How To Open A Direct Primary Care Practice In 7 Months
You’re moving from insurance billing to patient memberships, so the launch work is legal setup, clinical workflows, systems, and first-member enrollment This guide covers the opening path for a US direct primary care practice over a 7-month breakeven ramp, with launch validation tied to $987,000 Year 1 revenue, Month 6 cash need, staffing, vendors, and patient acquisition
Time to Open7 monthsLaunch runwayLaunch Sequence10 stagesEntity firstKey BottleneckCompliance gateApproval pathFirst Revenue StepMembership signupIntro pricing live
Launch timeline
Short web summary of the launch plan; the XLSX export has the full Gantt Chart.
If you need first patients for a Direct Primary Care Practice, start with ethical local outreach before opening, then use your founder network, community education, local search, referral ties, employer conversations, and a waitlist; first revenue should come from pre-opening enrollment and opening-month memberships. For a launch map, see How To Launch Direct Primary Care Practice?
Year 1 can be priced at $99 individual, $199 family, and $49 small business plans, with a 45%/30%/25% mix and a $120,000 marketing budget at about $85 CAC (customer acquisition cost).
Start before opening
Do ethical local outreach first
Use founder network early
Ask former patients where allowed
Build a waitlist fast
Make the offer clear
State access in plain words
Define scope and limits
Share response times up front
Say what's not included
What DPC launch mistakes create the most risk?
If you launch a Direct Primary Care Practice before the legal and operating basics are done, the biggest risk is a fast cash squeeze and a messy member experience. The highest-risk mistakes are opening before the membership agreement, malpractice, and HIPAA workflows are ready, then underestimating ramp time. Here’s the quick math: by Month 6, minimum cash needs to be $552,000, and Month 7 breakeven only works if onboarding and employer outreach stay on track.
Big launch risks
Open before legal docs are done
Use unclear membership terms
Skip local positioning work
Hire before demand checks
Ready-before-launch check
Membership agreement in place
Malpractice coverage active
HIPAA workflows ready
EHR, telehealth, payment, portal, phone, scheduling, intake set
How long does it take to start a DPC practice?
Month 1 to Month 7 is the realistic launch-to-breakeven window for a Direct Primary Care Practice. You can open earlier, but breakeven is not opening day; it depends on approvals, payment setup, portal readiness, and patient outreach. Website work runs Month 1 to Month 3, and equipment work can stretch from Month 2 to Month 4 or even Month 1 to Month 5.
Launch setup
Set up the entity in Month 1.
Finish compliance review early.
Secure malpractice coverage before opening.
Build the facility, EHR, and telehealth stack.
Opening blockers
Wait for membership agreement approval.
Confirm payment processing and portal readiness.
Track equipment delivery and workflow testing.
Run pre-enrollment EHR tests before go-live.
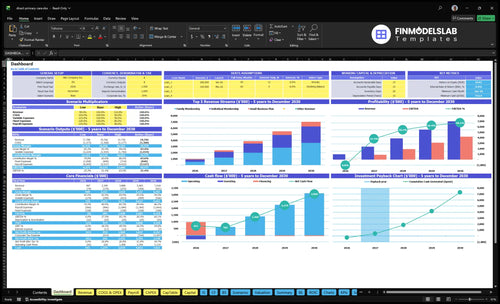
Direct Primary Care Practice Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Validate whether the DPC practice is ready to open
Launch readiness checklist
Use this go-live approval checklist before opening the practice.
1Compliance
Business entity formedCritical
The practice needs a legal entity before contracts, banking, and licenses move forward.
Physician license verifiedCritical
The lead physician must be licensed and in good standing before any patient care starts.
Malpractice and liability boundCritical
Malpractice at $2,500 and liability at $400 should be active before opening day.
2Site
Lease and permits clearedCritical
The clinic space must be approved before buildout, staffing, and patient visits begin.
Utilities and internet liveHigh
Power, water, and internet have to work on day one for visits and admin work.
Exam rooms and supplies readyHigh
Rooms, furniture, and basic supplies should be ready before the first patient arrives.
3Systems
EHR configuredCritical
The EHR, or electronic health record, must support charting, orders, and visit notes.
Telehealth workflow testedHigh
Telehealth has to work before launch because it is part of the service model.
HIPAA workflows validatedCritical
Patient data handling must meet HIPAA rules before any real records are stored.
4Offer
Membership agreement approvedCritical
The membership contract must be clear on fees, access, and service limits.
Payment and enrollment liveCritical
New members need a working path to join and pay before first revenue starts.
Patient access rules setHigh
Response times, visit channels, and refill rules should be set before opening.
5Staffing
Core clinical hires onboardedCritical
The launch team needs the physician, nurse, assistant, and manager roles covered.
Coverage schedule confirmedHigh
Opening coverage has to match patient demand, call flow, and admin work.
Staff training completedHigh
The team must know intake, visits, escalations, and patient communication before launch.
6Financials
Launch cash runway reviewedCritical
Cash must cover the Month 6 low point before the model reaches breakeven in Month 7.
Monthly overhead lockedHigh
Rent, utilities, compliance, and other fixed costs need a locked monthly budget.
Breakeven month approvedCritical
The team should agree on the Month 7 breakeven path and Month 20 payback target.
Which launch drivers decide whether your DPC opens cleanly?
1Regulatory Readiness
License gate
No one enrolls safely without entity setup, malpractice, compliance workflows, and signed terms; delays drop when these are done.
2Membership Model
$116.50/mo
A clear $99/$199/$49 offer and 45/30/25 mix make the membership easy to explain and easier to close.
3Clinical Setup
Day-1 flow
Tested intake, scheduling, refill rules, and referral steps keep day-one care moving and reduce physician overload.
4Tech Stack
$167K build
Electronic health record, portal, telehealth, and website must work together before opening or billing breaks and intake slows.
5Patient Pipeline
$85 CAC
$120K in Year 1 marketing and an $85 CAC help build warm members before opening month.
6Runway Check
M6 $552K
$552K minimum cash and Month 7 breakeven make runway the last gate before growth can breathe.
Regulatory And Legal Readiness
Legal Readiness
For a direct primary care practice, launch is binary: you can’t safely enroll members until the entity, physician license, malpractice coverage, and patient agreement are in place. The known monthly legal run rate is $3,500 for malpractice at $2,500, general liability at $400, and professional licenses and compliance at $600.
What this setup includes is state review, corporate practice rules, scope of services, privacy workflows, cancellation terms, and excluded services. If any one piece is late, opening slips and day-one onboarding gets messy, because patients need clear terms before the first visit and before any membership charge starts.
Pre-Open Legal Check
Get the legal stack done in order: entity review, physician licensing, insurance binders, and signed membership terms. The readiness signal is simple: state review completed, coverage active, and the patient-facing agreement ready to use. That is what keeps opening on time and avoids a stop-start launch.
Before the first member joins, verify these items and document them:
State corporate practice review
Active physician licenses
Malpractice binder at $2,500/month
General liability at $400/month
Compliance budget at $600/month
Signed terms for privacy and cancellations
Excluded services spelled out clearly
1
Membership Model Design
Simple Membership Terms
Opening day depends on a membership offer people can understand fast. If the practice can’t say who it serves, what’s included, and what costs extra, enrollment slows and billing disputes start on day one. Year 1 pricing is $99 individual, $199 family, and $49 small business; with a 45% / 30% / 25% mix, the weighted monthly fee is about $116.50.
Panel limits, lab rules, medication policies, and employer terms also shape capacity. If those terms are vague, staff will improvise, patients will push back, and the physician gets pulled into pricing questions instead of care. The launch signal is simple: one patient or one employer should be able to understand the offer in a single visit or meeting.
Lock the Offer Before First Enrollments
Before opening, turn the model into a one-page membership sheet and a signed agreement. Test it with three cases: one individual, one family, and one small business. Confirm who is accepted, what visits are included, how labs and medications are billed, and the panel limit the practice can support so intake does not outrun staffing.
Write access rules and exclusions.
Set lab and medication billing.
Define family and employer terms.
Cap panel size before launch.
Weak pricing design does more than slow sales; it creates refunds, confusion, and wasted staff time after opening. If the offer takes more than one meeting to explain, enrollment will lag and cash comes in later than planned. Clean terms help the front desk quote faster and keep day-one service smooth.
2
Clinical Operations Setup
Clinical Workflow Readiness
If the day-one workflow is messy, the first members feel it fast. A direct primary care practice has to open with intake, appointment scheduling, patient onboarding, secure messaging, refill rules, referral routing, lab coordination, documentation standards, and after-hours boundaries already set.
The plan shows 10 primary care physicians, 10 registered nurses, 10 medical assistants, 10 practice managers, and 10 marketing managers starting in Month 1, with the billing and administrative specialist starting in Month 13. That makes tested handoffs critical, or the physician ends up doing admin work and care slows down.
Test Every Handoff Before Go-Live
Dry-run the full path before the first member arrives: new patient intake, visit booking, onboarding, refill requests, lab orders, referrals, and secure messaging. The readiness signal is simple: staff can run the workflow without guessing who owns each step.
Use the Month 1 team to prove it works. If the physician has to chase labs, rewrite notes, or answer refill questions after hours, opening day will run hot. Clear rules now reduce care delays and keep physician overload down during early ramp-up.
Write refill rules in advance.
Set lab coordination ownership.
Define after-hours response limits.
Test secure messaging end to end.
Standardize visit documentation templates.
3
Technology And Vendor Stack
Tech Stack Ready at Launch
If the Electronic Health Record (EHR), membership billing, portal, telehealth, payment, scheduling, phone, website, and secure messaging are not live together, the practice cannot run cleanly from day one. The launch stack is not just software setup; it is the intake path for members, the way visits get booked, and the way money gets collected.
Here’s the quick math: $45,000 for EHR setup in Month 1 to Month 3, $35,000 for telehealth in Month 1 to Month 2, $32,000 for patient portal and membership software in Month 2 to Month 3, and $18,000 for the website and enrollment portal in Month 2 to Month 4. The main bottleneck risk is simple: untested billing or portal workflows can slow signups, payment collection, and first-day care.
Test Billing and Portal Workflows Before Opening
Plan the setup around the full member journey: enroll, pay, book, message, and visit. The practice should verify each vendor handoff before launch, because the ongoing telehealth and EHR fees are 55% of Year 1 revenue, so mistakes here hit both operations and cash flow fast.
Use one pre-open checklist for the web form, portal login, membership billing, payment processing, and telehealth visit flow. Make sure staff can complete a test signup, send a secure message, schedule a visit, and process a payment without manual workarounds. If any step breaks, opening day turns into support triage instead of patient care.
Confirm EHR data fields match the membership plan.
Test portal access before taking members.
Run a fake payment from start to finish.
Check telehealth links and message routing.
Assign one owner for vendor go-live fixes.
4
Patient Acquisition Pipeline
Pre-Launch Patient Pipeline
For a direct primary care practice, the patient pipeline is what turns an open date into real revenue. You need signed or warm members before opening month, not just ads, because the model depends on day-one enrollment and early recurring cash. With a $120,000 Year 1 marketing budget and $85 customer acquisition cost (CAC), the plan only works if local search, physician outreach, community education, employer conversations, referral links, and a waitlist are live before launch.
Here’s the quick math: the Year 1 revenue target is $987,000, and the early mix assumes 45% individual, 30% family, and 25% small business plans. If the pipeline is thin at opening, the practice starts with more cash strain and slower member growth, which pushes pressure into the run-up to Month 7 breakeven. One clean rule: no warm pipeline, no safe open.
Build the Waitlist First
Sequence the work before opening: local search setup, physician network outreach, employer conversations, and community education, then track each lead to a signed member or warm prospect. A ready pipeline should show where members came from, what plan they want, and when they can start. That keeps the opening date tied to real demand, not hope.
Track signed and warm leads weekly.
Separate individual, family, employer.
Test referral scripts before launch.
Confirm waitlist handoff and follow-up.
If early channels don’t fill the waitlist, the first months rely on paid demand at an average $85 CAC, and that can stretch cash before the clinic reaches steady volume. The practical check is simple: members in hand, clear plan mix, and a repeatable follow-up process before the first day.
5
Financial Runway Validation
Runway and Ramp Control
This launch driver decides whether the practice can open with enough cash to absorb the slow member ramp. The base load is $14,000 per month for facility and admin overhead, before $40,800 monthly payroll and $120,000 in Year 1 marketing, so opening on time depends on cash, not just sign-ups.
Here’s the quick math: the model needs $552,000 minimum cash by Month 6, with breakeven in Month 7 and payback in Month 20. If panel growth lags or staff is added too early, the clinic can miss day-one access targets and burn runway before members cover fixed costs.
Test the ramp before lease signing
Build the launch plan around member count, staff timing, and physician capacity. Validate how many members are needed to cover overhead, then match hiring to that curve so payroll does not outrun demand. One clean rule: don’t add cost faster than enrolled members can absorb it.
Confirm Month 6 cash: $552,000.
Map member ramp to each hiring step.
Test panel size against physician capacity.
Hold marketing spend to the launch plan.
Track cash weekly until Month 7.
What this estimate hides is the pace of enrollment and the real load on the physician schedule. If growth is slow, the clinic still has to cover facility, admin, payroll, and software costs, so weak ramp control can turn a clean opening into a cash squeeze fast.
Start with licensing, entity setup, malpractice coverage, membership agreements, and a clear patient offer Then set up the Electronic Health Record, telehealth, payment processing, website, and intake workflows In the researched case, Year 1 pricing is $99 individual, $199 family, and $49 small business, with breakeven in Month 7
Plan around a Month 1 to Month 7 launch-to-breakeven ramp The Electronic Health Record setup runs Month 1 to Month 3, telehealth runs Month 1 to Month 2, and medical equipment runs Month 1 to Month 5 The opening can happen earlier, but breakeven is modeled in Month 7
No, the direct primary care model is built around patient membership payments instead of traditional insurance billing You still need clear contracts, payment workflows, compliance review, and patient communication The researched Year 1 mix is 45% individual memberships, 30% family memberships, and 25% small business plans
The usual delays are legal review, membership agreement terms, malpractice coverage, payment setup, portal testing, and slow pre-enrollment Vendor timing matters too: the website and enrollment portal run Month 2 to Month 4, while equipment runs through Month 5 If patient outreach starts late, Month 6 cash pressure rises
Build a waitlist and start pre-enrollment once the membership terms, pricing, and payment process are ready Use local physician relationships, community education, and employer outreach The model assumes a $120,000 Year 1 marketing budget, $85 CAC, and first revenue from individual, family, and small business memberships
About the author
Andrew Brooks
Business Model Writer
Andrew Brooks writes about business model economics and the day-to-day realities of running a new venture for Financial Models Lab. As a business model writer, he helps founders planning a physical location work through startup planning and the money questions that come up before opening, without heavy finance jargon. His work focuses on showing what it really takes to turn an idea into a workable business.
Choosing a selection results in a full page refresh.