Oral Appliance Therapy Startup Costs: $35k Scanner Plus Runway
Oral Appliance Therapy for Sleep Apnea
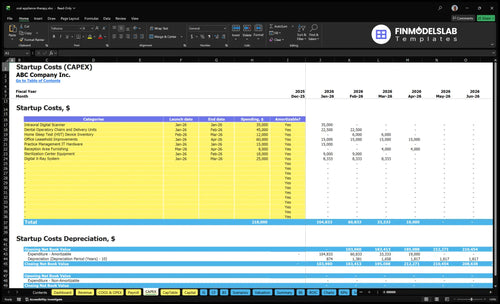
This outline covers $35,000 in known scanner CAPEX, pre-opening expenses, working capital, and first operating year funding needs for an oral appliance therapy practice It separates equipment from launch costs, including $10,600/month in facility and admin overhead and $30,833/month in Year 1 payroll before variable costs
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
This estimates capitalized startup assets only for opening an oral appliance therapy practice.
!
Excluded cash needs This calculator covers capitalized startup assets only. It excludes payroll runway, debt service, working capital, deposits, inventory runway, marketing runway, and operating expenses.
Oral Appliance Therapy for Sleep Apnea Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
What equipment is needed for oral appliance therapy?
For Oral Appliance Therapy for Sleep Apnea, the core startup gear is an intraoral digital scanner or impression setup, bite registration tools, imaging access, sterilization, computers, monitors, secure records hardware, a consultation room, and dental chair access. A digital scanner can cost about $35,000, and many general dental practices already have chairs, sterilization, imaging, computers, and operatory supplies. Keep one-time CAPEX separate from ongoing lab fees and supply costs.
Core startup gear
Intraoral digital scanner or impressions
Bite registration tools
Imaging access or integration
Sterilization setup and supplies
What drives cost
$35,000 scanner figure
Standalone office buildout
Consultation room assets
Ongoing lab fees and supplies
What hidden costs come with starting an oral appliance therapy practice?
If you’re planning How To Write A Business Plan For Oral Appliance Therapy For Sleep Apnea?, the $35,000 scanner is only part of the startup bill. Hidden costs like billing setup, payer credentialing, HIPAA compliance, staff training, physician outreach, and early payroll can push cash needs much higher. Year 1 assumptions also include $1,200/month for malpractice and liability insurance, $600/month for EHR and sleep software, 50% for digital marketing and physician outreach, and 30% for billing and insurance processing.
Startup costs
Medical billing setup costs money
Payer credentialing slows cash inflow
HIPAA compliance adds setup work
Staff training takes paid time
Cash pressure
Referral outreach needs real spend
Website content and local search cost
Early payroll starts before collections
Billing delays raise working capital needs
How much does it cost to add oral appliance therapy to a dental practice?
Adding Oral Appliance Therapy for Sleep Apnea to an existing dental practice can be much cheaper than launching a standalone site because chairs, imaging access, sterilization, staff, lease, and patients may already exist; if the practice lacks a scanner, known CAPEX is $35,000. A standalone researched model starts with $10,600 in first-month fixed facility/admin costs plus about $30,833/month in Year 1 payroll, or $41,433/month for those two known buckets; see How Much Does An Owner Make From Oral Appliance Therapy For Sleep Apnea? for the owner-income side.
Add-on cost
Use existing dental chairs
Use current sterilization workflow
Avoid new lease burden
Add $35,000 if scanner is missing
Standalone cost
Fund facility readiness
Cover $10,600 first-month fixed costs
Plan $30,833/month Year 1 payroll
Build marketing and referrals
Calculate Fuding Needs
Startup cost summary
Startup cost table covering core CAPEX and excluded launch cash needs for an oral appliance sleep apnea practice.
Highlighted CAPEX$183,000Base planning example
Excluded cash needs$775,000Outside CAPEX total
Funding need$958,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Intraoral Digital Scanner
$35,000
3D scanning for treatment planning
Yes
Dental Operatory Chairs and Delivery Units
$45,000
Operatory buildout and patient seating
Yes
Office Leasehold Improvements
$60,000
Suite buildout and clinical finish
Yes
Digital X-Ray System
$25,000
Imaging for diagnosis and monitoring
Yes
Sterilization Center Equipment
$18,000
Infection control and instrument processing
Yes
Opening Cash Buffer
$775,000
Month 2 payroll and overhead runway
No
Oral Appliance Therapy for Sleep Apnea Core Five Startup Costs
Facility, Operatory, And Buildout Startup Expense
Buildout costs
For this practice, one-time facility setup is CAPEX: lease deposit, minor buildout, patient consult rooms, dental chair access, signage, and accessibility work. Use inputs for square feet, lease terms, and contractor scope. Keep this separate from monthly rent and overhead. Add-on launch inside an existing dental office is usually lighter than a standalone clinic buildout.
Monthly burn
The researched monthly facility and admin overhead is $8,800: $6,500 clinical facility rent, $850 utilities and high-speed internet, $450 janitorial and medical waste disposal, and $1,000 general administrative expenses. Here’s the quick math: $8,800 per month before clinical labor and marketing. If some services are shared in an existing office, this burn can drop fast.
$6,500 rent
$850 utilities and internet
$450 janitorial and waste
Launch footprint
A standalone clinic needs more upfront spend because it must cover rooms, chair access, signage, accessibility, and full facility readiness on day one. An add-on launch inside an existing dental office can reuse space and equipment, so the real job is checking what is already live: power, internet, waste pickup, and patient flow. The lease drives the model.
Reuse chair access when possible
Verify accessibility before opening
Confirm waste pickup early
Readiness check
Budget the buildout as a separate line from monthly overhead, then test readiness before first patient day. If signage, internet, janitorial service, or medical waste pickup is late, opening slips and cash burn starts before revenue does. That’s why the pre-opening checklist matters more than the paint color.
Clinical Equipment And Technology Startup Expense
What counts
Tangible assets belong in CAPEX: scanner or impression systems, bite registration tools, imaging integration, sterilization equipment if needed, computers, monitors, secure records hardware, dental chair access, and other clinical setup items. A known CAPEX source is $35,000 for an intraoral digital scanner. Monthly software is operating expense, not CAPEX.
How to size it
Here’s the quick math: count the units you need, multiply by unit price, then add a contingency input for launch risk. Existing dental offices may already own chairs, sterilization equipment, imaging, and computers, so their startup CAPEX can be lower. Standalone practices usually need more assets funded upfront.
List owned assets first
Price missing items by unit
Keep software out of CAPEX
Reduce upfront spend
Buy only what the first launch cases need, then phase the rest as volume grows. The cleanest savings come from using existing dental chair access, imaging, and computers instead of buying duplicates. Don’t bury monthly software or service fees in equipment. That keeps the asset budget honest and makes payback easier to track.
Reuse existing clinic assets
Phase nonessential purchases
Track software separately
Budget guardrails
Use the scanner line item as the anchor and build the rest from what the office already owns. If the practice is standalone, expect a larger upfront cash need for imaging, sterilization, computers, and secure records hardware. Keep a contingency input in the model, but don’t treat it like a quote.
Lab Workflow And Clinical Supplies Startup Expense
Supply stack
Initial lab workflow supplies cover bite registration materials, impression supplies, sterilization packs, appliance cases, cleaning instructions, patient education sheets, and shipping labels. The first order should match expected cases, not annual volume, so the key inputs are units, par level, and lab turnaround time.
Budget math
Custom lab fabrication is usually a variable cost, not CAPEX. Using the stated Year 1 assumptions, 120% lab fees plus 25% clinical impression and sterilization supplies equals 145% of revenue. On $118,500 monthly revenue, that is $171,825/month.
Keep it lean
Buy starter kits in small batches, set reorder points, and get clear lab turn times and shipping rules. The savings come from avoiding dead stock, rush freight, and remake fees. Don’t overbuy cases or print stacks of education packets before case flow is steady.
Match stock to monthly cases
Standardize shipping and labeling
Track remake and rush costs
Cash before cases
Before the first steady cases land, the launch budget still needs cash for the first supply orders. Treat that as working capital, not CAPEX, because it moves with case volume and timing.
Software, Billing, And Compliance Startup Expense
Software Setup
Budget this as two layers: pre-opening setup and monthly run cost. The setup work covers practice management integration, EHR and sleep software, payer enrollment, HIPAA compliance, documentation workflows, and secure records. After launch, plan $600/month for software plus 30% of Year 1 revenue for billing and insurance processing fees.
What It Covers
This line item also covers claims support and reporting, plus any one-time implementation work before the first patient is billed. Size it with vendor setup fees, number of users, and months of subscription coverage. If payer setup slips, cash gets tied up before claims start paying.
Count setup fees once
Count monthly seats separately
Track payer enrollment timing
Keep It Lean
Avoid buying separate tools that do the same job. Use one system for documentation, records, and billing where possible, and delay extras until volume justifies them. The safe cut is duplication, not compliance. Skip HIPAA controls or claims support, and the savings can turn into denials.
Drop duplicate modules first
Review claims denials weekly
Train staff on one workflow
Cash Lag
Reimbursement timing matters. Even if demand is strong, claims may pay after the appliance is delivered, so working capital needs can rise before cash comes back. Build the budget for that lag, especially in the first months when billing volume is growing.
Training, Insurance, And Referral Launch Startup Expense
Launch Setup
This cost covers clinician education, team training, legal and accounting setup, professional liability review, website content, local SEO, and sleep physician referral work. Treat it as pre-opening expense, not CAPEX. Rules for credentials vary by state, payer, and role, so size the budget around a staffed Year 1 team: 1 lead dentist, 1 registered dental assistant, 1 office manager, and 0.5 FTE billing support.
Estimate Inputs
Start with months of coverage and launch timing. Use $1,200/month for malpractice and liability insurance, then add the months before claims and referrals run cleanly. For growth, plan 50% of Year 1 digital marketing and physician outreach here. Website copy and local SEO belong in this bucket because they drive referrals, not assets.
Keep It Tight
Use one onboarding plan, one claims workflow, and one referral script. The common mistake is spending on outreach before the office can document, code, and submit clean claims. If payer setup or staff training slips, hold back extra ad spend until the team can answer calls, book consults, and process claims without rework.
Referral Readiness
Put the budget against referral volume and claim quality. If the team cannot turn sleep physician leads into scheduled consults and clean claims, extra marketing just burns cash. The real output is a ready front end: trained staff, insured coverage, clear documentation, and a site message that matches the referral channel.
Compare 3 Startup Cost Scenarios
Scenario Table
Lean works when the dental office already has rooms, staff, and patients, so startup spend stays low. Base adds the scanner and launch stack, while Full adds buildout and a bigger payroll load.
Lean, Base, and Full launch cost comparison
Scenario
Lean LaunchExisting-office add-on
Base LaunchDedicated sleep line
Full LaunchStandalone clinic
Launch model
Add sleep apnea fitting to an existing dental office using shared rooms, shared staff, and an in-house patient base.
Run a dedicated sleep service line inside an existing practice with its own scanner, billing setup, and referral push.
Open a standalone clinic with its own facility, full team, and dedicated sleep-apnea workflow.
Typical setup
Use current chairs, sterilization, lease, and admin systems, then add a small device-fitting workflow.
Add the $35,000 scanner, software, supplies, training, and a tighter insurance workflow.
Fund buildout, equipment, and a full Year 1 payroll base, plus fixed overhead.
Cost drivers
chair access
sterilization
existing staff
lease already in place
referral flow
scanner purchase
software and billing setup
supplies and training
referral launch
insurance processing
facility leasehold
operatory buildout
full payroll
equipment and inventory
overhead run rate
Planning rangeCAPEX only
$10,000 - $25,000Lowest spend
$50,000 - $100,000Mid spend
$450,000 - $750,000Highest funding
Best fit
Best for an owner-dentist who wants to test demand with low new spend and already has chair time and staff.
Best for practices ready to build a real sleep line and absorb a mid-sized setup spend.
Best for operators with enough capital to launch a new clinic and support slower payback.
!
Planning note: These ranges are researched planning assumptions for scenario modeling, not exact quotes or vendor bids.
Oral Appliance Therapy for Sleep Apnea Business Plan
Plan beyond the $35,000 scanner because payroll and overhead start fast The researched Year 1 model carries about $30,833/month in payroll and $10,600/month in fixed facility and admin costs A one-month runway is about $76,433 before unlisted buildout, training, deposits, supplies, and owner draw
Payer and billing setup can affect cash before steady collections arrive The model includes medical billing and insurance processing at 30% of Year 1 revenue, plus an insurance billing specialist at 05 FTE If claims setup or documentation workflows lag, the practice needs more working capital even when patients are scheduled
Not always An existing dental office may already have chairs, sterilization, imaging access, computers, and patient flow The major known equipment line in this plan is a $35,000 intraoral digital scanner If you already own suitable scanning or impression systems, your add-on funding need may shift toward training, billing setup, supplies, and referral outreach
The researched Year 1 plan starts with 1 lead dentist, 1 registered dental assistant, 1 office manager, and 05 FTE insurance billing specialist That equals about $30,833/month in payroll The associate sleep dentist starts in Year 2, so the first year depends heavily on the lead dentist and a tight billing workflow
The researched Year 1 monthly revenue capacity is about $118,500 at modeled utilization Here’s the quick math: the senior sleep dentist contributes 40 treatments/month at $3,500 and 650% capacity, or $91,000/month Technician, assistant, and coordinator services add modeled revenue, while Year 1 variable costs total 225% of revenue
About the author
Lucas Hart
Local Business Observer
Lucas Hart writes for Financial Models Lab as a local business observer focused on simple cash flow planning for people turning a service idea into a business. He explains business costs in plain language and shares startup budget examples to help readers make practical decisions before launch.
Choosing a selection results in a full page refresh.