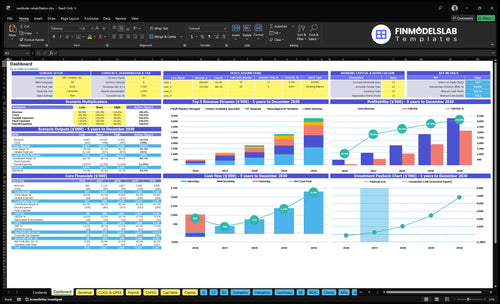
How Much Vestibular Rehabilitation Therapy Owners Can Make: $172K
Based on the model, first-year collected revenue is $481,560 from about 65 completed visits per week, with estimated pre-tax owner take-home of about $172,000 before taxes, reserves, debt service, and any unlisted clinician payroll This page covers visits, collections, payer mix, staffing, overhead, margin, and owner role assumptions across a five-year US practice model It does not cover personal debt, tax planning, legal advice, or guaranteed distributions
Owner income≈$172kNet margin18.5%Revenue for target pay≈$425kBusiness difficultyHard
Want the six income drivers that matter most?
1
Visit Volume
65/wk
Every kept slot helps because the clinic already carries fixed rent, software, insurance, and a $125K owner wage.
2
Net Collections
$143
A higher collected amount per visit lifts pre-tax profit faster than adding staff, because the room and systems are already in place.
3
Clinician Use
80%-85%
Higher chair time per clinician turns the same payroll into more billable visits, so EBITDA improves without new rent.
4
Retention
High
Keeping patients through the full plan and refilling cancellations protects the visit count you already staffed for.
5
Overhead
$121.8K
That is the annual fixed load from rent, software, insurance, utilities, waste, supplies, and fees, so it hits take-home every month.
6
Owner Role
$47K
After the $125K owner wage and reserves, this is the cash left for the owner to keep.
Want to test your own vestibular rehab owner salary?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
!
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
How do you check owner income in the financial model?
How many vestibular rehab visits are needed to pay the owner?
To cover a $125,000 owner salary in Year 1, Vestibular Rehabilitation Therapy needs about 57 completed visits per week, or $350,300 of total cost coverage, with about $143 collected per visit. The model shows about 65 completed visits per week, so the cushion is only 8 visits a week. That’s tight, because booked visits do not pay bills and demand, physician referrals, and plan-of-care completion are not automatic.
Break-even math
57 visits per week
$350,300 total cost coverage
$143 collected per visit
65 visits in the model
Risk points
8-visit weekly cushion
Booked visits still miss bills
Referrals are not automatic
Plan-of-care completion can slip
How does reimbursement affect vestibular rehab practice profit?
If you’re opening Vestibular Rehabilitation Therapy, reimbursement can change profit fast: at modeled utilization, average collected revenue is about $143 per completed visit, built from $175 senior specialist visits, $145 staff physical therapist visits, and $110 physical therapist assistant visits. A $10 drop in average collection cuts yearly revenue by about $33,660 across 3,366 annual visits before cost effects, so the same visit count can still produce very different cash. If you want the launch context, see How Do I Launch A Vestibular Rehabilitation Therapy Business? This is planning, not billing or compliance advice.
What drives profit
$143 average collected per visit
$175, $145, and $110 visit mix
$10 less per visit hurts cash
$33,660 yearly revenue drop
What to check first
Verify payer contract rates
Check allowed amounts locally
Track denials and collection speed
Test cash-pay pricing too
Should a vestibular rehab owner hire another therapist?
For Vestibular Rehabilitation Therapy, hire another therapist only when schedule fill rate and referrals can support the added visits. Year 1 uses 1 senior specialist, 1 staff physical therapist, and 1 physical therapist assistant at about 65 weekly completed visits; Year 2 can reach about 144 weekly visits and $1,126,290 revenue, but take-home still depends on wages, payroll taxes, benefits, supervision time, and collections. If utilization lags, extra capacity can lift revenue and still hurt cash, so admin support, longer hours, and referral partnerships are safer first steps.
When to hire
Fill rate must stay high
Referrals must keep growing
65 weekly visits is Year 1
144 weekly visits is Year 2
Safer first moves
Add admin support first
Extend hours before payroll
Build referral partnerships
Watch cash, not just revenue
Key Takeaways
Completed visits, not bookings, set revenue.
A $10 collection swing changes revenue by $33,660.
Utilization helps only when payroll stays aligned.
Keep fixed costs lean until referrals prove capacity.
Compare low, base, and scaled vestibular rehab owner income scenarios
Owner income table
Owner income rises with visits, pricing, and staffing mix. The model gets much stronger by Year 5, but extra clinician payroll can still trim take-home.
Low, base, and scaled cases for owner income planning.
Scenario
Low CaseDownside
Base CasePlan case
High CaseUpside
Launch model
Income stays in the opening-year band while the clinic proves demand.
Income follows the modeled scaling path as volume and staffing rise.
Income jumps in the mature-growth case if throughput stays high.
Typical setup
The clinic opens with 65 weekly visits at $143 per visit, $481,560 revenue, $121,800 fixed overhead, and $228,500 known payroll before reserves.
Year 2 scales to 144 weekly visits and $1,126,290 revenue, with more therapists and payroll pressure.
Year 5 runs at 531 weekly visits and $4,284,960 revenue, so margin depends on keeping clinician payroll in line.
Cost drivers
visit-level costs
fixed overhead
known payroll
slower capacity
reserves
more weekly visits
higher collections
added staff
payroll growth
fixed rent
531 weekly visits
higher price mix
larger team
payroll dilution
reserve need
Owner income rangeBefore owner reserves
$172,000Opening year
Year 2 scaling bandScaling year
Year 5 mature bandMature year
Best fit
Use this to test early cash strain and staffing discipline.
Use this for standard planning and lender talks.
Use this to test aggressive growth with a fuller care team.
!
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or profit distributions.
Vestibular Rehabilitation Therapy Core Six Income Drivers
Completed Visit Volume
Completed Visit Volume
Completed visits are the revenue ceiling here: Year 1 models about 3,366 visits, or 65 per week. That includes evaluations and follow-up care actually delivered; booked slots do not pay if the patient cancels or never starts care. In a fee-for-service clinic, more completed visits raise revenue before fixed costs and decide how much the owner can take home.
Here’s the quick math: at $143 net collection per visit, every 10 more completed visits per week adds about $74,360 a year before variable costs. Referrals from physicians, ear, nose, and throat offices, neurology, audiology, and balance clinics feed that volume, so weak referral flow or high no-shows caps income fast.
Track completions, not bookings
Measure inquiries → booked → completed visits each week, plus cancellations and no-shows by clinician. If bookings rise but completions stall, cash flow will lag and payroll still clears. Staff to completed volume, not schedule fill, so the owner does not add labor before referrals and follow-through can support it.
Protect the 65-per-week base by tightening referral follow-up and patient education, especially before the first visit and through the plan of care. Keep a simple watch on completed visits by source, since that shows which referral partners actually turn into revenue. If cancellations stay high, the revenue ceiling stays low even when demand looks strong.
Fixed Overhead Control
Keep Fixed Overhead Lean
$10,150 a month in fixed overhead hits take-home before the first visit is completed. That equals $121,800 a year, and it includes rent, EMR and HIPAA software, liability insurance, utilities, janitorial and medical waste, office supplies, and memberships. Because these costs barely move with volume, weak referral flow can shrink owner pay fast.
The key check is fixed overhead per completed visit. Use completed visits, not booked slots, because cancellations still leave rent and software running. Keep the lease, admin stack, and nonclinical spend lean until referral flow proves the clinic can fill capacity.
Track Cost per Completed Visit
Track the monthly base and compare it to collected revenue and completed visits. If referrals are still light, every added dollar of fixed cost has to be covered by future volume, so delay extra space, extra software, or extra admin until the schedule holds.
A simple control is fixed overhead ÷ completed visits. When that ratio stays high, owner draw gets squeezed even if the clinic looks busy. Hold rent at $6,500, keep EMR and HIPAA software at $850, and protect cash for months when visits come in below plan.
Net Collection Per Visit
Net Collection Per Visit
Your real revenue per visit is not the charge on the superbill; it is what actually gets collected after payer mix, allowed amounts, cash-pay pricing, denials, and collection lag. In this model, Year 1 average net collection is about $143 per completed visit, with modeled visit prices of $175 for senior specialist visits, $145 for staff physical therapist visits, and $110 for physical therapist assistant visits.
That number hits owner income fast. A $10 change in net collection across 3,366 annual visits changes revenue by about $33,660 before fixed costs, wages, and owner pay. If reimbursement drops or denials rise, cash flow tightens even when schedules stay full. Verify local reimbursement assumptions before hiring.
Track reimbursement before you add staff
Track net collection per completed visit by payer, visit type, and clinician. Here’s the quick math: collected cash divided by completed visits. Watch denial rate and days to collect, because collection lag delays payroll support and can make growth look stronger than it is. Keep the forecast tied to actual allowed amounts, not posted charges.
Test whether senior specialist visits, staff physical therapist visits, and physical therapist assistant visits really collect near $175, $145, and $110. If the local average is below $143, cut hiring plans or raise cash-pay pricing before fixed costs lock in. That protects margin and the owner’s draw.
Plan-of-Care Retention And No-Shows
Plan-of-Care Retention
This driver is about how many referred patients finish the clinically needed visit plan, not just how many get booked. Revenue comes from completed monthly treatments, so cancellations and no-shows hit income right away while rent, software, insurance, and salaries still run.
Here’s the quick math: if average visits per case falls, the clinic sells fewer treatment sessions without adding marketing spend. Patient education materials also matter here, at 25% of revenue in Year 1 and 17% by Year 5, because home programs and adherence help patients complete care appropriately. Retention should mean finishing the right plan, not adding unnecessary visits.
Track Completed Visits, Not Booked Slots
Measure average visits per case, completed follow-ups, and the cancellation/no-show rate each month. Compare booked visits to completed visits by clinician and referral source so you can see where patients drop out. A full schedule on paper does not pay the bills if the chair stays empty.
Use discharge timing, reminder calls, and patient education to support adherence, then watch whether completions rise without pushing extra visits. The key question is simple: are referrals turning into finished care and collected revenue, or just into open calendar slots?
Owner Role, Reserves, And Reinvestment
Owner Pay, Profit, and Coverage
Owner income here is split across wage, profit, reserves, and distributions. In the Year 1 model, the clinic director role pays $125,000 and known Year 1 costs leave about $46,987 profit, so the owner’s take-home depends on whether they treat patients, manage referrals, or hire coverage.
If the founder steps out of clinical work, replacement labor can lift revenue capacity but still cut distributions. That’s because extra payroll, taxes, and supervision often rise before cash does. Profit is not pay; only the cash left after payroll and reserves is safe to draw.
Keep Cash Before Increasing Draws
Track collections, payroll, and reserve cash separately so you know what is truly available to pay the owner. Hold back cash for billing delays, staff pay, marketing tests, equipment, and expansion before increasing distributions. If visits rise but collections lag, the business can look healthier on paper than it is in the bank.
Use a simple rule: fund the clinic director salary, then keep a reserve buffer, then pay distributions from leftover cash. If you hire coverage, model the added wage against the expected visit lift before promising a higher owner draw. More revenue does not always mean more take-home.
Clinician Utilization
Clinician Utilization
Utilization is how full your paid treatment capacity is. In Year 1, the model uses 65% for the senior specialist, 60% for the staff physical therapist, and 55% for the physical therapist assistant; by Year 5, all three reach 85%. Higher utilization lifts revenue only when collections rise faster than payroll, because empty slots still carry wage, benefit, and supervision cost.
Here’s the quick math: more filled visits increase top-line income, but no-shows, documentation time, and slow payer cash can still block owner pay. If you add clinicians before demand is steady, you raise capacity first and profit later. One clean rule: fill hours before you add heads.
Track Paid Hours, Not Just Bookings
Measure utilization as completed treatment hours divided by available paid hours. Track it by role, since the Year 1 mix is different for each clinician, and compare it with net collection per visit and payroll. If booked visits look strong but completions lag, the owner still feels the gap in cash flow and take-home pay.
Use staffing plans that match referral flow. Watch wages, payroll taxes, benefits, supervision time, and cancellations together, because those costs can outrun the revenue gain from a fuller schedule. The best test is simple: if a higher utilization rate does not improve margin after labor cost, it is not helping owner income.