Sleep Apnea Diagnostic Center Startup Costs: $680K Cash Plan
To start a sleep apnea diagnostic center, plan around $452,000 in core CAPEX plus startup expenses, deposits, staffing readiness, and working capital The researched model shows a $680,000 minimum cash need in Month 6, with first-year revenue of $129 million and Month 1 breakeven under the stated assumptions The final sleep study center startup cost depends on room count, in-lab versus home testing mix, location, accreditation path, payer enrollment timing, and how quickly physician referrals convert Treat these numbers as business-planning assumptions, not quotes or guaranteed reimbursement outcomes
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates capitalized startup assets only for a sleep apnea diagnostic center, not working capital or other startup funding needs.
!
Excluded from CAPEX This calculator covers capitalized startup assets only. It excludes payroll runway, rent deposits, debt service, working capital, inventory, referral marketing, billing setup, insurance premiums, credentialing delays, and owner draws.
Calculate Fuding Needs
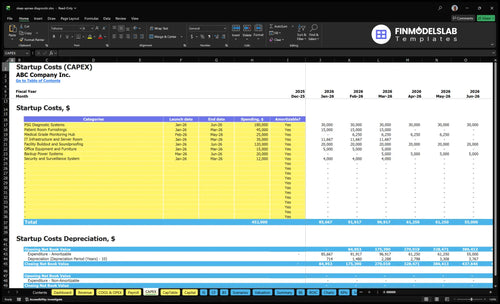
Startup cost summary
This table covers the main startup assets and the non-CAPEX operating reserve needed before Month 6.
Startup cost swings with room count, PSG system depth, and how much home testing you keep in the mix. Lean cuts buildout and cash burn; Full adds rooms, staff, and payer prep.
Lean, Base, and Full launch setups for a sleep apnea diagnostic center.
Scenario
Lean LaunchLow-capex pilot
Base LaunchBalanced model
Full LaunchScale build
Launch model
Start with home sleep apnea testing and limited overnight rooms, then add capacity as referrals prove out.
Use a mixed home and in-lab model with enough rooms and staff to match the researched forecast.
Open a multi-room center with more PSG systems, broader staffing, and stronger payer readiness.
Typical setup
Use a small buildout, lighter equipment depth, and tighter working capital.
Keep the modeled PSG systems, standard buildout, clinical staff, and billing support.
Add room count, equipment depth, accreditation prep, and more operating cushion.
Cost drivers
sleep testing equipment
small room buildout
lean clinical staffing
referral outreach
working capital
PSG systems
facility buildout
clinical payroll
billing services
compliance fees
extra rooms
PSG systems
staffing depth
accreditation prep
payer setup
Planning rangeCAPEX only
$250,000 - $400,000Tight funding band
$452,000 - $680,000Model-based range
$750,000 - $1,100,000Higher build risk
Best fit
Best for a referral-testing pilot that wants to prove demand before adding more rooms.
Best for a mixed diagnostic center that expects steady referral flow and wants the modeled Month 1 breakeven path.
Best for a multi-room accredited sleep center built for larger referral volume and broader payer access.
!
Planning note: These ranges are researched planning assumptions from the model, not exact vendor quotes or final bids.
How do I build a sleep apnea diagnostic center funding plan?
For a Sleep Apnea Diagnostic Center, start the funding plan with the $452,000 CAPEX schedule, then add pre-opening payroll, insurance, compliance, rent deposits, billing setup, and working capital so lenders can see the full cash need before launch. Map the spend across Month 1 to Month 6, and include depreciation on equipment plus amortization where it applies. Then stress test the plan against Year 1 revenue of $129 million, Year 2 revenue of $2438 million, IRR of 1306%, ROE of 1389%, and a 15-month payback, but also test slower payer enrollment and lower utilization.
Funding build
$452,000 CAPEX baseline
Pre-opening payroll next
Add rent deposits and insurance
Include billing setup and working capital
Model checks
Stage spend across Month 1 to Month 6
Include equipment depreciation
Track amortization where needed
Test slower payer enrollment and utilization
What are the biggest cost drivers for a sleep lab startup?
For a Sleep Apnea Diagnostic Center, the biggest cost drivers are room count, PSG diagnostic systems, and facility buildout. The largest CAPEX line is $180,000 for PSG systems, followed by $120,000 for buildout and soundproofing, plus $45,000 for patient room furnishings, $35,000 for IT, and $25,000 for the monitoring hub. With 22 million Americans affected and 80% of moderate to severe cases still undiagnosed, cost rises fast when you add private bathrooms, low-voltage wiring, sound control, backup power, and patient comfort.
Largest cost lines
$180,000 PSG systems
$120,000 buildout
$45,000 furnishings
$35,000 IT setup
Room-level cost adds
Private bathrooms raise cost
Soundproofing adds spend
Backup power adds spend
Staffing depth adds fixed cost
How much money do I need to open a sleep study center?
You should budget at least $680,000 to open a Sleep Apnea Diagnostic Center, not just the $452,000 CAPEX line; the gap covers pre-opening costs and working capital through the Month 6 cash low point. For setup steps, see How Do I Launch A Sleep Apnea Diagnostic Center Business?, but don’t price this like an equipment purchase because payroll, rent, insurance, compliance, payer enrollment, referral ramp, and reimbursement lag drive the real cash need.
Equipment CAPEX starts at $180,000 for PSG systems.
Buildout and furnishings add $165,000 before opening.
Software costs $35,000 upfront plus $1,200 monthly.
Staffing and enrollment create early cash gaps.
Sleep Apnea Diagnostic Center Core Five Startup Costs
Sleep Study Equipment Startup Expense
PSG Core Spend
$180,000 for PSG diagnostic systems is the main launch CAPEX for Month 1 to Month 6. That line should also cover sensors, amplifiers, home sleep apnea testing kits, CPAP titration equipment, calibration tools, monitoring devices, and backup devices. The real driver is how many beds and simultaneous studies you plan to run.
Capacity Drivers
Estimate spend by bed count, simultaneous studies, and scoring workflow, then check backup capacity and physician or accreditation needs. Add $25,000 for a medical-grade monitoring hub and $20,000 for backup power systems when the lab needs always-on oversight. That keeps equipment planning tied to uptime, not just device price.
Buy in Phases
The safest way to control this cost is staged buying: start with the approved PSG core, then add the monitoring hub and backup power only when the licensed workflow needs them. Don’t buy for theoretical peak load. Overbuying usually shows up as idle rooms, duplicate monitors, and weak cash use.
Compliance Gate
Do not treat the purchase as clinically adequate until physician supervision, state rules, and accreditation review are done. Equipment can look complete on paper and still miss the mark if scoring workflow, backup plan, or monitoring setup does not fit the approved operating model.
Sleep Lab Buildout Startup Expense
Buildout Scope
$120,000 for facility buildout and soundproofing plus $45,000 for patient room furnishings is the main planning base. This covers private sleep rooms, bathrooms, a monitoring or control area, electrical work, low-voltage cabling, HVAC comfort, signage, and Americans with Disabilities Act (ADA) access features. Add $12,000 for security and surveillance where readiness requires it.
Cost Inputs
Estimate this by room count, bathroom layout, leased-space condition, local construction pricing, and landlord allowances. Here’s the quick math: base buildout $120,000 + furnishings $45,000 + security $12,000 = $177,000 before site-specific changes. One extra room or a rough shell can push the total up fast.
Count rooms and bathrooms.
Get contractor quotes.
Check landlord credits.
Keep It Tight
Cut cost by matching the scope to the leased shell, not by trimming comfort or access. Keep the room count tight, reuse usable finishes, and price sound control before signing. The common miss is underbudgeting HVAC, cabling, and bathroom work, then paying more later. Small design choices can save real cash.
Value-engineer finishes early.
Lock landlord work scope.
Protect ADA access.
CAPEX Only
This is CAPEX, not working capital, because it builds long-life facility assets. Put it on the balance sheet and match it to lease term and expected use, not monthly cash needs. If the space needs heavy soundproofing or new bathrooms, budget extra time and cash before opening.
Compliance and Payer Enrollment Startup Expense
Setup Cost
One-time setup covers legal formation, policies and procedures, medical director arrangements, payer enrollment, compliance documentation, professional fees, and billing readiness. The cost depends on state rules, payer contract terms, physician supervision model, and services offered. Treat this as pre-opening admin and legal work, not equipment, and get quotes for each payer packet and attorney review.
Monthly Overhead
The ongoing compliance load is about $3,800 per month: $800 for accreditation and compliance support plus $3,000 for professional liability insurance. That keeps policies current, supports documentation, and helps with payer follow-up. Keep the file set clean, because each state and payer can ask for different proof before claims can move.
Credentialing Lag
Payer credentialing delays can create a cash gap even when demand is strong. Working capital should cover the months between first study and first paid claim, so use monthly compliance overhead × delay months as the base and add staffing and lab cash on top. If billing is not ready on day one, the delay gets expensive fast.
Cash Buffer
Build the buffer around the slowest payer, not the fastest one. If enrollment takes longer than planned, keep enough cash to cover compliance, insurance, and billing support until claims start paying, because open slots do not fix a reimbursement delay.
Sleep Lab Software Startup Expense
Software stack
Sleep lab software should bundle scoring software, electronic health record (EHR), practice management, scheduling, billing, secure data storage, cybersecurity, telehealth tools, and IT hardware. Budget $35,000 for IT infrastructure and a server room as capital spending (CAPEX), plus $1,200 a month for the EHR and data security license. Add diagnostic software processing fees equal to 30% of Year 1 revenue, stepping down to 20% by Year 5.
Budget inputs
Price it from the number of users, study volume, and vendor quotes. Use separate lines for hardware purchase, software subscriptions, and processing fees so you can see cash timing. Ask for pricing per seat, per study, and per month of coverage. This cost sits in launch budget because hardware is upfront, while the license and processing fees hit monthly cash flow.
Quote per-user and per-study rates.
Split hardware from subscriptions.
Track months of license coverage.
Keep it lean
Keep the stack lean by buying only the seats and modules you need, then review usage after launch. Don’t mix equipment buys with subscriptions, and don’t skip vendor due diligence. The biggest waste is paying for unused licenses or weak integration. If billing, scheduling, and scoring share data cleanly, you avoid duplicate entry and rework.
Kill unused user seats fast.
Test integrations before signing.
Renew only what gets used.
HIPAA controls
Health Insurance Portability and Accountability Act (HIPAA) setup is part of software spend, not an add-on. Build access controls, backup procedures, audit logs, and vendor due diligence before go-live. The point is to protect patient data and keep the center audit-ready, especially when telehealth tools and cloud storage share the same workflow.
Sleep Lab Staffing Startup Expense
Payroll Floor
Treat staffing readiness as pre-opening working capital, not CAPEX. The base payroll model is $525,000 a year, or about $43,750 a month, before payroll taxes, benefits, and temp cover. That is the cash floor for opening with the planned clinical team and staying ready for overnight studies.
Year 1 Team
Year 1 staffing assumes 4 sleep technologists, 1 sleep specialist physician, 1 scoring technician, 1 respiratory therapist, and 1 nurse practitioner. The wage model also carries a $280,000 medical director, $95,000 clinical manager, $45,000 patient coordinator, $65,000 physician liaison, and $40,000 administrative assistant, or $525,000 annual base payroll.
Cost Control
Keep the team lean until referrals and overnight volume are real. The main cost drivers are operating hours, overnight coverage, study volume, onboarding, recruiting, training, and billing support. Year 1 utilization can run from 500% to 700% depending on role, so match staffing to actual nightly demand, not hope.
Cash Buffer
Working capital should cover payroll while payer enrollment and claims catch up. Put the first hires, training time, and billing setup in this bucket, then keep it separate from equipment and buildout CAPEX. If enrollment slips, payroll still hits on schedule, so this reserve protects opening month cash.