Palliative Care Startup Costs: $205K CAPEX Plus Runway
The cost to start a palliative care business in this model starts with $205,000 in identified CAPEX before working capital A practical palliative care startup cost estimate also needs runway because Year 1 payroll is $115,000 per month and fixed overhead is $15,700 per month Using only payroll and fixed overhead, 3 to 6 months of runway equals about $392,100 to $784,200 These are researched planning assumptions, not vendor quotes, reimbursement guarantees, or universal startup costs
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates capitalized startup assets only for a palliative care launch, before any contingency.
!
Excluded Costs Base CAPEX is $205,000 before contingency. This calculator covers capitalized startup assets only. It excludes inventory, payroll runway, rent deposits treated as pre-opening expense, debt service, working capital, marketing spend, credentialing delays, payer collection delays, operating losses, and other non-CAPEX funding needs.
Calculate Fuding Needs
Startup cost summary
Startup cost breakdown for palliative care, covering buildout, clinical technology, equipment, furniture, telehealth setup, and payroll runway reserve.
Highlighted CAPEX$205,000Base planning example
Excluded cash needs$522,800Outside CAPEX total
Funding need$727,800CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Office Leasehold Improvements
$75,000
Office buildout and leasehold work
Yes
Initial Medical Equipment
$40,000
Clinical equipment volume and spec level
Yes
EHR, HIPAA, and IT Setup
$50,000
Software buildout, licensing, and hardware scope
Yes
Office Furniture & Fixtures
$25,000
Workspace size and furnishing count
Yes
Telehealth Platform Setup
$15,000
Remote visit setup and configuration effort
Yes
Payroll Runway Reserve
$522,800
Monthly payroll of 115000 plus 15700 overhead, delayed payer collections, and startup billing lag
No
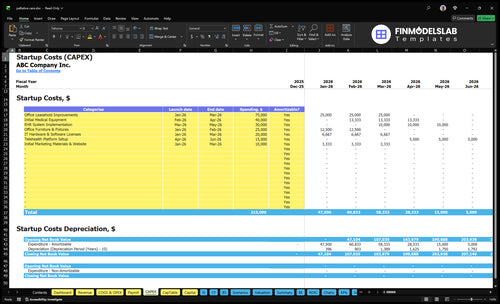
Does the CAPEX tab show launch costs?
The screenshot shows the financial model tab's startup CAPEX by category, timing, amount, and depreciation/amortization in Palliative Care Financial Model Template; review assumptions.
Key screenshot checks
Month 1-6 timing
$205,000 CAPEX total
Vendor, payer, clinician checks
Compare 3 Startup Cost Scenarios
Startup cost scenarios
Staffing drives most of the spend in palliative care, so scenario scale matters. Lean delays space buildout, base follows the model, and full assumes a faster clinician ramp.
Lean, base, and full palliative care launch cost bands.
Scenario
Lean LaunchLowest buildout
Base LaunchModel case
Full LaunchHigh ramp
Launch model
Run a smaller home-based or outpatient coordination start with deferred facility spend.
Follow the modeled hybrid or outpatient setup at about $109,200 in monthly revenue and 65% Year 1 capacity.
Start closer to later-year staffing levels so the team can cover more volume sooner.
Typical setup
Use core clinicians, a small office, and only the systems needed to start care coordination.
Use the modeled interdisciplinary team, standard office overhead, and the full EHR and telehealth stack.
Use a larger team and broader admin support, with more room for higher visit volume.
Cost drivers
Deferred leasehold improvements
reduced furniture
core clinical staffing
basic systems
Modeled CAPEX
3-6 months payroll
fixed overhead
EHR and telehealth
Later-year FTE ramp
higher payroll
larger admin load
more clinical coverage
Planning rangeCAPEX only
$392,100 - $497,100Lower cash need
$597,100 - $989,200Modeled funding
$1.44M - $2.98MHigh cash need
Best fit
Founders testing demand with tight cash and a lighter facility footprint.
Operators who want the clearest read on staffing, overhead, and break-even timing.
Teams that need broader coverage and can fund a faster ramp.
!
Planning note: These ranges are researched planning assumptions built from the model's CAPEX, payroll, and overhead inputs, not exact quotes or guaranteed budgets.
What hidden costs come with starting a palliative care business?
The biggest hidden costs in Palliative Care are usually working capital items, not buildout. Malpractice insurance at $2,000/month, legal and compliance at $1,000, the EHR at $1,500, and telehealth at $800 add up to $5,300/month before payroll, and payer enrollment delays plus referral development can push cash needs well past the $205,000 CAPEX budget; for owner pay context, see How Much Does The Owner Of Palliative Care Business Typically Earn?
Main hidden costs
Payer enrollment delays slow cash
Referral development takes time
Malpractice coverage is recurring
HIPAA and workflow setup cost cash
What to fund first
$5,300 monthly fixed base
Payroll during early ramp-up
Cash before collections stabilize
Extra funding beyond $205,000
What drives palliative care staffing costs?
Clinical staffing readiness is the biggest cost driver in Palliative Care, because the service only works when a licensed team is in place and billable. Here’s the quick math: Year 1 salary load is about $1.425 million from 2 physicians at $200,000 each, 3 nurse practitioners at $120,000 each, 2 social workers at $80,000 each, plus the chaplain, bereavement counselor, clinical director, operations manager, and billing/admin coordinator; ongoing payroll alone runs $115,000 per month.
Pre-opening recruiting, onboarding, training, credentialing, and payroll hit before revenue starts, so cash needs rise fast. The real risk is not just headcount, it’s paying for licensed capacity before patient volume ramps.
Year 1 staffing load
2 physicians = $400,000
3 nurse practitioners = $360,000
2 social workers = $160,000
Support roles add $505,000
Cash pressure points
$115,000 monthly payroll run-rate
$1.38 million annual payroll run-rate
Recruiting comes before billing
Credentialing delays cash flow
How should startup costs feed into a palliative care financial model?
For Palliative Care, startup costs should set launch timing, runway, and the staffing ramp first, then feed the payer mix and break-even math. Put the known $205,000 of CAPEX across Months 1 to 6, then test Year 1 capacity at 650% against about $109,200 in monthly revenue from 2 physicians, 3 nurse practitioners, 2 social workers, 1 chaplain, and 1 bereavement counselor. That revenue has to sit next to $115,000 payroll, $15,700 fixed overhead, and revenue-linked COGS, so this is a planning step after cost estimation, not the main pitch.
Startup cost uses
Spread $205,000 over 6 months
Match spend to launch timing
Build runway from cash outflow
Delay hires until demand supports them
Model checks
Test $109,200 monthly revenue
Compare against $115,000 payroll
Add $15,700 fixed overhead
Include revenue-linked COGS and variable costs
Key Takeaways
State rules drive licensing, compliance, and enrollment costs.
Year 1 staffing opens with 115 FTE and $115k payroll.
Buildout splits one-time office and tech CAPEX from rent.
Launch burn adds insurance, supplies, transport, and marketing.
Palliative Care Core Five Startup Costs
Licensing And Compliance Startup Expense
License Scope
There isn’t one national license for every palliative care launch. Budget for entity formation, healthcare attorney review, state rules, payer enrollment support, and Medicare and Medicaid checks where needed. The sourced legal and compliance retainer is $1,000 per month from Month 1 to Month 60.
Pre-Open Costs
Classify attorney setup, payer enrollment support, and compliance documentation as pre-opening expenses unless you capitalize them. The main inputs are state, care model, payer strategy, clinician credentialing, and whether the practice bills directly.
State rules change filing work
Direct billing adds enrollment steps
Credentialing adds time and cost
Control Spend
Keep spend tight by using state-specific checklists, reusing policies only after local review, and drafting consent forms and referral agreements after the payer plan is set. Don’t skip compliance work to save a few weeks; that usually costs more later.
Budget Drivers
The legal load rises when you expand into more states, add direct billing, or need heavier clinician credentialing. If the model stays referral-based with limited payer work, the setup is lighter; once it bills payers, compliance becomes a real launch gate.
Insurance, Supplies, And Referral Launch Startup Expense
Launch coverage
For a palliative care launch, the model starts with $2,000 a month for medical malpractice insurance. Add policy review, payer enrollment help, consent forms, and referral agreements before opening unless a cost is clearly capitalized. The main drivers are state rules, care model, payer mix, clinician credentialing, and direct billing.
Supply base
Clinical and medical supplies run at 20% of Year 1 revenue, and the model shows about $2,184 a month, plus $500 for general office supplies. Estimate it from visit volume, per-patient supply use, vendor quotes, and months of opening stock. One clean rule: don’t buy a big shelf of items until referral flow is real.
Travel and outreach
Transportation is modeled at 30% of Year 1 revenue, or about $3,276 a month, and marketing and patient acquisition are also 30%, or about $3,276 a month. Build this from mileage, visit density, referral outreach, education materials, and launch campaigns. If routes are scattered, travel burn rises fast.
Launch control
Treat insurance premiums, supplies, education materials, referral outreach, and launch marketing as pre-opening or operating launch expenses unless they’re clearly capitalized. Keep a separate launch budget, tie spend to signed referral talks, and track monthly burn against first-patient volume. The mistake is funding growth spend before care capacity and payer setup are ready.
EHR, Telehealth, And HIPAA Technology Startup Expense
Core tech stack
This startup cost covers the systems that run visits, charts, secure messages, billing, and telehealth. The main build is $30,000 for EHR implementation, $20,000 for IT hardware and software licenses, and $15,000 for telehealth setup, so you keep one-time launch cash separate from monthly run costs.
What it buys
The buildout should include secure messaging, billing integration, laptops, tablets, phones, cybersecurity, telehealth workflows, and documentation standards. Estimate it from vendor quotes, device counts, and setup hours. That keeps the launch budget tied to real inputs, not guesswork.
Count users and devices first
Quote setup and license fees
Map charting and payer needs
Recurring run rate
After launch, plan on $1,500 a month for the EHR subscription and $800 for telehealth. Billing software fees add 20% of Year 1 revenue, so fixed software costs stay steady while transaction fees rise with volume.
Fixed tech run rate is $2,300 monthly
Variable fees scale with revenue
Check contract terms before signing
Launch control
Buy only the devices and licenses you need at go-live, then add seats as referrals build. The common mistake is mixing implementation with subscriptions or ignoring billing fees in margin math. If onboarding slips, you still pay the monthly tech stack before visits start.
Office And Care Coordination Startup Expense
Upfront buildout
$75,000 of leasehold improvements plus $25,000 of furniture and fixtures puts the base space cost at $100,000 before deposits or utility setup. For palliative care, this should cover care coordination workstations, accessibility needs, and signage. Count these as capital spending, not monthly overhead, and keep the scope smaller if the model is mostly home-based or partner-facility led.
Monthly space cost
$8,000 rent, $1,200 utilities, and $500 general office supplies total $9,700 per month, or $116,400 a year. Here’s the quick math: rent is the big fixed cost, while utilities and supplies are smaller but steady. Treat them as operating or pre-opening expenses, not buildout.
Rent drives the run rate.
Utilities need setup cash.
Supplies stay modest.
Keep it lean
If you’re mostly home-based or using partner sites, don’t copy a full clinic buildout. Use the $100,000 space budget only when the office truly needs patient-facing rooms, accessibility changes, and dedicated coordination desks. A smaller suite, shared clinical space, or phased furniture buy can cut waste without hurting care quality.
Start with the minimum usable footprint.
Delay nonessential finishes.
Buy furniture in phases.
Budget order
Put deposits, utility setup, and compliance-ready workspace items in pre-opening cash needs, then keep rent and utilities in the monthly operating plan. If opening volume is still uncertain, delay oversized buildout and sign shorter leases first. That keeps cash tied to the care launch, not empty square footage.
Clinical Staffing Readiness Startup Expense
Staffing Build
Here’s the quick math: the source model opens with 115 FTE across clinicians, clinical leadership, operations, and billing admin, and monthly Year 1 payroll is $115,000. That is a full interdisciplinary team, so staffing is not a small add-on cost. It belongs in the startup budget from day one, not just in the monthly run rate.
Pre-Open Payroll
Pre-opening payroll can get large fast if clinicians start before referral volume or payer approvals. Budget for recruiting, onboarding, background checks, credentialing time, training, care protocols, documentation workflows, and team meetings. One clean rule: don’t hire every role at once unless launch dates and payer timing are already locked.
Count weeks before first billable visit
Budget credentialing delays separately
Track payroll before revenue starts
Phased Hiring
To manage this cost, stage hires against referral flow and payer approvals, then add coverage only when demand is real. That protects cash without lowering care quality. A startup does not need a hospital-sized team on day one, but this source model does assume a full team at launch, so the staffing plan must match that ambition.
Hire in waves, not all at once
Use start dates to control cash burn
Keep the first schedule tight
Payroll Gate
If clinicians are on payroll before patients are flowing, staffing becomes a startup expense instead of a steady operating cost. With $115,000 a month in payroll, even a short delay in referrals or payer approval can strain cash, so tie headcount to launch milestones and keep onboarding dates flexible.