Start a Palliative Care Practice: 4–9 Month Launch Plan
To open a palliative care practice, define the service model, form the entity, verify state healthcare rules, secure malpractice coverage, hire licensed clinicians, set up the EMR and billing workflow, credential with payers, and build referral channels A practical palliative care launch timeline is often 4–9 months, mainly because payer credentialing, staffing, and referral readiness can move at different speeds The researched planning assumptions start Year 1 at 65% capacity with 2 physicians, 3 nurse practitioners, 2 social workers, 1 chaplain, and 1 bereavement counselor First revenue starts when a referral becomes a completed, documented, billable care encounter
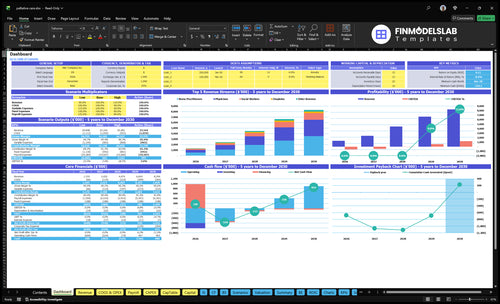
Time to Open6 monthsSetup windowLaunch Sequence6 stagesCompliance firstKey BottleneckPayer gateApproval pathFirst Revenue StepBillable consultReferral to visit
Launch timeline
This is a short web summary of the launch plan, and the XLSX export contains the detailed Gantt chart.
What are the biggest palliative care startup mistakes?
The biggest palliative care startup mistakes are launching before payer credentialing is done, hiring clinicians too late, and blurring palliative care with hospice. If intake, consent, symptom assessment, care plans, family communication, and billing docs are not tested, problems show up fast; plan Year 1 at 65% capacity, not full utilization. Readiness beats speed.
Common launch mistakes
Start before credentialing clears.
Hire clinicians too late.
Underestimate documentation load.
Use an unclear service scope.
What to test first
Check compliance and staffing.
Test EMR and billing.
Build referral pathways.
Review first-patient onboarding.
How long does it take to start palliative care?
A practical Palliative Care launch usually takes 4–9 months, but payer credentialing can push first billable revenue out even when the clinical team is ready. Hiring physicians and nurse practitioners is the other big timing risk, and EMR setup, billing workflows, documentation templates, referral agreements, and state compliance should all run at the same time. The first month should not assume full schedules; the Year 1 model assumes 65% capacity.
What slows launch
Payer credentialing delays revenue
Hiring physicians takes time
Hiring NPs takes time
Compliance reviews run in parallel
What to do first
Start payer enrollment early
Build billing workflows first
Test EMR before opening
Set referral outreach before broad intake
How do you get palliative care referrals?
Palliative Care referrals usually come from trusted clinical relationships, not broad ads. Start with 9 partner types—hospitals, discharge planners, oncology groups, cardiology practices, nephrology practices, primary care clinics, skilled nursing facilities, assisted living communities, and senior living operators—and lead with patient fit, symptom burden, family support, and care coordination; if you’re also mapping launch costs, see How Much Does It Cost To Open And Launch Your Palliative Care Business?
Build referral trust
Lead with patient fit.
Explain symptom burden.
Show family support.
Clarify hospice differences.
Track billable flow
Count referral source.
Count accepted cases.
Count completed encounters.
Review payer status and follow-ups.
Key Takeaways
Choose one care model before hiring or systems setup.
Compliance gaps can block care, billing, and referrals.
Hire to launch capacity, not vanity headcount.
Credentialing and intake must work before first referral.
Clinical Care Model
Clinical Care Model
If the care model is not set before hiring or systems setup, the launch will slip. Clinic-based, home-based, telehealth-supported, facility-contracted, and hybrid models each change staffing, scheduling, transport, billing, and compliance checks, so trying to serve every setting from day one usually slows first visits and creates bad handoffs.
The readiness signal is a written scope that names eligible patients, visit types, symptom assessment flow, care-plan ownership, family communication, and escalation rules. That scope keeps referrals clean and first-patient onboarding safer because the team knows what it will do, what it will not do, and when to hand off.
Lock the care scope early
Pick one launch model before you buy software or assign staff. Then test the path from referral to visit to note to follow-up for that one setting, so your schedule, travel plan, and documentation match the real workflow.
Define eligible patients first.
Set visit types and escalation rules.
Assign care-plan ownership now.
Write family update steps clearly.
If the model cannot fit on one page, referral partners will send the wrong patients and day-one operations will get messy.
1
Compliance and Licensing Readiness
Compliance and Licensing
If this piece is weak, you may not be able to see patients, bill, or sign referral agreements on day one. For palliative care, the launch gate is state licensure, scope of practice, HIPAA, consent, documentation, malpractice coverage, and care-plan rules, not just staffing.
The main trap is assuming palliative care follows hospice rules or standard primary care workflows. That can break care delivery fast. A realistic budget includes $2,000 per month for malpractice insurance and $1,000 per month for a legal and compliance retainer, or $3,000 per month before you even count clinical labor.
Lock the checklist before opening
Build the compliance file before scheduling the first visit. Verify clinician licenses by state, define who can order or sign what, and make sure consent forms, note templates, privacy rules, and escalation paths match the care model. One clean launch signal is a completed compliance checklist reviewed by qualified advisors.
Here’s the quick math: if any required approval slips, opening slips too. So sequence the work in this order: licensure, malpractice, HIPAA and consent, documentation, then referral and billing sign-off. What this setup hides is delay risk from carrier review, advisor review, and policy edits, so bake that time into the launch calendar.
Confirm state-by-state clinician authority.
Document care-plan ownership rules.
Test note-to-claim workflow.
Store consent and privacy forms.
Review coverage with qualified advisors.
2
Staffing and Clinical Team
Launch-Ready Clinical Coverage
Staffing has to match day-one capacity, not a wish list. If the 2 physicians and 3 nurse practitioners are late, the clinic can’t safely open, because consults, follow-ups, and medical director oversight all depend on licensed coverage. The Year 1 core team also includes 2 social workers, 1 chaplain, and 1 bereavement counselor, so the launch is really a full care model, not just medical visits.
Here’s the quick math: the listed salaries for the physicians, nurse practitioners, and social workers total $920,000 per year before chaplain and bereavement pay. The readiness signal is coverage for consults, symptom follow-up, social needs, spiritual support, bereavement support, care coordination, and oversight. If hiring slips, you get unsafe overbooking or delayed starts, and both hurt first-patient experience.
Hire to the Opening Schedule
Sequence the clinical hires before referrals start. Lock the physician and nurse practitioner start dates first, then fill social work, chaplain, and bereavement support around the first consult calendar. Verify active licenses, scope of practice, and supervision rules before assigning visits. If one key clinician is missing, reduce launch capacity instead of stretching the team.
Use a simple go-live check: can the team cover consults, follow-ups, family calls, and escalations on the planned launch week? If not, delay opening or narrow the service area. That keeps access controlled, protects clinical quality, and avoids the common trap of promising more patients than the team can safely see.
Confirm physician start dates first.
Match schedules to licensed coverage.
Test consult and follow-up workflows.
Assign oversight before first referral.
3
Payer Credentialing and Billing
Payer Credentialing and Billing Setup
Payer enrollment and provider credentialing decide when this practice can bill, not just when it can see patients. If clinicians start visits before enrollment, documentation rules, and coding workflows are ready, the first consults can turn into unpaid work and slow opening cash.
The launch path should connect referral → completed note → clean claim. That means EMR billing build, claim submission testing, denial tracking, and payer mix review are in place before opening. With Year 1 billing software fees at 20% of revenue, weak claim flow can eat early margin fast.
Test the Clean Claim Path
Build and test the billing chain before the first patient is scheduled. The goal is a working handoff from intake to coding to submission, with the right documentation tied to each visit type. One clean test claim is worth more than ten open slots.
Enroll payers first
Credential each provider
Set coding rules in EMR
Define note-to-claim checks
Track denials from day one
If claims fail, cash lags even when consult volume looks strong. The bottleneck is usually not care delivery; it is seeing patients before the billing file, documentation rules, and payer approvals are aligned.
4
Referral Network Development
Referral Network Development
The first patients will not come from broad ads. They will come from trust and fit, so the referral network must be built before opening month. For palliative care, that means hospitals, discharge planners, oncology, cardiology, nephrology, primary care, skilled nursing facilities, assisted living communities, and senior living operators already know who to send, why to send them, and how to hand them off.
Year 1 marketing and patient acquisition is modeled at 30% of revenue, so weak referral conversion can drain cash fast. A generic ad plan is the bottleneck risk here. The launch is ready when there is a named referral list, clear patient-fit criteria, education materials, a handoff process, and a feedback loop that tells you which sources are actually producing completed consults.
Build referrals before first day
Start with a short list of high-fit sources and document exactly what each one needs to see before sending a patient. Here’s the quick math: if referrals are not converting, you still pay the marketing load, but completed consult volume stays uneven. One clean referral path is more useful than a wide but vague outreach plan.
List named contacts by source.
Send patient-fit criteria in writing.
Standardize handoffs and follow-up.
Track source-to-consult conversion.
Use the feedback loop to spot who sends the right cases, who needs more education, and where delays happen. If the handoff is unclear, patients stall before the first consult, and day-one volume gets patchy.
5
Patient Intake and Care Coordination
Intake and Care Coordination
Palliative care can’t open on time unless referrals move from receipt to a complete plan without gaps. The day-one risk is not demand; it’s whether each visit produces eligibility review, consent, symptom assessment, and a note that supports billing.
The setup also needs the EMR and telehealth stack live before the first referral. With an EMR subscription at $1,500 per month and a telehealth platform at $800 per month, software runs at $2,300 per month. If intake is weak, scheduling slips, care-plan documentation gets missed, and claims slow down.
Test the referral-to-claim path first
Run one test referral end to end before opening. The path should cover referral receipt, eligibility review, consent, medication and goals review, family communication, scheduling, care-plan documentation, follow-up reminders, and billing documentation.
Load intake templates in the EMR.
Test telehealth access before launch.
Assign one owner for chart completion.
Use a claim-ready documentation checklist.
What matters is a clean handoff, not speed. If documentation slips during an emotional visit, staff may still deliver care, but claims can stall and the team will spend time fixing charts instead of seeing patients. A clean test referral is the readiness signal; if it fails, fix the workflow before opening.