What are the biggest mistakes starting oral appliance therapy?
The biggest mistake in Oral Appliance Therapy for Sleep Apnea is launching before the referral path, medical billing, clinical protocol, lab turnaround, and follow-up systems are ready. If diagnosis handoff, prior authorization, front desk scripts, or referral tracking are weak, accepted cases still stall and cancellations rise. The clean test is simple: one patient must move from referral to consult, appliance order, fit visit, adjustment, documentation, and claim submission without a gap.
Common launch misses
Unclear diagnosis handoff
Weak prior authorization process
Untrained front desk scripts
No referral tracking system
Readiness check
Confirm the 6-step patient path
Set adjustment visit dates early
Test vendor turnaround before launch
Slow marketing if onboarding lags
How long does it take to start oral appliance therapy?
Oral Appliance Therapy for Sleep Apnea usually takes 3 to 6 months to start, and the pace depends on payer credentialing, Medicare or durable medical equipment (DME) readiness, physician referral setup, staff training, lab onboarding, and records workflow. Existing dental offices with trained staff and active medical referral links usually move faster. Don’t open the first month until scheduling, insurance intake, lab ordering, fit visits, and follow-ups are all tested.
Main timing drivers
3 to 6 months is the planning range.
Credentialing can slow the start.
Medicare and DME setup matter.
Referral and training add time.
What speeds it up
Existing dental offices launch faster.
Active physician referrals cut delays.
Clear billing avoids handoff gaps.
Test every workflow before opening.
How do you get patients for oral appliance therapy?
Patients for Oral Appliance Therapy for Sleep Apnea usually come from sleep physician, primary care, and ear, nose, and throat referrals, plus screening your own dental patients and people educated about snoring or continuous positive airway pressure (CPAP) intolerance. Keep every claim tied to a confirmed diagnosis and provider coordination; see How To Write A Business Plan For Oral Appliance Therapy For Sleep Apnea? and move each case through screen, document, confirm diagnosis, coordinate the treatment plan, run insurance intake, and schedule the consult. In Year 1, plan on 5% of revenue for digital marketing and physician outreach.
Patient sources
Build sleep physician referrals first
Ask primary care for referrals
Keep ear, nose, and throat links active
Screen existing dental patients for snoring
Conversion workflow
Tie claims to confirmed diagnosis
Coordinate treatment with the referring provider
Run insurance intake before the consult
Use 5% of revenue for outreach
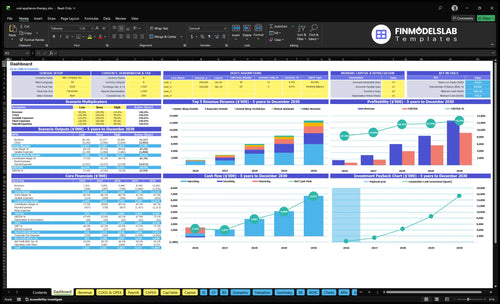
Oral Appliance Therapy for Sleep Apnea Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Validate readiness before accepting oral appliance therapy patients
Launch readiness checklist
Use this go-live approval checklist before opening to confirm the practice is ready to treat sleep apnea and snoring with custom oral devices.
1Compliance
State dental license activeCritical
No patient care should start until the lead dentist is licensed in the launch state.
HIPAA workflows documentedCritical
Protected health data needs a clear intake, storage, and access process before opening.
Informed consent forms approvedCritical
Patients must sign sleep apnea treatment consent before scans, fittings, or delivery.
Sleep study coordination liveHigh
You need a set path for sleep study results before you can confirm treatment eligibility.
2Clinical flow
Scheduling templates loadedHigh
The schedule should separate consults, scans, fittings, and follow-ups so visits do not collide.
Clinical note templates approvedHigh
Notes must capture symptoms, findings, treatment plan, and adjustment steps the same way each time.
Appliance delivery steps testedHigh
Delivery should be repeatable so fit checks and patient instructions are not missed.
Follow-up cadence setHigh
A fixed follow-up plan reduces remakes, confusion, and late problem calls.
3Lab
Lab onboarding completeCritical
The lab must be ready to receive orders before the first patient is scanned or impressed.
Scan and impression path confirmedCritical
You need one clean path for digital scans or impressions so cases move without rework.
Adjustment protocol agreedHigh
A clear adjustment rule set keeps comfort issues from turning into delayed remakes.
4Staffing
Year 1 team staffedCritical
Opening needs the Year 1 mix of 1 senior sleep dentist, 1 technician, 1 assistant, and 1 coordinator.
Role coverage mappedHigh
Each visit step needs a named owner so handoffs do not fail on day one.
Device workflow training completeHigh
Staff must know scan, fit, handoff, and follow-up steps before launch traffic starts.
5Referrals
Physician referral loop liveCritical
Sleep physician referrals are a core demand source, so the handoff has to work on day one.
Primary care outreach list readyHigh
Primary care contacts help fill the top of funnel and reduce dependence on one source.
Patient screening script approvedHigh
A short script helps staff spot likely sleep apnea or snoring cases fast.
6Finance
Pricing matches treatment modelCritical
Year 1 pricing must align with the $3,500 senior dentist rate and the launch case mix.
Billing handoff to claims setCritical
Insurance intake, prior auth, and claim handoff must be clear before the first claim.
Cash runway covers launchCritical
The model shows a $775k minimum cash point in Month 2, so early cash control matters.
Want the six launch drivers that decide opening readiness?
1Clinical Authorization
Gate
A documented diagnosis and consent path keeps first cases billable and avoids stalled starts.
2Referral Network
Source
Tracked referral sources and outreach cadence keep consults flowing while marketing ramps.
3Medical Billing
Cash
Clear intake, prior auth, and claim steps reduce delays and protect early cash collection.
4Appliance Workflow
Lab
An onboarded lab and fit protocol cut remakes and keep delivery visits on schedule.
5Patient Acquisition
Flow
A screened funnel turns patient and physician interest into qualified consults instead of dead-end leads.
6Follow-Up System
Recall
Scheduled adjustments and recall workflows improve case completion and strengthen provider trust.
Clinical Authorization Workflow
Clinical Authorization Workflow
Oral appliance cases cannot start cleanly without a sleep apnea diagnosis and a clear handoff from the sleep physician or other qualified provider. The launch risk is simple: if the chart is missing the sleep study, prescription or treatment plan, consent, medical history, or clinical notes, the case can stall before the first visit and before billing can start.
Set the intake gate before opening. Use one intake criteria sheet, one referral form, one records request path, one consult template, and one case acceptance checklist. That keeps the team from taking patients whose documentation cannot support treatment or payment, which protects day-one flow.
Build the chart gate first
Before launch, verify that every new case can move through the same documented sequence: diagnosis record, treatment order, consent, and clinical notes. If any one step is missing, stop the case and request the file before scheduling production or follow-up. That keeps the opening plan realistic and avoids wasted chair time.
Confirm diagnosis source before intake
Request sleep study records early
Use one consult template
Check consent and medical history
Accept cases only after checklist pass
That process lowers the chance of stalled cases and makes the first revenue cleaner because the chart is ready before treatment starts. The bottleneck to watch is accepting patients too early; once that happens, staff time shifts from care delivery to document chasing.
1
Referral Network
Referral Network
This driver matters because early case volume usually comes from sleep physicians, ear, nose, and throat providers, primary care providers, and existing dental patients. If those referral paths are not active on day one, you may still open on time but have weak consult flow in the first operating month. The main risk is spending on marketing before you have a diagnosis source that can hand off qualified cases.
For this business, the launch goal is steadier consult volume from day one. A working referral network keeps patients moving from screening to consult to treatment instead of stalling while records, notes, or a provider handoff get sorted out.
Build referral paths early
Before opening, build a tracked list of referral sources, set an outreach cadence, and prepare education materials plus the handoff process. Use provider visits, a referral packet, and monthly referral review so you can see which sources are active and which are not.
Screen existing dental patients first.
Track each source and next step.
Set response time standards.
Assign one owner for follow-up.
If referrals are slow, consult volume slows too, so keep the handoff tight and review source activity every month.
2
Medical Billing Readiness
Medical Billing Readiness
Billing has to work before the first patient sits in the chair. For oral appliance therapy, cash can stall fast if insurance intake, prior authorization, documentation, and claim submission are not mapped before launch. The readiness signal is a clear workflow from benefits check to denial follow-up, plus payer credentialing and any Medicare or durable medical equipment steps that apply.
Year 1 assumes 3% of revenue for medical billing and insurance processing fees, so weak setup hits margin and slows collections. If the team takes cases before benefits and authorization rules are clear, patients may get mixed messages, claims can bounce, and first revenue gets pushed back. E0486 may sit in the billing setup, but the real launch risk is process, not coding trivia.
Set Billing Before First Case
Build the flow in this order: intake, benefits check, prior auth, clinical notes, claim file, then denial review. Test it with one sample case before opening so the front desk, clinical team, and billing support all know who does what and when.
Verify payer credentialing is active.
Document prior auth triggers and owners.
Standardize claim and denial follow-up.
Flag Medicare or DME cases early.
Map E0486 only where relevant.
3
Appliance Vendor Workflow
Appliance Lab Workflow
When custom devices are the product, launch timing depends on the lab, not just the chair. Lab turnaround, shipping steps, and remake handling must be set before opening, or first cases will slip and the schedule will look full but not cash-ready. One late remake can block a fit visit and leave a patient waiting.
The readiness signal is simple: an onboarded oral appliance therapy lab vendor, an approved custom workflow, and a clear path for impressions or digital scans, delivery, and adjustments. The Year 1 model assumes 12% lab fabrication fees and 25% impression and sterilization supply costs, so weak vendor terms or slow production timing can squeeze margins fast.
Before You Open
Lock the vendor process before you sell the first case. Confirm device selection, case submission checklist, shipping rules, remake policy, and fit appointment protocol. If production timing is unknown, do not overbook delivery slots. One clean handoff beats a crowded schedule with delayed appliances.
Device selection by case type
Case submission checklist with scans
Delivery template for patient visits
Adjustment schedule for follow-up
Test one full case from scan to delivery before day one. That check shows whether shipping, remake timing, and fit visits fit your calendar and staffing. It also cuts missed appointments and makes case completion smoother from the first month.
4
Patient Acquisition Funnel
Patient Acquisition Funnel
Opening on time depends on getting qualified demand, not just clicks. For oral appliance therapy, the funnel must screen existing dental patients, support local search pages, educate physicians, and route people through a compliant diagnosis workflow. If leads arrive without sleep study records or referral support, they stall before consults and waste launch spend.
The Year 1 plan assumes 5% of revenue for digital marketing and physician outreach, so the early job is to make that spend productive. Build the scripts, landing pages, callback standards, and referral tracking before go-live, or first-day demand will be noisy but not convertible.
Prelaunch Funnel Setup
Set the funnel in this order: existing patient screening, local search pages, physician education, snoring campaigns, CPAP intolerance messaging, consult follow-up, then referral tracking. That sequence matters because each step should move a patient closer to diagnosis-ready intake, not just create interest.
Test the handoff before opening. Every lead should have a clear next step for records, diagnosis confirmation, and case acceptance, with no gap between marketing and clinical review. The main risk is paying for leads that cannot move forward, which slows first revenue and makes the opening feel unsteady.
Confirm scripts before launch.
Publish landing pages early.
Track every referral source.
Standardize callback handling.
Verify diagnosis record intake.
5
Operational Follow-Up System
Day-One Follow-Up System
Oral appliance therapy doesn’t end at delivery, so scheduled delivery, adjustment, titration, provider communication, outcomes tracking, and recall must work on day one. If those steps are not built before opening, delivered cases stall, patient experience slips, and provider trust gets weak fast.
The follow-up load needs 1 dental sleep technician, 1 clinical assistant, and 1 patient care coordinator to keep reminders, documentation, follow-up templates, appliance issue triage, and referral-source updates moving. The bottleneck is treating follow-up as admin instead of core operations, when it is really part of the treatment path.
Map Every Delivered Case
Before opening, load the workflow into the schedule and charting system so every case has a clear path after delivery. Verify reminder timing, documentation fields, follow-up templates, and escalation rules for device issues. One test patient should be enough to show whether the team can handle the full loop without slowing first-day care.
Keep each task owned by one role: reminders, chart notes, adjustment visits, and referral-source updates. That keeps the team from losing cases between delivery and completion, which is where early revenue and patient trust can leak out.
Schedule delivery before first case.
Assign one owner per follow-up task.
Test reminders and chart templates.
Set issue triage response steps.
Review referral updates monthly.
6
Oral Appliance Therapy for Sleep Apnea Business Plan
Start by building the patient path before marketing hard You need a qualified dental provider, diagnosis coordination, appliance vendor setup, medical billing workflow, and follow-up schedule The planning case uses a 3 to 6 month opening window and Year 1 staffing of 1 senior sleep dentist, 1 technician, 1 assistant, and 1 coordinator
Plan for 3 to 6 months if you need referral development, billing setup, and staff training Delays usually come from payer credentialing, Medicare or durable medical equipment readiness where applicable, physician referral handoffs, and appliance lab onboarding Existing dental offices with trained teams can move faster than new standalone launches
Yes, this is a dental clinical service and should be led by appropriately licensed dental providers with dental sleep medicine training The model assumes 1 senior sleep dentist in Year 1, then an associate dentist starting in Year 2 Staff can support intake, records, scanning, scheduling, billing, and follow-up, but clinical responsibility remains with qualified providers
First revenue is delayed when diagnosis records, referral handoffs, insurance intake, or appliance vendor steps are not ready The first paid consultation or appliance case should follow a sleep apnea diagnosis and treatment plan In the Year 1 model, the senior sleep dentist has 40 monthly treatment capacity at 65% utilization
Map one complete case from referral to follow-up before opening Include screening, diagnosis confirmation, consult, insurance intake, appliance order, fit visit, adjustment, claim submission, and provider communication Then test the model using the $3,500 Year 1 senior dentist treatment price and 225% combined variable cost assumptions
About the author
Martin Fletcher
Founder Support Writer
Martin Fletcher is a founder support writer at Financial Models Lab, focused on practical profit planning for founders writing a business plan. He helps small business owners understand how profit works, with clear guidance on startup cost estimates and the numbers to check before money is invested. His writing keeps the focus on useful figures and realistic expectations.
Choosing a selection results in a full page refresh.