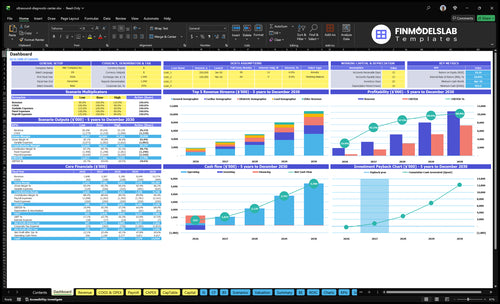
How Much an Ultrasound Center Owner Makes at $154K Monthly Revenue
An ultrasound center owner can make meaningful income, but only after clinical payroll, radiologist costs, rent, software, billing, insurance, and reserves are covered In the researched first-year case, revenue is about $185 million, with operating profit of about $504,000 before taxes, debt service, and reserves That equals a planning operating margin of about 27% By Year 5, the same model reaches about $1077 million in revenue and about $783 million in operating profit, but that assumes major volume, staffing, and utilization growth
Owner income$504kNet margin27% to 73%Revenue for target pay$1.9MBusiness difficultyHard
Want to test your ultrasound center income?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
!
Planning note: Research-based planning estimate only. Actual owner income depends on collections, payer mix, staffing, taxes, debt, and retained cash. It is not guaranteed salary, tax advice, or owner distribution advice.
Which drivers move ultrasound center owner income most?
1
Scan Volume
60%-88%
General sonographer capacity rises from 60% to 88% by year 5, so fuller schedules spread fixed cost across more scans and raise cash before taxes, debt service, and reserves.
2
Net Reimbursement
$100-$650
A better payer mix lifts net reimbursement per exam, so the same slot count produces more EBITDA and more owner take-home.
3
Exam Mix
120-240/mo
A heavier mix of higher-priced cardiac, lead, and general exams pushes the blended ticket up, and that feeds straight into owner cash.
4
Labor Load
$873K-$1.66M
Annual wages climb from about $873K in year 1 to $1.66M in year 5, so staffing and interpretation control has a big swing on EBITDA and owner take-home.
5
Fixed Overhead
$20.8K/mo
Fixed overhead holds at $20.8K per month, so every extra scan helps spread the rent, software, and service load across more revenue.
6
Billing Flow
5.8%-7.0%
Billing fees and referral commissions total 5.8% to 7.0% of revenue, so cleaner collections and fewer paid referrals keep more cash for the owner.
How many ultrasound scans per day to be profitable?
There isn’t one fixed scan count for the Ultrasound Center; break-even moves with net reimbursement, operating days, exam mix, staffing, and overhead. In Year 1, the center has $20,800 in monthly fixed overhead before payroll and about $72,708 in monthly payroll, against roughly $153,960 in monthly revenue, so the base case clears the fixed-cost wall. Here’s the quick math: use monthly fixed costs plus payroll, then divide by contribution per scan; if no-shows rise or payer collections fall, the required scans per day move up fast.
Base case
$153,960 monthly revenue
$72,708 monthly payroll
$20,800 fixed overhead
Base case clears the wall
What changes break-even
Net reimbursement per scan
Operating days per month
Exam mix and staffing
No-shows and collections
What profit margin can an ultrasound center reach?
An Ultrasound Center can reach an operating margin of 27% in Year 1, about 51% in Year 2, and about 73% in Year 5, before taxes, debt service, and reserves. That math depends on model assumptions, not generic healthcare averages, and the link between setup cost and margin starts here: How Much Does It Cost To Open An Ultrasound Center?. The margin expands as utilization rises, prices increase, and fixed overhead stays at $20,800 per month.
Margin drivers
27% operating margin in Year 1
51% operating margin in Year 2
73% operating margin in Year 5
$20,800 fixed overhead each month
Margin risks
Underused rooms can crush margin
Payer denials delay cash
Overtime raises labor cost
Weak referrals slow utilization
How much profit can an ultrasound center make?
An Ultrasound Center can make about $504,000 in Year 1 operating profit on about $1.85 million in revenue, before owner distributions, taxes, debt service, and reserves; by Year 5, the model shows about $7.83 million operating profit on about $10.77 million in revenue, but only with higher utilization, more sonographers, and expanded radiologist capacity. For the core KPI behind that profit, see What Is The Most Important Metric To Measure The Success Of Ultrasound Center?.
Year 1 profit
$1.85 million projected revenue
$504,000 operating profit
$872,500 payroll cost
$249,600 fixed overhead
Owner cash caution
Profit is not owner take-home cash
Exclude taxes and debt service first
Hold reserves for equipment and claims
Growth needs staff and radiologist capacity
Key Takeaways
Higher scan volume spreads fixed costs and lifts margin.
Net reimbursement depends on collections, denials, and payer mix.
Better mix and productivity raise revenue per slot.
Fixed overhead and fees make utilization the main break-even lever.
Compare low, base, and high ultrasound center income cases
Owner income scenarios
Owner income swings with scan volume, reimbursement, staffing, and fixed overhead. The opening year is much leaner than the mature Year 5 case, so the planning spread is wide.
Compare conservative, modeled, and upside owner take-home.
Scenario
Low CaseLean launch
Base CaseModeled base
High CaseHigh utilization
Launch model
This is the slower-fill opening case with tighter owner take-home.
This is the main plan case with steady opening-year utilization.
This is the strong-volume case with a much larger owner income pool.
Typical setup
About 27 scans/day, about $154k monthly revenue, 12% variable fees, $20.8k fixed overhead, and $872.5k annual payroll.
About 27 scans/day, about $154k monthly revenue, $20.8k fixed overhead, $872.5k annual payroll, and about $504k operating profit before taxes and reserves.
By Year 5, the model reaches about 85 scans/day, about $898k monthly revenue, heavier staffing, and about $7.8M operating profit before taxes and reserves.
Cost drivers
Scan volume
reimbursement per scan
staffing load
fixed overhead
billing and referral fees
Scan volume
payer mix
staffing schedule
fixed overhead
billing and referral fees
Scan volume
better utilization
larger staff
lower fee rates
fixed overhead
Owner income rangeBefore owner reserves
about $368kConservative profit
about $504kCore profit
about $7.8MUpside profit
Best fit
Use this to stress-test a slower ramp and a thinner owner draw.
Use this as the core case for hiring, pricing, and owner pay.
Use this to test upside if referral flow and utilization stay high into Year 5.
!
Planning note: Planning assumptions only; not guaranteed earnings, salary promises, tax advice, or distributions.
Ultrasound Center Core Six Income Drivers
Scan Volume and Utilization
Scan Volume and Utilization
Utilization is the share of available scan time that turns into completed exams. In Year 1, the model assumes 65% obstetric, 60% general, 70% lead sonographer, and 60% radiologist capacity. More completed exams spread the $20,800 monthly fixed overhead across more revenue, so owner pay improves once staff are already covered.
What matters most is completed volume, not booked slots. No-shows, schedule gaps, operating days, and room capacity all cut realized utilization, so a center can look busy and still miss cash. By Year 5, the model rises to 85%, 88%, 90%, and 90%, which should lift margin if collections stay clean and staffing stays tight.
Track Fill Rate, Not Just Bookings
Measure booked slots, completed exams, no-show rate, and open hours by modality every week. Here’s the quick math: more scans lower fixed cost per exam, but only if rooms, sonographers, and radiologist reading time all stay aligned. If one of those breaks, utilization drops and owner draw gets squeezed even when demand is there.
Push reminders, shorten gaps, and match staffing to the real schedule. Watch operating days and room capacity first, because those set the ceiling before demand does. A center that holds utilization near the Year 5 targets will usually keep more margin after payroll, rent, software, insurance, and admin are already paid.
Collections, Denials, and Referrals
Collections and Referrals
An ultrasound center can look full and still miss cash. This driver includes billing collections, authorization approval, coding accuracy, denials, and physician referral flow. Owner pay depends on collected cash, not scheduled visits, so weak follow-up can cut income even when volume is steady.
In the model, billing and collections fees take 40% of revenue in Year 1 and referral commissions take 30%, so only 30% is left before payroll, rent, and reads. By Year 5, those costs fall to 36% and 22%, which lifts cash retained to 42% before other overhead.
Track Cash Conversion
Watch collection rate, denial rate, days in A/R (accounts receivable), and referral count by physician. Here’s the quick math: collected revenue minus billing fees and referral commissions is what can pay the owner. If cash lags, profit on paper won’t fund draws.
Use a simple monthly check: exams ordered, exams completed, claims accepted, claims denied, and dollars collected. Fix the usual leak points fast: missing authorizations, coding errors, and slow referral follow-up. One clean referral can be worth more than a late scan.
Track denial reasons weekly
Match referrals to paid claims
Review authorization before scheduling
Measure cash by service line
Equipment and Facility Overhead
Fixed Overhead
Fixed overhead sets the floor. With $20,800 a month, or $249,600 a year, the center must clear rent, software, service, insurance, IT, utilities, and supplies before the owner sees profit. Higher exam volume spreads that base over more revenue, so the same site can pay the owner more when utilization rises.
This overhead includes $10,000 rent, $2,500 service contracts, $2,000 RIS/PACS, $1,800 EHR/billing, $1,500 utilities, $1,200 insurance, $1,000 IT, and $800 supplies and cleaning. Equipment financing and buildout are separate. If utilization slips, these costs stay fixed and squeeze take-home pay fast.
Hold the Base
Track monthly fixed overhead per completed exam and compare it with net collections, not scheduled visits. The key test is simple: more exams with the same $20,800 base lowers overhead per scan and raises cash left for owner pay. If no-shows or open slots rise, the overhead ratio gets worse.
Keep buildout and equipment debt in a separate forecast, then stress test 65%, 75%, and 85% utilization. That shows how many exams are needed to carry the fixed base without cutting the owner draw. One empty day a week can matter more than a small price change.
Exam and Service Mix
Service Mix Drives Revenue per Slot
Service mix is the share of obstetric, general, cardiac, lead sonographer, and radiologist-read work in the schedule. It changes income because Year 1 pricing ranges from $100 for radiologist reads to $550 for cardiac exams, so a shift toward higher-value cases lifts revenue per slot and can improve owner take-home.
Year 1 starts with zero cardiac sonographer count, so cardiac volume is a ramp, not an instant lever. That means the mix is bounded by skill, compliance, and referral flow. A faster shift can raise dollars per case, but it can also slow throughput if the team is not trained and the interpretation path is not in place.
Track Mix by Exam Type
Measure completed exams by type each week, not just total volume. The key inputs are case counts, price per exam, staff skill by service, and radiologist read load. One line to keep in mind: more cardiac work can mean more revenue, but only if staffing and reads keep up.
Track exam count by service line.
Match staff skill to case mix.
Watch radiologist read demand.
Test referral sources by exam type.
Use the mix forecast to see where owner cash comes from: completed exams × price by type. If the schedule shifts toward higher-priced cardiac work without enough trained sonographer coverage, the center can lose speed and create bottlenecks. If it stays too heavy on lower-priced exams, revenue per slot stays capped.
Payer Mix and Net Reimbursement
Net Reimbursement
This driver is the share of billed ultrasound charges that actually turns into cash. In Year 1, list prices run $300 for obstetric work and $550 for cardiac work, plus $100 for radiologist reads; by Year 5, they rise to $360, $650, and $120. The owner’s income depends on how much of that charge survives payer rules, denials, and contract cuts.
Medicare, commercial insurance, self-pay, and negotiated contracts all pay differently. If authorizations are weak or claims deny, booked revenue looks fine but bank deposits lag, so profit and owner pay fall even with a full schedule. Net collections, not sticker price, should drive forecasting, because the real question is what cash each exam clears after payer adjustments.
Measure Net Cash, Not Charges
Track net collection rate by payer and exam type. Compare billed charges to cash received, then split the gap by denials, authorization failures, and contract write-offs. That shows whether an OB scan at $300 or a cardiac scan at $550 is really paying as planned.
Separate Medicare, commercial, self-pay.
Track denial rate by CPT code.
Check authorizations before every visit.
Reprice yearly to $360, $650, $120.
What this hides: a full schedule can still produce weak cash if collections slip. Fixed costs still hit, so owner draw gets squeezed first. Tight billing controls and clean prior auth protect cash flow better than raising list prices alone.
Staffing Productivity and Interpretation Cost
Staffing Productivity and Read Cost
This driver covers sonographer pay, lead coverage, and radiologist interpretation fees. In Year 1, payroll is $872,500, including $240,000 for 30 sonographer FTEs, $110,000 for the lead sonographer, and $300,000 for the employed radiologist. Contracted radiologist fees add 30% of revenue in Year 1, so the owner’s income rises only when exams per paid clinical hour stay high.
Here’s the quick math: if staffing runs ahead of exam volume, gross margin gets squeezed fast. The key inputs are exams per paid clinical hour, overtime, contractor rates, idle time, and admin coverage. One line matters most: productivity beats headcount. If hours are paid but not filled with scans or reads, that labor cost shows up before the owner can pay themselves.
Track Hours, Not Just Headcount
Measure exams per paid clinical hour by sonographer and by radiologist. Split employed versus contract read cost, then compare that to revenue each month. If overtime or contractor use rises while idle time stays high, margin drops even if visit volume looks fine.
Track paid hours versus completed exams.
Flag overtime above plan.
Separate employed and contract reads.
Cut idle time and schedule gaps.
Match admin coverage to booked volume.
Use staffing plans that flex with demand. If a sonographer shift is open but demand is soft, owner pay gets hit twice: first by wage cost, then by lower utilization of fixed labor. Better staffing control protects gross margin, cash flow, and the draw the owner can safely take.