
Yes
Physical therapy gym outfitting
$85,000
Rehab equipment and therapy room fit-out
Yes
Medical facility furniture
$60,000
Waiting area, exam rooms, and office furniture
Yes
IT infrastructure and hardware
$50,000
Network, devices, and clinical hardware
Yes
Operating runway reserve
$788,000
Pre-opening payroll, $34.2k monthly overhead, and billing lag
No
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates the upfront capitalized startup assets needed to open a multiple sclerosis treatment center, before working capital.
!
CAPEX limits This calculator covers capitalized startup assets only. It excludes drug reserves, inventory, pre-opening payroll, payroll runway, financing fees, deposits, debt service, working capital, and other operating expenses.
Lean defers infusion and therapy buildout, Base funds the researched clinic setup, and Full adds more capacity and staff. Startup cost swings come from rooms, equipment, and payroll.
Compare a deferred build, the researched core clinic, and a larger full-service launch.
Scenario
Lean LaunchReferral model
Base LaunchInfusion-enabled
Full LaunchFull-service specialty center
Launch model
Runs as a consult-first, leased clinic that defers the infusion suite and physical therapy gym.
Launches the researched core clinic with diagnosis, infusion, therapy, and counseling on site.
Adds more infusion capacity and staff, with room for optional advanced diagnostics.
Typical setup
Keeps exam space, EHR, IT, furniture, and diagnostic tools while delaying heavier service buildout.
Includes exam rooms, infusion suite, therapy space, EHR, IT, furniture, and diagnostic tools.
Builds on the base clinic with extra nurses and therapists, while MRI and major imaging stay out because they are not priced.
Cost drivers
Leasehold improvements
EHR and IT
core care staff
diagnostic tools
Infusion suite equipment
physical therapy gym
leasehold improvements
EHR and IT
compliance systems
Expanded infusion capacity
more nurses and therapists
advanced diagnostics
higher payroll float
Planning rangeCAPEX only
$340,000Deferred build
$545,000Core build
$545,000+Capacity build
Best fit
Founders testing demand with a referral-first clinic and a lighter service mix.
Operators ready to open the standard specialty center with the full base service set.
Teams that want a broader center, higher throughput, and more cash cushion for staffing.
!
Planning note: These ranges are researched planning assumptions from the model, not vendor quotes or final bids.
How much does an MS infusion suite cost to set up?
For a Multiple Sclerosis Treatment Center, an infusion suite adds about $120,000 in equipment CAPEX, and that’s before staffing and working capital. It changes the startup budget because you now need chairs, pumps, emergency supplies, medication handling, possible refrigeration, tighter nurse workflow, prior authorization, and slower reimbursement timing risk. Here’s the quick math: with 3 infusion nurses, 80 monthly treatments per nurse, $2,500 per treatment, and 50% Year 1 capacity, infusion volume is about 120 treatments a month, or $300,000 in monthly revenue. Consult-only neurology care is a lighter startup; MRI ownership stays separate and optional because no imaging CAPEX is in the source data.
Infusion setup costs
$120,000 infusion equipment CAPEX
Chairs and infusion pumps
Emergency supplies and handling
Refrigeration if drugs need it
Year 1 operating impact
3 infusion nurses in model
120 treatments a month at 50%
About $300,000 monthly revenue
MRI is separate and optional
How do you fund a multiple sclerosis treatment center?
Fund the Multiple Sclerosis Treatment Center like a bankable launch plan, not a guess: start with $545,000 in CAPEX, $34,200 a month in fixed overhead, and $629,000 in first-year payroll. The variable-cost load is still real, with 75% consumables, 50% pharmaceutical procurement, 40% referral marketing, and 30% billing fees, so the funding stack should blend owner equity, medical practice loans, equipment financing, tenant improvement allowances, and a working capital line. Build in collections lag, payer credentialing, debt service, staffing ramp, and infusion volume ramp first; then do the financial projections.
Funding stack
Use owner equity first
Layer medical practice loans
Finance equipment separately
Negotiate tenant improvement allowances
Cash plan
Model collections lag monthly
Assume payer credentialing delay
Stage debt service carefully
Ramp staffing and infusion volume
What hidden costs of starting a multiple sclerosis treatment center are often missed?
For a Multiple Sclerosis Treatment Center, the hidden cost is working capital, not just build-out. If you’re sizing the model, start with How To Write A Business Plan For Multiple Sclerosis Treatment Center? and then add the cash drag from payer credentialing delays, 30% billing and claims fees in Year 1, and 40% patient referral and marketing costs. Drug timing matters too: you can show strong gross revenue and still run short on cash when pharma must be paid before reimbursement lands.
Big cash drains
30% billing and claims in Year 1
40% referral and marketing in Year 1
75% consumables and infusion supplies
50% pharmaceutical procurement costs
Fixed monthly load
$6,500 malpractice insurance each month
$2,500 compliance and legal retainer
$3,200 EHR and IT support
Hidden costs set funding need
Key Takeaways
Buildout is CAPEX; lease stays monthly overhead.
Infusion equipment drives the biggest clinical spend.
Technology setup and support must be budgeted separately.
Credentialing delays hit working capital, not CAPEX.
Multiple Sclerosis Treatment Center Core Five Startup Costs
Facility Buildout Startup Expense
Buildout Scope
$150,000 covers the shell-to-clinic work: exam rooms, reception, ADA access (Americans with Disabilities Act), optional infusion bays, clean storage, staff work areas, patient flow, plumbing, electrical, medical-grade finishes, and therapy space next to care rooms. This is CAPEX (capital spending), not rent. The $18,000 per month lease sits in overhead, and major imaging construction is excluded.
Budget Inputs
Use the $150,000 line as the base, then price by square footage, room count, and contractor quotes. Add the cost of code work, medical-grade finishes, and any infusion-ready plumbing or power. This spend belongs in startup CAPEX with equipment and IT, while the $18,000 monthly lease stays separate in recurring overhead.
Price by square foot.
Count rooms and bays.
Get fixed contractor quotes.
Cost Control
Keep the layout tight: reuse any code-compliant shell, group plumbing-heavy rooms together, and put therapy near exam space to avoid wasted hall area. Do not cut ADA access, clean storage, or medical-grade finishes. The common mistake is building more clinic than Year 1 staffing can use, which ties up cash with no added patient throughput.
Reuse compliant plumbing and electrical.
Keep therapy next to exams.
Skip MRI construction in base CAPEX.
Lease Timing
The $18,000 per month medical lease is recurring overhead, not buildout CAPEX. So the cash need is not just construction; it’s also rent before patient volume ramps. Keep the fitout line and the lease line separate in the model, because lease timing and any free-rent period can matter more to runway than the buildout budget itself.
Licensing Compliance And Credentialing Startup Expense
State Rules Drive Cost
Licensing for an MS treatment center is state-based, not one national fee. Budget for business formation, provider credentialing, payer enrollment, HIPAA compliance, legal help, accounting setup, and $2,500 per month for compliance and legal retainer plus $6,500 per month for malpractice insurance.
What To Price
Estimate this cost from the number of states, provider count, lab testing plans, and whether infusion drugs are purchased and billed by the center. Add CLIA review if lab testing is offered. The main inputs are filing fees, attorney time, payer contracts, and monthly retainers, not buildout CAPEX.
State medical requirements
Provider credentialing
Payer enrollment timing
CLIA if lab testing
Keep It Lean
Keep this as launch cash, not construction spend. Start with only the services you can credential fast, then add lab testing or drug billing after approvals are in place. The biggest mistake is overbuilding compliance before revenue starts. One clean one-liner: delay scope, not licenses.
Batch filings and reviews
Use one accounting setup
Limit service scope first
Cash Timing Risk
Payer credentialing delay hits working capital more than CAPEX. The clinic can be built and staffed, but cash still lags until enrollments clear and claims can go out. If infusion drugs are billed by the center, timing risk gets bigger because approvals and billing rules affect when money comes in.
Healthcare IT And EHR Startup Expense
Setup Cost
The base build is $45,000 for electronic health record (EHR) implementation plus $50,000 for IT hardware and infrastructure. That covers practice management, e-prescribing, prior authorization, infusion scheduling, billing links, patient portal, phones, network, cybersecurity, and access controls. Treat it as one-time CAPEX, not monthly overhead.
Monthly Support
Plan on $3,200 per month for EHR and IT support services. This recurring spend keeps systems updated and working across scheduling, charting, billing integrations, and secure access. Use it as operating expense, and keep it separate from the launch build so the startup budget stays clean.
Billing Setup
Claims processing fees are modeled at 30% of Year 1 revenue, so billing setup matters. If coding, prior auth, and claim flow are weak, the center loses cash to denials and rework. Build billing rules before go-live, because tech spend only works if the revenue cycle works too.
Budget Split
Use three inputs: $45,000 implementation, $50,000 hardware and infrastructure, and $3,200 monthly support. Here’s the quick math: launch CAPEX funds setup, while monthly spend funds operations. That split helps founders budget both the opening build and the ongoing technology run rate.
Staffing Readiness And Pre-Opening Payroll Startup Expense
Payroll Is Not Capex
For a Multiple Sclerosis Treatment Center, the first-year payroll listed at $629,000 is an operating cost, not CAPEX. It covers the Medical Director Neurologist at $280,000, the Clinic Operations Manager at $95,000, and the front-line care team needed before first revenue.
Base Payroll Build
Here’s the quick math: 2 care coordinators at $55,000 each, 2 front desk roles at $42,000 each, and 1 billing specialist at $60,000 bring the total to $629,000. That budget sits beside pre-opening recruiting, onboarding, training, infusion protocols, billing workflows, and scheduling readiness.
2 care coordinators = $110,000
2 front desk roles = $84,000
1 billing specialist = $60,000
Stagger The Hire Date
Keep HR and admin support after year one in the model, and hire only what is needed to open cleanly. The best savings come from timing, not quality cuts: start staff when training, payer setup, and room readiness are real, so you avoid paying months of idle labor before patient volume starts.
Hire for go-live dates, not guesses
Train on billing before launch
Use exact scheduling templates
Staffing Readiness Gate
This staffing plan supports the modeled service mix of 2 neurologists, 3 infusion nurses, 2 physical therapists, 1 occupational therapist, and 1 mental health counselor. Pre-opening payroll should fund readiness work only. Full annual wages stay in operating expenses, so the startup budget does not overstate capital needs.
Clinical And Infusion Equipment Startup Expense
Facility Buildout
The base plan uses $150,000 in leasehold improvements for exam rooms, reception, ADA access, infusion areas, clean storage, staff work areas, and therapy adjacency. This is CAPEX; the $18,000/month medical lease stays in overhead. Exclude MRI build costs, since specialty imaging is optional and not in default spend.
Clinical Equipment
Clinical equipment totals $240,000: $120,000 for infusion suite gear, $85,000 for physical therapy gym outfitting, and $35,000 for diagnostic tools. That covers exam tables, vital signs equipment, infusion chairs, pumps, emergency supplies, neurological assessment tools, therapy gear, and refrigeration where needed. Infusion gear is the biggest driver in the base plan.
IT Systems
Budget $95,000 up front for $45,000 of EHR implementation and $50,000 of IT hardware and network setup. Recurring support is $3,200/month. This covers scheduling, e-prescribing, prior auth, billing links, patient portal, phones, cybersecurity, and access controls. Claims processing fees are modeled at 30% of Year 1 revenue, so billing setup affects cash fast.
Compliance Setup
Start with state medical rules, provider credentialing, payer enrollment, HIPAA, malpractice, general liability, legal, and accounting setup; there is no single national license. The model carries $2,500/month for compliance and legal plus $6,500/month for malpractice. Credentialing delay hits working capital more than CAPEX, especially if infusion drugs are bought and billed by the center.
Pre-Opening Payroll
First-year payroll is $629,000 for the medical director neurologist ($280,000), clinic operations manager ($95,000), 2 care coordinators ($55,000 each), 2 front desk roles ($42,000 each), and 1 billing specialist ($60,000). Pre-opening spend should cover recruiting, onboarding, training, infusion protocols, and scheduling, while service capacity assumes 2 neurologists, 3 infusion nurses, 2 physical therapists, 1 occupational therapist, and 1 mental health counselor.