How To Open A Biofeedback Therapy Clinic In 3 To 6 Months
You’re opening a clinical service where readiness matters before marketing volume This launch plan covers 3 to 6 months of setup across licensing, rooms, sensors, intake, staffing, referrals, and first bookings, with a 5-year model used only to check capacity, timing, and cash runway
Time to Open3-6 monthsSetup windowLaunch Sequence7 stagesCompliance firstKey BottleneckLicense gateProvider coverageFirst Revenue StepPaid evalIntake ready
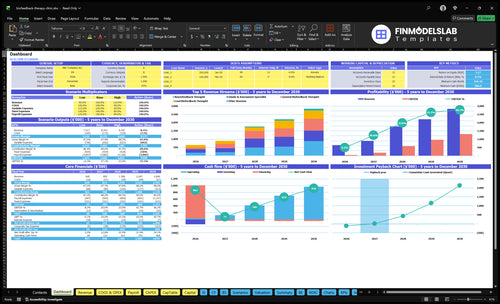
Launch timeline
Short web summary of the launch plan; the XLSX export contains the detailed Gantt Chart.
How long does it take to open a biofeedback clinic?
A Biofeedback Therapy Clinic usually takes 3 to 6 months to open. Faster launches use an existing compliant clinical space, cash-pay intake, trained providers, and ready equipment; slower launches get delayed by payer credentialing, lease buildout, state approvals, device delivery, EHR setup, clinician hiring, and weak referral development. The big bottleneck is usually licensed-provider readiness plus the payer or referral pipeline, so don’t promise an opening date until equipment, documentation, scheduling, and first referral sources are live.
Faster launch path
3 to 6 months is the planning range.
Use an existing compliant clinical space.
Start with cash-pay intake.
Keep equipment and staff ready first.
Slower launch path
Allow time for payer credentialing.
Expect lease buildout and state approvals.
Finish EHR setup and clinician hiring.
Do not open before referrals are live.
What are common biofeedback clinic launch mistakes?
The biggest launch mistake for a Biofeedback Therapy Clinic is opening before the basics are ready: clinical protocols, documentation, staff training, device calibration, payer workflow, referral flow, and patient education. Don’t advertise services or book patients until consents, assessment forms, and intake steps are final. A soft open beats a full schedule when onboarding is still messy, because unclear explanations can stop patients before treatment starts.
Common launch mistakes
Don’t advertise before scope is verified.
Don’t book before consents are final.
Don’t buy devices without vendor training.
Don’t skip outcome tracking and follow-up.
Readiness checks first
Run a mock intake before launch.
Test a mock session end to end.
Do a billing test with payer workflow.
Review privacy and referral handoff.
Do you need a license to open a biofeedback clinic?
Yes, a Biofeedback Therapy Clinic may need state licensure, but the answer depends on scope of practice, provider credentials, supervision, treatment claims, and payer contracts across 50 states. What Is The Most Critical Measure Of Success For Your Biofeedback Therapy Clinic? should be checked before lease signing because BCIA certification supports training credibility but doesn’t replace a required clinical license.
License Triggers
Diagnosing anxiety, pain, migraines, or stress disorders
Treating under medical or mental health scope
Billing insurers under clinical provider contracts
Advertising measurable treatment outcomes or symptom relief
Scope and licensing decide who can treat patients.
Equipment setup shapes first visits and cancel rates.
HIPAA-compliant intake cuts billing rework and delays.
Pricing and referrals drive the first bookings.
Clinical Licensing And Scope
Clinical Scope
Clinical licensing and scope decide who can deliver care, what claims staff can make, and what can be billed. For a biofeedback therapy clinic, that means the launch can’t move cleanly until the state scope review, provider credential file, malpractice coverage, consent language, and approved service descriptions are in place.
If scope is unclear, opening slips fast because hiring, marketing copy, intake forms, and billing setup all depend on it. One clean rule: no public promise before the clinical rule is written.
Verify Before Hiring
Start with the licensed clinical lead, then confirm supervision rules and payer requirements before you train staff on claims language. That keeps the clinic from opening with the wrong service mix or a billing setup that can’t support day-one revenue.
Confirm the clinical lead’s license.
Document supervision by role.
Approve service descriptions in writing.
Match consent forms to scope.
Train staff on allowed claims only.
What this protects: fewer complaint issues, fewer payer disputes, and a safer first month. What this estimate hides is simple—if the scope review runs late, everything downstream waits, even if the room is ready.
1
Equipment And Treatment-Room Setup
Room and Equipment Ready
In a biofeedback clinic, installed devices, tested sensors, vendor training, and active software licenses decide whether the first visit feels smooth or messy. If room privacy, calibration, or data capture is weak, sessions get canceled, notes get delayed, and the clinic may not be ready to open on time.
This setup also carries a real cost load: direct equipment and software licensing are 15% of Year 1 revenue. That spend only works if the lease is ready, the EHR workflow is live, and patient safety steps are already tested in the room.
Test the Full Room Flow
Match each device to the service line first, then prove the room works with a live test. Clean sensors, document calibration, and run one full patient flow from check-in to session close. If staff cannot complete the full workflow without help, the room is not launch-ready.
Confirm private rooms are built out.
Test data capture before opening.
Finish vendor training early.
Align setup with EHR workflow.
Document calibration after each device.
Watch the weak links: lease delays, training gaps, or missing safety steps. Those problems show up fast as longer first visits, more canceled sessions, and extra rework in the first week.
2
HIPAA, Intake, And Documentation Workflow
HIPAA Intake Ready
For a biofeedback clinic, HIPAA-compliant EHR, scheduling, consents, privacy policies, assessment forms, progress notes, outcome tracking, and billing documents all need to work before soft opening. If they don’t, the clinic can still open the doors, but it won’t be ready for real patient flow, clean follow-up, or day-one billing.
This launch driver depends on compliance review, payer setup, pricing, and staff training. The bottleneck is slow intake or missing documentation, because one missed consent or note can force rework, delay claims or superbills, and make first visits feel messy for both patients and staff. That also means more billing rework loops.
Test the Patient Flow
Run one full mock visit before opening: online booking, patient intake, consent capture, provider note templates, superbill or claim workflow, and follow-up reminders. If any step breaks, fix it before soft opening so the team is not learning in front of paying patients.
Confirm EHR fields match services.
Check consents before first visits.
Train staff on missing-document follow-up.
Test billing export and claim steps.
3
Provider Staffing And Training
Provider Staffing And Training
Staffing is the launch gate here because this clinic can’t open safely if the right roles aren’t covered on day one. Year 1 readiness means 1 lead biofeedback therapist, 1 neurofeedback therapist, 1 general biofeedback therapist, and 1 intake and assessment specialist. Capacity assumptions are only 65%, 60%, 55%, and 75%, so the first schedule must stay inside those limits or sessions get overbooked and quality slips.
This driver also affects patient safety. If training is weak, the clinic can’t rely on consistent session flow, supervision, or handoffs between front desk and providers. A slow start on equipment training, documentation workflow, or referral volume can delay first visits, create intake bottlenecks, and push the team into reactive scheduling instead of controlled launch-week coverage.
Launch-Week Coverage Plan
Before opening, assign launch-week roles, confirm training for each service line, define supervision, and schedule mock sessions. One clean rule: no mock session, no live slot. Tie front-desk handoffs to the intake specialist so new patients move from call to assessment without gaps, and keep the first calendar sized to the Year 1 coverage assumptions, not hoped-for demand.
Use the staffing plan as a scheduling cap, not a wish list. If the lead therapist is at 65% coverage and the general therapist at 55%, then opening-day templates should leave buffer for charting, room turnover, and unexpected no-shows. That keeps day-one operations realistic, protects patient safety, and avoids the cash drag of empty or canceled appointments caused by poor handoff timing.
Match roles to service lines.
Test supervision before first visit.
Run mock sessions end to end.
Train front desk on handoffs.
Cap slots to coverage limits.
4
Payer, Pricing, And Referral Readiness
Cash Pay, Payers, and Referrals
When the clinic opens, patients need a clear first payment path. If cash-pay evaluations, package pricing, and superbills are not set, calls turn into confusion and bookings slow. A superbill is an itemized receipt for out-of-network reimbursement. The first revenue path depends on answering one question fast: can a patient pay today, or do they need an insurer?
The launch prices must be locked before day one: $300 intake assessment, $140 lead biofeedback, $200 neurofeedback, and $120 general biofeedback in Year 1. If the team waits on insurer credentialing without a cash-pay offer, the clinic can open on paper but not actually convert inquiries. That delays first bookings and leaves staff time idle.
Build the First-Revenue Workflow
Confirm the billing flow before opening: who collects payment, when a superbill is issued, and how referrals are logged. Write a one-page referral sheet for physicians, therapists, and wellness partners so they know the service mix, prices, and who to send. Train intake staff to explain payment options in one sentence and route each caller to the right next step.
Here’s the quick math: the clinic needs a ready answer for each of these paths on day one — cash-pay, insurer credentialing, physician referrals, therapist referrals, and wellness partnerships. Build a payer checklist, test the script with mock calls, and verify the billing setup before soft opening. If the script is weak, patients hear mixed messages and the first visit stalls.
Set launch prices before marketing.
Write one referral one-pager.
Test superbill and payment steps.
Build payer checklist and assign owners.
Train intake script for insurance questions.
5
Patient Acquisition And Soft Opening
Patient Acquisition And Soft Opening
Patient acquisition and soft opening matter because they decide whether the clinic opens with booked visits or with empty slots. For a biofeedback therapy clinic, the first signal is not ad volume; it’s whether local search, condition pages, and outreach can turn interest into scheduled intake visits before full launch. One clean line: traffic without trust does not pay the rent.
This launch driver depends on scope approval, pricing, intake workflow, and room readiness. If the consultation script is weak or the schedule is too open, you get noise instead of usable demand. That slows first-day operations, makes intake-to-treatment conversion hard to track, and can leave the team idle while the launch window keeps moving.
Control First-Week Demand
Use a soft-opening schedule with limited first-week slots, then test the full path from inquiry call to booked intake to first treatment. Make sure the front desk can explain biofeedback in plain language, follow the referral process, and record conversion from intake to treatment. If calls are slow or unclear, fix that before opening wider.
Build the launch list around local search presence, condition-specific pages, and a provider outreach list. Invite referral partners before opening, then track whether each source can schedule fast enough to fill the limited slots. What this setup hides is simple: if the clinic cannot answer, educate, and book quickly, demand will leak out before the first week is over.