How To Open A NICU In A Hospital: 12–24+ Month Launch Plan
To start a neonatal intensive care unit in the United States, assume a hospital-based launch that needs state approval, hospital licensure alignment, neonatal medical leadership, trained nursing coverage, specialized equipment, transfer protocols, payer setup, and referral activation A practical NICU launch timeline is often 12–24+ months, but construction, Certificate of Need review where applicable, and hiring can push that longer In the researched planning model, Year 1 capacity is set at 700%, with 2 neonatologists, 10 NICU nurses, 4 respiratory therapists, 2 developmental specialists, and 1 lactation consultant First revenue starts only after the service is credentialed, contracted, clinically ready, and caring for an eligible neonatal admission
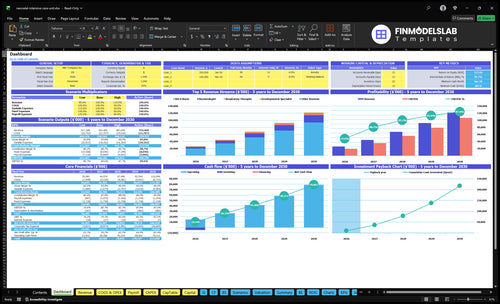
Time to Open12-24 monthsLaunch runwayLaunch Sequence7 stagesApproval firstKey BottleneckStaffing gapProvider coverageFirst Revenue StepEligible admitBilling begins
NICU launch timeline
This is a short web summary of the NICU launch plan, and the XLSX export holds the full Gantt Chart.
Confirm the NICU is safe, licensed, staffed, and billable before go-live
Launch readiness checklist
Use this go-live approval checklist to confirm the NICU is ready before opening.
1Compliance
State licensure approvedCritical
No launch without state approval to operate a neonatal intensive care unit.
Certificate of Need clearedCritical
If your state needs a Certificate of Need, this must be settled first.
CMS enrollment completeCritical
Medicare and Medicaid billing cannot start until enrollment is active.
2Care model
Level-of-care designation confirmedCritical
The unit must match its approved neonatal level of care before opening.
Transfer agreements signedHigh
Clear transfer paths protect babies that need higher or different care.
Hospital policies alignedHigh
Unit rules must match hospital policy on safety, escalation, and consent.
3Unit setup
Incubators and warmers installedCritical
Core bedside gear must be in place before the first infant arrives.
Ventilators and monitors testedCritical
Failed ventilator or monitor tests are a hard stop for go-live.
Backup power and suction testedCritical
Backup power, oxygen, and suction need to work during outages.
4Staffing
Medical director hiredCritical
A named medical director is needed for clinical oversight and escalation.
Neonatologists rosteredCritical
The model assumes 2 neonatologists in Year 1, rising to 6 by Year 5.
NICU nurse roster filledCritical
The unit assumes 10 NICU nurses in Year 1, so gaps will block care.
Respiratory coverage scheduledCritical
Respiratory therapy must cover day, night, and backup shifts.
Support specialists scheduledHigh
Developmental and lactation support should be ready for family care.
5Vendors
Supply contracts confirmedHigh
Medical supplies and pharmaceuticals must be secured before first census.
Diagnostic lab readyHigh
Lab and diagnostic access must be live for sick newborn care.
EHR base license activeCritical
The electronic health record is the base system for orders, notes, and billing.
Billing workflows loadedHigh
Coding rules, claim edits, and charge capture need to be set before launch.
Security access configuredMedium
Patient data and unit access need role-based controls before go-live.
6Revenue
Referral paths activeHigh
Pediatric and obstetric referral flow drives first census after opening.
Payer enrollment completeCritical
Claims will stall if payer setup is missing or incomplete.
Coding rules approvedHigh
Correct coding protects revenue and cuts claim denials from day one.
Financial model validatedHigh
The launch plan should match the Year 1 staffing, cost, and cash setup.
Go-live signoff obtainedCritical
This is the last gate before opening the unit and taking live admissions.
Want the six drivers that decide NICU launch readiness?
1Regulatory Approval
12–24+ mo
Licensing approval is the legal gate; delays here can stop opening even after build-out is done.
2Facility Readiness
$4.5M
Tested equipment, backup power, and infection control cut go-live delays and make first admissions safer.
3Clinical Staffing
2/10/4
Year 1 staffing needs 2 neonatologists, 10 nurses, and 4 respiratory therapists for safe coverage.
4Protocols & Quality
Mock admits
Approved policies, trained staff, and mock admissions reduce handoff errors and improve survey readiness.
5Referral Network
Named partners
Named transfer partners and response standards speed first admissions and prevent failed referrals.
6Payer Readiness
Clean claims
Clean payer setup keeps first admissions collectible and avoids claim denials during ramp.
Why test your NICU launch plan with a financial model before go-live?
The NICU Financial Model Template shows revenue, costs, cash needs, assumptions, and breakeven logic—open it before go-live.
Financial model highlights
Launch timing and census ramp
2 neonatologists, 10 nurses
4 respiratory, 2 specialists
700% capacity, $217M
140% costs, $144k fixed
Cash runway, AR, breakeven
Can you open a standalone NICU?
You usually can’t open a truly standalone NICU in the US like a retail clinic; it is normally a hospital-based service tied to licensure, emergency coverage, obstetrics, pharmacy, lab, imaging, respiratory therapy, infection control, transfers, and payer enrollment. Demand is real, with about 10% of US births preterm, but feasibility depends on hospital sponsorship or a licensed-facility joint venture; see What Is The Current Growth Trajectory Of NICU Bed Occupancy Rates? before sizing beds.
What blocks standalone
State health department approval
Hospital licensure requirements
24/7 emergency coverage
Level IV care standards
Practical launch path
Partner with a licensed hospital
Expand an existing service line
Secure transfer agreements first
Complete payer enrollment early
How long does it take to open a NICU?
Opening a NICU usually takes 12–24+ months, and the schedule slips most from construction, state approvals, Certificate of Need review where required, equipment lead times, neonatologist recruitment, NICU nurse training, payer credentialing, and accreditation readiness. Start with regulatory scoping and service-level selection, then move through design, equipment, staffing, protocols, payer setup, referral activation, mock survey, and go-live. Year 1 model assumes 700% capacity as a ramp assumption, not a day-one promise.
Main delays
12–24+ months is the planning range
Construction can set the pace
State approvals can add months
Equipment lead times can slip launch
Best sequence
Start with regulatory scoping
Choose the service level first
Then hire, train, and credential
Finish with mock survey and go-live
How does a NICU get patients?
A NICU gets patients from the hospital obstetrics unit, maternal-fetal medicine, the emergency department, pediatricians, nearby hospitals, neonatal transport agreements, and regional perinatal networks; see What Is The Estimated Cost To Open And Launch NICU Hospital Unit? for launch costs. First revenue starts only when an eligible newborn is admitted under contracted, billable terms. So payer contracts, credentialed clinicians, billing codes, documentation workflows, and prior authorization rules need to be ready before launch.
Patient sources
Obstetrics sends in-hospital cases
Maternal-fetal medicine handles high-risk referrals
Emergency and pediatricians route urgent babies
Transfers come from nearby hospitals
Ready to bill
Lock payer contracts first
Credential clinicians before opening
Set billing codes and documentation
Build transfer criteria and call coverage
Key Takeaways
Regulatory approval sets the legal launch gate.
Safe equipment and power prevent go-live delays.
Staffing capacity must match acuity before opening.
Billing setup must be clean before first admissions.
Regulatory Approval
NICU Licensing
If the unit does not have written approval for its intended service scope, it cannot open on time or safely admit babies on day one. This includes state health department review, hospital licensure alignment, Certificate of Need where required, CMS participation, accreditation standards, and neonatal level-of-care readiness. No license, no admissions.
The main risk is sequencing. If you finish construction or hire to full coverage before approval lands, you can burn cash while the opening date slips. A lower-acuity launch scope can match approved capacity and let the unit open legally while higher-acuity clearance is still in process.
Approval First
Use qualified legal and regulatory advisors for state-specific filings before you commit to final buildout or staffing. Map each required filing, owner, and due date, then keep the clearance letter, license, and scope limits in one launch file. One clean rule: do not schedule first admissions until the approved scope matches the planned care model.
What this plan needs is simple: the exact license path, the intended level-of-care designation, and proof that the hospital, payer, and accreditation pieces line up. If any step is still pending, keep the launch scope narrow so staffing, equipment, and patient intake stay within what the state has actually cleared.
1
Facility And Equipment Readiness
NICU Equipment Readiness
For a Level IV NICU, the room has to be ready before the first admission, not after. That means incubators, ventilators, monitors, oxygen, suction, isolation space, pharmacy access, lab support, and backup power all need to work together for 24/7 care. If one critical item is late or untested, opening slips and safe first-day care gets smaller fast.
The real risk is buying gear without service coverage, replacement plans, or biomedical sign-off. Tested equipment, validated emergency power, stocked supplies, and signed biomedical checks are the readiness signal. Tie each purchase to a live clinical workflow, so the unit can take the first infant safely instead of sitting on a shopping list.
Test every critical system
Build the opening sequence around the care path: receive infant, stabilize, monitor, isolate if needed, get meds, get labs, and keep power on. That means confirming service contracts, spare parts, lead times, infection control setup, and maintenance ownership before go-live. If the equipment is in the room but not maintained, the launch is still exposed.
Verify all critical devices work.
Validate emergency power under load.
Stock supplies for first admissions.
Sign off biomedical maintenance checks.
Match each item to one workflow.
2
Clinical Staffing
Clinical Staffing
For a NICU, staffing is often the gatekeeper for opening on time. The Year 1 plan assumes 2 neonatologists, 10 NICU nurses, 4 respiratory therapists, 2 developmental specialists, and 1 lactation consultant, plus a medical director, unit manager, billing and reimbursement manager, administrative assistant, and biomedical technician. If 24/7 coverage is not built to match acuity and census, day-one admissions get delayed.
The main launch risk is not headcount on paper; it is whether the team can cover nights, weekends, and higher-acuity shifts without gaps. Neonatologist recruitment and NICU-trained nurse coverage are the usual bottlenecks. Do not build the plan on universal ratios unless state rules, accreditation standards, or hospital policy require them.
Hire to the coverage plan
Start with the roster by shift, not just by title. Verify that each role is credentialed, scheduled, and backed up for sick time and turnover. Document who covers 24/7, who signs off on clinical supervision, and who handles billing, equipment checks, and unit administration before the first admission.
Match staff to planned census.
Fill neonatologist gaps first.
Confirm NICU nurse coverage.
Test night and weekend schedules.
Lock support roles before go-live.
What this plan hides is simple: if staffing lags, cash burn starts before patient volume does. So the launch checklist should prove that every shift can run, not just that resumes are collected.
3
Protocols And Quality Systems
Protocols And Quality Systems
For a Level IV NICU, the unit cannot open safely if core protocols are still draft notes. Before the first admission, the team needs approved rules for admission and transfer criteria, infection prevention, medication safety, feeding, neonatal resuscitation policy, emergency response, family communication, data reporting, and quality review. If those workflows are not live, day-one care gets slower, handoffs get messy, and survey readiness slips.
The real launch risk is treating policies as paperwork instead of operating steps. Readiness shows up when staff are trained, policies are approved, mock admissions are complete, and action items are closed. One clean rule: if the team cannot walk through a transfer, escalation, and documentation path without stopping, the unit is not ready for first admission.
Make the protocols usable, not just written
Build the launch file around the actual first-day workflow. That means mapping who decides admission, who handles transfers, who documents infection checks, who escalates emergencies, and who owns family updates and quality reporting. Keep each policy tied to a named role, a form, and a timing step so staff can follow it under pressure.
Run mock admissions before opening and close every gap before the first patient arrives. If any policy still needs edits, if staff are not trained on the approved version, or if the quality review process is not assigned, opening on time becomes a risk. That usually turns into avoidable rework, delayed first revenue, and weaker compliance on day one.
Approve policies before first admission.
Train every shift on live workflows.
Test handoffs with mock admissions.
Close all action items before launch.
4
Referral And Transfer Network
Referral And Transfer Readiness
A NICU can’t open on time if transfer partners are still informal. Before first beds go live, the unit needs working paths from obstetrics, maternal-fetal medicine, pediatricians, emergency departments, surrounding hospitals, regional perinatal networks, and neonatal transport partners so a baby can be accepted, moved, and admitted without delay.
The launch risk is simple: open beds without aligned referrals, and census stays thin while transfers fail. The readiness signal is a tested process with named contacts, transfer agreements, admission criteria, transport protocols, bed-status communication, physician outreach, and 24/7 call coverage that staff can use on day one.
Test The Transfer Path
Verify each feeder path before opening. Confirm who calls whom, how bed status is shared, and who has authority to accept the patient. Put the contact list, response standard, and escalation path in writing so the first transfer does not depend on memory or one person’s phone.
Run a live drill with one referring hospital and one transport partner. Make sure the team can move from referral to acceptance to arrival without a gap. One clean test beats ten promises.
Confirm named referral contacts.
Document transfer acceptance steps.
Test bed-status updates.
Align call coverage before launch.
Review transport handoff timing.
5
Payer And Revenue-Cycle Readiness
Payer Readiness
If the payer file is not clean, the first NICU admission can turn into a delayed or denied claim. Payer enrollment, Medicaid and commercial contracting, and credentialing have to be done before the first bed is used, because NICU care is billed with DRG or per-diem assumptions that drive cash timing.
The Year 1 model assumes billing and collections fees at 40% of revenue and EHR usage fees at 25%, so 65% of revenue is already spoken for before clinical labor and supplies. If prior authorization, coding, or documentation are weak, accounts receivable (AR) ramps slowly and opening-day cash gets tight.
Load Claims Before Opening
Build the revenue cycle before opening, not after the first transfer. Confirm contracted service terms, load every payer file, and align coding and documentation standards to NICU service lines so the first claim can go out cleanly.
Then test the full path: admit, authorize, code, submit, deny, appeal. One clean run shows whether the team can support day-one volume without billing bottlenecks or claim rework.