How Much Can a Total Artificial Heart Program Owner Make at $129M?
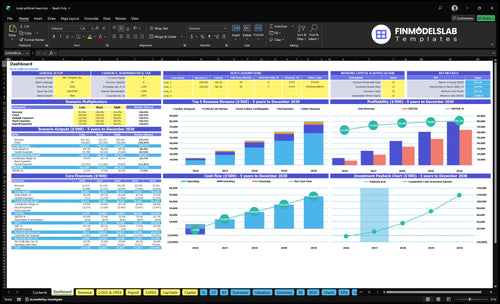
You’re modeling owner take-home from a hospital-based Total Artificial Heart Program, not a guaranteed salary The provided five-year model shows $129M in first-year revenue rising to $793M by Year 5, before full payroll, debt service, taxes, reinvestment, and compliance reserves This page covers revenue, direct costs, staffing capacity, fixed facility cost, margins, and owner distributions as planning assumptions only
Owner income$8.3M–$64.3MNet margin64%–81%Revenue for target pay$12.9MBusiness difficultyHard
Which drivers move owner income most?
1
Implant Volume
192-1,152
More implants spread fixed costs faster and lift owner take-home the most.
2
Payer Mix
$450K-$506K
Higher reimbursement per case raises revenue before the program hits labor and facility costs.
3
Direct Costs
20.5%-15.2%
Lower device, consumable, commission, and logistics load keeps more gross margin per implant.
4
Staffing Model
23-64 roles
Clinical headcount growth must stay close to volume or wages will eat EBITDA.
5
Referral Network
4.0%-2.0%
Stronger referral flow reduces paid partner commissions and keeps the pipeline full.
6
ICU Outcomes
$2.71M
Shorter ICU stays protect capacity and stop annual fixed overhead from diluting margin.
Want to test your owner take-home?
Owner income calculator
Estimate owner take-home and the target-pay gap from monthly revenue, margin, labor, overhead, reserves, and target pay. Use the Year 1, Year 3, and Year 5 planning cases as the default range.
!
Planning note: This is a researched planning estimate, not guaranteed salary, tax advice, or owner distribution advice.
Need the full pro forma view for the Total Artificial Heart Program?
Yes—this Total Artificial Heart Program Financial Model Template adds the full dashboard, reimbursement, volume, staffing, device and ICU costs, lease, reserves, debt, and owner-income scenarios. It’s the next step after income logic. Open the model.
Full pro forma model highlights
Revenue charts: $129M to $793M
Surgeons: 2 to 6
Cardiologists: 3 to 8
Nurses: 12 to 36
How many total artificial heart implants are needed to be profitable?
The Total Artificial Heart Program needs reimbursement to exceed direct case costs plus fixed readiness costs; the provided model uses 192 implants in Year 1, 672 in Year 3, and 1,152 in Year 5 as the operating scale, not a confirmed break-even count. For the plan math behind this, see How Do I Write A Business Plan To Launch Total Artificial Heart Program?, because a $144M annual facility lease makes low volume owner income highly volatile.
Volume targets
Year 1 model: 192 implants
Year 3 model: 672 implants
Year 5 model: 1,152 implants
Lease load: $144M per year
Profit gates
Beat direct case costs
Control cost load from 205% to 152%
Secure payer authorization
Fund payroll, debt, compliance, capacity
Is a Total Artificial Heart Program profitable for an owner?
The Total Artificial Heart Program can be financially feasible inside a larger medical center, but it is much harder as a standalone site. Here’s the quick math: model revenue grows from $129M to $793M over 5 years, and known operating profit before unprovided payroll and reserves rises from about $88M to $658M. That only works if referral depth, transplant alignment, 24/7 clinical coverage, payer contracts, outcomes, and capital reserves all support volume.
Why it can work
$129M to $793M revenue path
$88M to $658M operating profit
Best fit: larger medical center
Needs steady referral and transplant flow
Why standalone is tougher
Readiness costs stay high
Reimbursement can move around
Regulation raises setup burden
Capital barriers limit early scale
Which Total Artificial Heart Program costs reduce take-home most?
If you’re asking which costs cut take-home most in a How Much To Start A Total Artificial Heart Program? setup, the biggest drag is device and surgical kits: they run at 120% of revenue in Year 1 and still 100% in Year 5. That’s before specialized consumables, referral partner costs, and transport; the known direct cost load is 205% in Year 1 and 152% in Year 5, so the model is underwater unless other economics are much better.
Main cost drains
Device and surgical kits: 120% to 100%
Specialized consumables: 30% to 22%
Referral partner costs: 40% to 20%
Transport and logistics: 15% to 10%
What’s still missing
Payroll is not included
ICU days are not included
Blood products and imaging are missing
Infection care, readmissions, debt service, reserves
Key Takeaways
Volume spreads fixed lease costs and improves team use.
Reimbursement and payer mix drive net revenue and cash.
Device, logistics, and ICU days can crush margin.
Referrals and authorization quality determine usable case flow.
Compare low, base, and high owner-income scenarios
Scenario table
Owner income moves with implant volume, staffing, and reimbursement. Low, base, and high cases show how fixed clinical costs and payer mix shape take-home profit.
Compare low, base, and high income cases for the program.
Scenario
Low CaseLow volume risk
Base CaseStaffing intensity
High CaseReimbursement sensitivity
Launch model
This is the lower earnings path, with Year 1 volume and a tighter spread between revenue and costs.
This is the modeled middle path, with Year 3 scale and steady throughput.
This is the stronger earnings path, with Year 5 scale and the widest operating spread.
Typical setup
Year 1 volume is 192 implants with about $129M revenue, a 795% contribution margin, and about $88M known profit before payroll, debt, taxes, and reserves.
Year 3 volume is 672 implants with about $442M revenue, an 821% contribution margin, and about $349M known profit before payroll, debt, taxes, and reserves.
Year 5 volume reaches 1,152 implants with about $793M revenue, an 848% contribution margin, and about $658M known profit before payroll, debt, taxes, and reserves.
Cost drivers
Low implant volume
fixed staffing load
referral commissions
device and surgical kit costs
reimbursement pressure
Steady implant volume
larger clinical team
referral commissions
facility and compliance overhead
reimbursement mix
High implant volume
bigger nursing bench
more surgeon coverage
higher compliance load
payer mix pressure
Owner income rangeBefore owner reserves
$88MVolume risk
$349MCore plan
$658MUpside case
Best fit
Use this to stress-test cash flow if volumes stay near launch levels and payer collection is slow.
Use this as the working plan for budgets, hiring, and lender talks.
Use this to test upside if capacity, staffing, and reimbursement all hold.
!
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Total Artificial Heart Program Core Six Income Drivers
Annual Implant Volume
Annual Implant Volume
Annual implant volume drives fixed-cost absorption—that means spreading the $144M facility lease and ready staffing over more cases. Going from 192 implants in Year 1 to 1,152 in Year 5 can improve margin and owner pay, but only if those implants are authorized, scheduled, and completed without wasting ICU time.
Volume alone does not create profit. Revenue grows only if cardiac surgeon capacity rises from 400% to 800%, because more qualified cases must pass through the same operating room, ICU, and follow-up team. If authorizations fail, ICU days stretch, or readmissions rise, the extra volume can raise costs faster than cash comes in.
Track Qualified Cases
Measure qualified authorized implants, not just referrals. Track monthly implants, authorization rate, ICU length of stay, readmissions, and fixed cost per case. That tells you whether volume is actually lowering overhead per implant and improving cash the owner can draw.
Monthly implants: 192 to 1,152 path
Authorization rate: no approval, no revenue
ICU days: drives nursing cost
Readmissions: can erase margin
Build a base, upside, and stress forecast. If case flow is strong but capacity stays near 400%, the program stays underused; if capacity climbs toward 800% and cases stay clean, fixed costs get spread better and take-home income improves.
Specialist Staffing Model
Specialist Staffing Load
This driver is the cost of keeping a 24/7 total artificial heart team ready before cases arrive. Headcount rises from 2 to 6 cardiac surgeons, 3 to 8 heart failure cardiologists, 4 to 8 perfusionists, 12 to 36 critical care nurses, and 2 to 6 device technicians. Low volume hurts take-home because salaries, benefits, call coverage, billing staff, and device coordination are partly fixed even when case count is thin.
The key pressure point is fixed readiness versus variable case labor. If authorized cases do not fill the schedule, payroll sits ahead of revenue and owner draw gets squeezed. What this estimate hides is the dollar pay rate, so the real test is whether staffed capacity stays high enough to spread coverage costs across enough implants and follow-up care.
Track Readiness, Not Just Headcount
Track FTEs, paid call hours, case volume, and staffed-to-case ratio every month. Build the model with separate lines for salaries, benefits, call coverage, billing, and device coordination, because those costs hit even before the next implant is booked. That is the quick math: more ready staff helps access, but only if volume is there to absorb them.
Match staffing to authorized cases.
Monitor idle coverage hours.
Forecast pay against implant volume.
Separate fixed and case labor.
Referral Network Strength
Referral Network Strength
Referral network strength is how well the program turns cardiology, transplant, emergency department, insurer, and regional hospital relationships into authorized, clinically appropriate cases. It drives implant volume, follow-up visits, and post-implant management, so weak referrals leave readiness costs underused and cut owner profit even when clinical skill is strong.
Track referrals received, authorization rate, conversion to implant, payer mix, and days from referral to approval. Here’s the quick math: more covered cases raise revenue and cash flow, but denials or slow approvals keep surgeons, ICU, and coordination capacity idle, which lowers the owner’s take-home pay.
Measure and Tighten Referral Flow
Build the model by source, not as one lump. Split referrals from cardiologists, transplant centers, emergency departments, insurers, and regional hospitals, then tag each case by payer and approval status. The goal is not more leads; it’s more billable, covered cases that can move to implant and long-term care.
Count referrals by source.
Track approval days.
Watch denial and appeal rates.
Measure implant conversion.
Link follow-ups to each case.
Device And Direct Clinical Costs
Direct Device Cost Load
This is the main margin lever per total artificial heart case. In the model, device and surgical kits run 120% of revenue in Year 1 and 100% in Year 5, consumables add 30% to 22%, and referral plus logistics add 55% to 30%; that cost mix decides how much cash is left for fixed overhead and owner pay.
Track cost per case, not just volume. If a case brings in the same fee but kit, consumable, or transport spend rises, contribution margin shrinks fast; the model shows a lift from 795% to 848% before fixed costs when direct load falls, so every point saved here drops straight to profit and draw.
Control Cost Per Case
Build each case around one file: episode revenue, device kit cost, consumables, and referral/logistics. Then compare actual spend to the modeled percentages every month. One line tells you the truth: direct cost per case ÷ case revenue. If that ratio drifts up, owner cash gets squeezed before fixed costs are even paid.
Measure cost by case ID.
Separate kits from consumables.
Audit logistics and referral spend.
Flag any case over target.
Reimbursement And Payer Mix
Reimbursement And Payer Mix
Reimbursement is the net money you keep per total artificial heart case after payer rules, denials, and collections. Even at the same implant volume, episode pricing moves from $450,000 in Year 1 to $506,479 in Year 5, a lift of $56,479 or about 12.6%. That change hits revenue, gross margin, and owner pay fast.
Payer mix changes cash timing, not just price. Medicare, commercial insurance, and negotiated rates can shift authorization rate, denial rate, and collection lag, so the same case load can produce very different cash reserves. Cardiology, perfusion, nursing, and device technician management revenue also adds income, but only if it is actually authorized and collected.
Track payer mix, not just case count
Build the model around Medicare, commercial insurance, negotiated rates, authorization rate, denial rate, and collection lag. Here’s the quick math: same volume, different mix, different cash. If one payer delays payment or denies more often, the program needs more working capital even when revenue looks stable on paper.
Track net revenue by payer
Separate managed-care and episode income
Measure days to cash
Review denied claims weekly
Never treat modeled reimbursement as guaranteed. If authorization slips or denials rise, owner draw gets squeezed before volume shows the problem. The cleanest control is to forecast cash by payer, then stress test the model for slower collections and lower approved case rates.
ICU Length Of Stay And Outcomes
ICU Stay Per Case
ICU length of stay is a margin driver because every extra day adds nursing, supplies, imaging, blood products, and complication costs before the case can clear to the next phase of care. For total artificial heart patients, post-implant management revenue helps, but longer ICU time can still wipe out contribution margin if labor and consumables rise faster than collections.
Here’s the quick math: the program’s critical care nursing load rises from 12 nurses at 600% capacity to 36 nurses at 850% capacity. That means bed-days are expensive, so the owner’s take-home income depends on keeping ICU days tight enough to protect margin and free capacity for more billable cases.
Track ICU Days And Cost Per Stay
Measure average ICU days per implant, nursing hours per patient, and direct ICU cost per case. Also track imaging, blood products, readmissions, and transplant timing, since each one can push cash out before payment catches up. If ICU days drift up, the program may need more nurses or higher reserve cash, which cuts owner draw.
Use a simple sensitivity check: hold implant volume and reimbursement flat, then test how one extra ICU day changes margin. If the added nursing and supply cost exceeds the post-implant management revenue on that case, the owner earns less even when clinical throughput looks busy. That is the real pressure point.