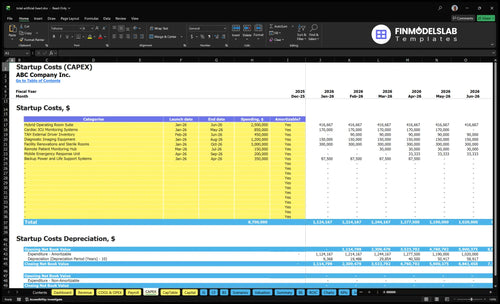
Total Artificial Heart Program Startup Costs: $50M+ CAPEX Before Ramp
You’re planning a high-acuity hospital service line, so the startup budget starts with infrastructure already in place This outline covers $50M in identified CAPEX, $2255K in monthly fixed overhead, $1745M in first-year leadership and admin payroll, pre-opening costs, working capital, and excluded hospital-scale costs These are researched planning assumptions for the first operating year and 60-month model, not vendor quotes, reimbursement guarantees, or clinical feasibility advice
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
This estimates capitalized startup assets only for a total artificial heart program, not launch cash or operating losses.
!
Capital only This calculator includes only startup CAPEX. It excludes payroll runway, salaries, training, payer contracting, deposits, debt service, working capital, inventory runway, reimbursement lag, and other operating expenses. Main spend is expected across Month 1 to Month 10, with contingency added on top of line-item CAPEX.
Calculate Fuding Needs
Startup cost breakdown
Startup cost summary for a total artificial heart program, split between major CAPEX and excluded launch cash needs.
Costs rise fast as the program moves from using an existing transplant center to adding new rooms, devices, and specialist staff. That shift changes both upfront CAPEX and monthly overhead.
Lean, base, and full launch cost bands for a total artificial heart program.
Scenario
Lean LaunchExisting Center
Base LaunchModerate Upgrade
Full LaunchMajor Buildout
Launch model
Start inside an established transplant or cardiac center and use existing ICU and perfusion capacity.
Run a standard program build with added staffing, payer readiness, training, and working capital.
Build a dedicated program with major facility expansion and a larger clinical team.
Typical setup
Keep new build light and limit added infrastructure to validated renovation work and core device support.
Add the modeled capex set, then carry about $225.5k in monthly fixed overhead for operations.
Expand the suite, ICU support, monitoring, and device handling while adding more surgeons, cardiologists, perfusionists, nurses, and technicians.
Cost drivers
Existing ICU capacity
perfusion coverage
validated renovation
limited new equipment
compliance setup
Facility lease
malpractice insurance
staff ramp
payer readiness
working capital
Facility expansion
more surgeons
more cardiologists
more perfusionists
more nurses and technicians
Planning rangeCAPEX only
$50M floorLowest setup
$8.7M plus working capitalMid build
Major buildout budgetHighest build
Best fit
Fits hospitals that already have transplant infrastructure and want the smallest new-build footprint.
Fits centers that need a real operating platform but can still lean on existing clinical space and shared services.
Fits systems that want a standalone heart failure platform and can fund heavy infrastructure and staffing growth.
!
Planning note: These scenario ranges are researched planning assumptions from the model, not vendor quotes or guaranteed prices.
How should I build a total artificial heart program financial model?
Build the Total Artificial Heart Program model from case volume first, then layer in device cost timing, payer mix, reimbursement lag, and staffing ramp. For Year 1, use 2 cardiac surgeons at 40%, 3 heart failure cardiologists at 50%, 4 perfusionists at 40%, 12 critical care nurses at 60%, and 2 device technicians at 30%. Here’s the quick math: 12% device and surgical kit cost, 3% specialized consumables, 4% referral commissions, and 15% transportation/logistics add up to 34% variable cost before payroll and overhead. Use base, downside, and upside cases so funding need changes with volume and payment timing.
Year 1 capacity
2 surgeons at 40% utilization
3 cardiologists at 50% utilization
4 perfusionists at 40% utilization
12 nurses at 60% and 2 technicians at 30%
Cash and cost
12% device and surgical kits
3% specialized consumables
4% referral commissions
15% logistics, or 34% total variable cost
How much money is needed to launch a total artificial heart program?
A Total Artificial Heart Program needs at least $50M in CAPEX before any facility renovation, and the final launch budget should be set by hospital readiness, case volume, device buying terms, and cash reserve policy; use How Do I Write A Business Plan To Launch Total Artificial Heart Program? to tie those assumptions into the plan.
Startup floor
Start with $50M CAPEX
Add facility renovation separately
Budget devices by procurement terms
Hold working capital for ramp-up
Opening burn
Fixed overhead: $2.255M/month
Year 1 admin payroll: $1.745M
Capacity starts at 40%
Plan around 16 implants/month
What hidden costs should a total artificial heart program budget include?
Hidden costs in a Total Artificial Heart Program budget sit far beyond equipment, and they usually show up first in launch work like credentialing, privileging, protocols, proctoring, payer contracting, and case-review admin. The cash hit gets bigger fast when you add $45K a month for malpractice insurance, $15K for FDA compliance and quality monitoring, and $85K for EHR and remote monitoring licensing. Separate pre-opening costs from working capital, because ICU stay exposure, blood bank readiness, pharmacy readiness, inventory timing, and reimbursement delays can drain cash before collections land.
Launch costs
Credentialing and privileging
Clinical protocol buildout
Proctoring and case review
Payer contracting setup
Cash drains
$45K monthly malpractice insurance
$15K monthly FDA compliance
$85K monthly EHR licensing
ICU, blood bank, pharmacy readiness
Key Takeaways
Facility buildout needs $37.85M across six to eight months.
Device startup adds $450K, plus validated consumable costs.
Governance needs $15K monthly for compliance and quality.
Staffing and working capital drive early cash burn.
Total Artificial Heart Program Core Five Startup Costs
Facility and Clinical Infrastructure Startup Expense
OR Suite
The launch budget is led by a $25M hybrid operating room suite from Month 1 to Month 6, plus $850K for cardiac ICU monitoring from Month 1 to Month 5 and $12M for diagnostic imaging from Month 1 to Month 8. That covers OR readiness, ICU bed capacity, sterile workflow, backup power, biomedical engineering, and post-implant recovery space.
ICU Systems
Build each line from units × quote × months. For this program, the inputs are room count, bed count, imaging scope, install timing, and service coverage. Facility renovations and sterile rooms are listed too, but the amount must be validated before it can enter the startup budget.
Cost Control
Keep the spend tied to implant volume, not broad hospital buildout. Phase equipment in only when the room is ready, get vendor bids early, and protect backup power and biomedical support. The real savings come from right-sizing ICU and imaging scope; the wrong cut is skipping readiness.
Scope Guard
Keep this expense separate from hospital acquisition or full construction. The only clean case is TAH-use space that directly supports surgery, monitoring, and recovery. If renovation pricing is still open, hold it as a validated placeholder, not a fixed number.
Launch Supplies, Payer Readiness, and Working Capital Startup Expense
Pre-Opening Cash
The hard part is not the implant itself; it’s the cash you burn before the first case. Plan for implant-related disposables, blood bank and pharmacy readiness, legal and consulting support, payer contracting, referral marketing, and early losses. Keep this separate from capital spending (CAPEX) because it still drains cash even when it is not capitalized.
Monthly Burn
Estimate the reserve by adding the monthly run rate and launch-only items. The listed overhead lines total $302K per month: $120K lease, $45K malpractice, $15K compliance, $85K EHR and remote monitoring, $12K utilities and biohazard, and $25K physician outreach.
Count monthly overhead first.
Add launch supply purchases.
Cover reimbursement lag.
Manage the Burn
Cut cash drag by buying to case schedule, not full shelf depth, and by closing payer terms before launch. Keep blood bank and pharmacy readiness intact, but avoid overstocking disposables that sit idle. The goal is simple: don’t let inventory timing and billing delay force a cash crunch.
Stage supplies to cases.
Contract payers early.
Limit idle inventory.
Timing Gap
A center can be clinically ready and still run short on cash because reimbursement comes after the implant date while supplies, staff, and readiness costs hit first. The working capital reserve should cover that timing gap plus early operating losses, so the launch date is driven by cash, not just the operating room calendar.
Device and Mechanical Circulatory Support Startup Expense
TAH hardware
Plan the Total Artificial Heart equipment line as patient-side hardware plus spares. It should cover the $450K external driver inventory from Month 2 to Month 6, backup components, perfusion equipment, and monitoring systems. Build the estimate from units, months of coverage, and validated quotes, since service and maintenance needs can change fast.
Cost build
This cost covers device startup, surgical kits, external driver support, and the tools needed to keep implants working after surgery. For Year 1, use 12% variable cost on device and surgical kits and 3% on specialized surgical consumables. The quick math is simple: price, volume, months of coverage, then validated supplier quotes.
Count every device and spare.
Separate kits from consumables.
Validate quotes before ordering.
Spend control
Keep the budget tight by staging purchases to case volume and keeping only the needed backup set on hand. Don’t lock in pricing without vendor validation, and don’t overbuy controllers or consumables before the implant schedule is clear. The best savings come from matching inventory to Month 2 to Month 6 demand, not from cutting clinical support.
Order to case schedule.
Track service intervals early.
Hold spare parts lean.
Procurement guardrails
Use one locked inventory list for drivers, backups, perfusion gear, and monitoring, then tie reorders to service assumptions and actual implant volume. This is a control cost as much as a device cost, so every item needs a unit count, a coverage window, and a signed-off quote before procurement.
Specialized Staffing, Recruitment, and Training Startup Expense
Opening Team
A Total Artificial Heart (TAH) program needs a full clinical bench before the first implant. Year 1 operating staff assumes 2 cardiac surgeons, 3 heart failure cardiologists, 4 perfusionists, 12 critical care nurses, and 2 device technicians. This cost covers recruiting, onboarding, and pre-open training, not ongoing payroll or working capital.
Payroll Base
Year 1 leadership and admin payroll is anchored by a $550K medical director, $750K chief surgical officer, $190K for 2 clinical care coordinators, $75K for billing and coding, and $180K for the administrator. Size it as headcount × salary × months, then add the cost of 24/7 coverage and coverage gaps.
Training Risk
Keep recruitment and training separate from payroll so you can see the real launch burn. The expensive part is overlap: surgeons, perfusion, ICU, and device support all need to be ready at once. One clean rule: if a role is not trained, the schedule is not truly 24/7, and onboarding risk rises fast.
Cash Timing
Model this as a startup cash item, not a one-time install. Pre-opening hiring, simulation, and cross-training hit before case volume does, so the budget must fund the gap between first hire and steady utilization. The clean budget split is pre-open recruitment, pre-open training, and Year 1 payroll plus working capital.
Regulatory, Credentialing, and Clinical Governance Startup Expense
Governance Stack
This cost covers FDA compliance, medical staff credentialing, privileging, quality reporting, policy work, transplant-program coordination, payer documentation, and institutional review needs where applicable. For planning, use $15K per month for compliance and quality monitoring, or $180K per year. Tie this budget to case approval workflows and quality files, and verify scope with counsel, compliance, and clinical leadership.
Budget Inputs
The estimate needs three inputs: months of coverage, staffing scope, and the number of approval files to maintain. Use 12 months if the program is running year-round, then add any one-time policy build, credentialing, and review setup costs. Keep it separate from facility and device capex, because this spend is mostly process support, not equipment.
Count credentialed clinicians first
Price monthly monitoring separately
Track case-file workload
Control The Spend
Keep costs down by standardizing policies, using one approval path, and reusing quality templates across cases. Don’t let every case start from scratch. The main savings come from faster documentation and fewer rework cycles, but quality can’t slip. If onboarding is messy, governance time balloons fast, and the monthly $15K planning figure can move up.
Use one policy library
Pre-build payer packets
Track exceptions by case
Approval File
Here’s the quick math: $15K monthly times 12 months equals $180K a year before any launch work. That budget should sit inside the case-approval file, quality folder, and payer packet so leaders can see what was approved, when, and by whom. Use counsel, compliance, and clinical leadership to confirm what’s required.