How Much Can a Sleep Apnea Diagnostic Center Owner Make From $1075K/Month?
A sleep apnea diagnostic center owner could plan around about $41,500 per month of pre-tax operating profit in the first year under the researched assumptions, before owner distributions, reserves, debt service, taxes, and staff wage lines not provided That comes from $107,540 in monthly revenue, less 185% in direct and variable costs, $22,800 in fixed overhead, and $23,333 in Medical Director payroll In a higher-utilization mature-year case, modeled revenue reaches $586,980 per month, but that is still a planning scenario, not a guaranteed owner paycheck The biggest swing factors are completed study volume, reimbursement, payer mix, technician coverage, physician interpretation cost, rent, equipment use, billing collections, and reserve policy
Owner income$37k-$427k/moNet margin34.5%-72.7%Revenue for target pay$107.5k/moBusiness difficultyHard
Want to test your sleep lab owner pay?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
!
Planning note: Research-based planning estimate only. Actual owner income depends on payer mix, staffing, reimbursement timing, taxes, debt, and reinvestment. This is not guaranteed salary, tax advice, or owner distribution advice.
Want the six drivers behind sleep lab income?
1
Study Volume
$107.5K/mo
Year 1 starts at about 2,282 billable units and $1.29M revenue, so more completed studies drive the biggest jump in owner take-home.
2
Payer Mix
$150-$1.4K
Service prices span $150 to $1,400, so a richer mix of higher-paid cases lifts cash per slot without adding space.
3
Room Use
65%-85%
Capacity climbs from 65% to 85%, and every point of use spreads the same lease and equipment cost over more studies.
4
Clinical Labor
$43.8K/mo
Year 1 wages run about $43.8K a month, so extra FTEs can eat EBITDA fast if volume misses plan.
5
Fixed Overhead
$22.8K/mo
Lease, insurance, and IT total $22.8K a month, so weak volume leaves less profit for the owner.
6
Owner Pay
$23.3K/mo
If the owner serves as Medical Director, the $23.3K monthly salary is direct income, but cash still has to clear the $680K Month 6 low.
Can you check owner income in the sleep lab model?
How much revenue does a sleep apnea diagnostic center need to pay the owner?
A Sleep Apnea Diagnostic Center needs about $56,600 per month in revenue just to cover the known $46,133 fixed burden, before owner pay, taxes, debt, reserves, or any unprovided wages. Here’s the quick math: $46,133 ÷ 81.5% contribution margin equals about $56,600; if you want to pay the owner, add that pay to fixed costs first, then divide by 81.5%.
Fixed cost base
$22,800 fixed overhead
$23,333 Medical Director payroll
$46,133 total monthly burden
Break-even: about $56,600 revenue
What changes the target
Use: (fixed costs + owner pay) ÷ 81.5%
Payer mix can shift revenue fast
Utilization can shift revenue fast
22 million Americans have sleep apnea; 80% go undiagnosed
Does a sleep apnea diagnostic center make more money if the owner operates it?
Yes—if the owner legally fills a needed clinical, admin, or management role, a Sleep Apnea Diagnostic Center can keep more cash in-house. But that does not make income guaranteed: monthly revenue can scale from $107,540 to $586,980 as staffing grows from 4 sleep technologists to 12 and physicians from 1 to 3, and that also raises payer, compliance, scheduling, and fixed-cost risk.
Cash flow boost
Owner work can replace a hire.
Cash flow improves if labor stays in-house.
Revenue still depends on utilization.
More rooms do not guarantee profit.
Scale risk
Staffing rises from 4 to 12.
Physicians rise from 1 to 3.
Monthly revenue can reach $586,980.
Compliance and fixed costs rise too.
What affects sleep apnea diagnostic center profit margins?
Margins in a Sleep Apnea Diagnostic Center are driven by reimbursement per completed study, completed volume, no-shows, payer mix, staff coverage, billing, and rent; the business-plan math starts with completed studies, not booked slots, in How To Write A Business Plan For Sleep Apnea Diagnostic Center?. Year 1 direct COGS is 95%, variable referral and billing costs are 90%, and fixed overhead is $22,800 per month. So every denied claim or unused room lowers owner take-home because fixed costs still run.
Revenue levers
Reimbursement per study sets margin.
Completed volume spreads fixed cost.
No-shows leave rooms empty.
Payer mix changes collections.
Cost pressure points
Year 1 direct COGS is 95%.
Referral and billing costs are 90%.
Fixed overhead is $22,800/month.
Mature-year costs are 140% combined.
Key Takeaways
Completed billable studies drive revenue, not booked slots.
Collections depend on payer mix, denials, and timing.
Understaffing hurts margins and can weaken collections.
Owner take-home comes after reserves, debt, taxes, reinvestment.
Compare lean, base, and high-utilization owner income cases
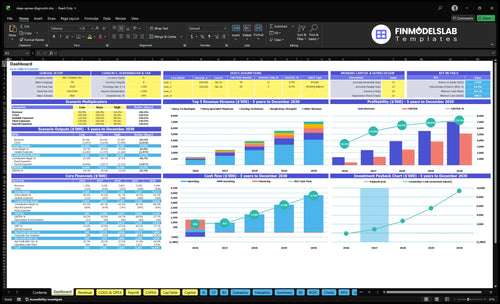
Owner income scenarios
Income here changes fast with patient volume, staffing, and fixed overhead. The lean, base, and high cases show how the same center moves from opening-month profit to mature-year cash flow.
Monthly owner income view across opening, base, and mature operation.
Scenario
Low CaseLow Case
Base CaseBase Case
High CaseHigh Case
Launch model
This is the lean opening case with Year 1 assumptions and the lowest modeled owner income.
This is the core case using Year 3 assumptions and the middle profit path.
This is the mature-year upside case with the strongest modeled owner income.
Typical setup
Revenue is about $107,540 a month on 2,282 billable units, with an 81.5% contribution margin and $46,133 in known fixed costs plus Medical Director burden.
Revenue rises to about $324,270 a month on 6,676 units, with an 83.9% contribution margin and about $225,898 in monthly operating profit on the provided cost base.
A mature year reaches about $586,980 a month on 11,828 units, with an 86.0% contribution margin and about $458,670 in monthly operating profit.
Cost drivers
Year 1 volume
81.5% contribution margin
$46,133 fixed costs
Medical Director burden
unprovided wage lines
Year 3 volume
83.9% contribution margin
6,676 billable units
provided cost base
staffing scale-up
Mature-year volume
86.0% contribution margin
11,828 billable units
larger staffing base
lower unit costs
Owner income rangeBefore owner reserves
$41k - $42kLow Case
$225k - $226kBase Case
$458k - $459kHigh Case
Best fit
Use this to stress-test the opening month before volume, staffing, and referral flow settle.
Use this for lender work, budget planning, and the center's normal operating target.
Use this to test upside when referral flow stays strong and capacity stays full.
!
Planning note: Scenario figures are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distribution amounts.
Sleep Apnea Diagnostic Center Core Six Income Drivers
Completed Sleep Study Volume
Completed Billable Sleep Studies
Income starts with completed billable studies, not inquiries or booked slots. In Year 1, 4 Sleep Technologists at 22 treatments and 65% capacity produce 572 completed units a month from that line, while total modeled billable activity reaches 2,282 units across all service lines. If no-shows, uncovered nights, or weak physician referrals cut completions, revenue falls before margin math even starts.
Track Completions, Not Bookings
Measure scheduled studies, completed studies, no-show rate, and referral volume every week. Here’s the quick math: if completed volume slips below the modeled 572 monthly technologist units, owner pay gets squeezed because fixed labor and facility costs stay put. Mature-year capacity rises to 2,448 units a month, so growth depends on keeping rooms filled, nights covered, and referrals moving.
Fixed Overhead and Administrative Costs
Fixed Overhead and Admin Costs
When fixed overhead runs $22,800 per month, owner take-home gets squeezed before any distribution decision. That base includes $12,000 lease, $3,000 professional liability insurance, $2,500 maintenance, $1,800 utilities and internet, $1,500 janitorial and linen, $1,200 EHR and data security, and $800 accreditation and compliance. Every month, completed sleep study gross profit has to cover this stack first.
If you add referral marketing at 50% of revenue in Year 1 and billing at 40%, cash gets tight fast. Keep overhead tied to sleep lab work, not generic office spend. If a line item does not help fill rooms, document studies, or collect claims, it is cutting into the owner’s draw.
Keep Overhead Tied to Lab Output
Track fixed overhead as a share of collected revenue, not booked volume. Here’s the quick math: with $22,800 in monthly fixed costs, every extra non-core dollar lowers cash available for payroll, reserves, and owner pay. Review lease size, insurance, EHR fees, janitorial scope, and compliance spend against the number of rooms used and studies completed.
Use a simple rule: if a cost does not help fill, run, document, bill, or defend a sleep study, cut it. The biggest leak is admin creep. Referral marketing at 50% of revenue in Year 1 and billing at 40% can wipe out margin quickly if overhead is not kept tight.
Reimbursement, Payer Mix, and Collections
Reimbursement and Collections
Income here comes from paid claims per completed sleep service, not the billed charge alone. The model uses $1,200 for a Sleep Technologist service in Year 1, plus $350 for a Sleep Specialist Physician, $150 for a Scoring Technician, $250 for a Respiratory Therapist, and $200 for a Nurse Practitioner.
What this estimate hides: local payer contracts, denials, and slow cash collection can cut owner income fast. Billing and claims processing cost is set at 40% of revenue in Year 1, so a weak payer mix or poor documentation can push cash flow down even when volume is steady. Reimbursement is never guaranteed.
Track Net Collection, Not Just Charges
Measure net collections by payer and service line, then compare that to denial rate and days to cash. If one payer pays slower or denies more, it lowers take-home income because staff and billing costs still get paid first.
Use clean notes, correct coding, and pre-service eligibility checks to protect collections. Keep a simple rule: if documentation does not support the claim, the expected revenue is not real yet. That is the difference between booked revenue and money the owner can draw.
Clinical Labor and Interpretation Costs
Clinical Labor and Interpretation Costs
This driver is the cost of getting each sleep study done, scored, interpreted, and supervised safely. It includes Sleep Technologists, Sleep Specialist Physicians, Scoring Technicians, Respiratory Therapists, Nurse Practitioners, and Medical Director oversight. The staffing model rises from 4 to 12 Sleep Technologists, 1 to 3 physicians, 1 to 3 scoring techs, 1 to 4 respiratory therapists, and 1 to 2 nurse practitioners, so payroll and margin move with coverage.
The Medical Director payroll alone is $280,000 per year, or about $23,333 per month. That means this line can protect revenue quality or drain owner pay fast. If staffing is too thin, documentation slips, collections slow, and compliance risk rises. If staffing is too heavy for actual completed studies, gross margin falls before the owner can pay themselves.
Staff to billed studies, not open shifts
Track completed billable studies, interpretation turnaround, and coverage gaps together. Here’s the quick math: labor only helps if it lifts the number of studies that are fully documented, signed, and collectible. Set staffing by referral volume and night coverage, then match scoring and physician hours to the read backlog.
Watch documentation quality like cash, because it drives denials and payment timing. Add technologists for nights, scoring techs for reads, physicians for interpretation, and respiratory therapy only when that bottleneck is real. Safe staffing protects collections; unsafe understaffing can look cheaper but usually costs more in denied claims and delayed income.
Room and Equipment Utilization
Room and Equipment Utilization
Room and equipment utilization is how many nights your rooms, beds, and monitoring devices are actually used. In this model, fixed facility and equipment costs are $17,500 per month from the lease, maintenance, utilities, internet, and EHR/security. When more nights are filled, those costs get spread over more billable studies, so owner profit and cash flow improve. Idle rooms do the opposite: the same cost base eats more of each collected dollar.
Year 1 capacity is modeled at 65%, rising to 85% in a mature year. That is about 31% more used capacity at the same fixed-cost base (85 ÷ 65). But adding rooms only helps if payer demand, staff coverage, scoring, and physician interpretation can keep pace. Otherwise, you add empty space, not income.
Track nights, not just rooms
Track occupied beds per night, canceled studies, and nights lost to staff gaps. Use a simple monthly formula: utilization = used nights ÷ available nights. If the schedule looks full but reports are late, cash still trails because billing waits on scoring and physician sign-off. The real goal is smooth throughput, not just a packed calendar.
Watch no-shows and open nights.
Match rooms to staff coverage.
Clear scoring and reads fast.
Before adding rooms, test whether current capacity is the limit. If utilization stays below 65%, more rooms usually raise fixed cost pressure faster than revenue. If utilization is near 85% and referrals are stable, new rooms can lift take-home income by raising billable volume without much extra overhead.
Owner Role, Reserves, and Reinvestment
Owner Take-Home After Reserves
Owner pay is not the same as operating profit. Under the provided assumptions, Year 1 operating profit is about $41,512 per month before debt service, taxes, reserves, and reinvestment. That means take-home depends on how much cash you keep back for claim delays, payer denials, and equipment replacement, not just how many studies you bill.
If the owner draws all cash, short-term income looks higher, but working capital risk rises fast. If the owner hires a manager, payroll lowers distributions, though it may free the owner from daily operations. Keep owner salary for work performed separate from profit draws, because that split changes both taxes and true cash left for the business.
Track Draws, Reserves, and Reinvestment
Measure operating profit, monthly reserves, debt service, tax set-asides, and owner salary separately. A simple rule: cash left after those items is the real owner take-home. If reserve funding is skipped, one slow payer or equipment failure can wipe out a month of distributions.
Build a reserve policy that covers claim delays, equipment replacement, and payer denials. Then decide what gets reinvested before any owner draw. Here’s the quick math: higher reserves mean lower current pay, but they protect future pay by keeping the sleep lab open, staffed, and collectable.