How to Open a Radiology Center: 9–18 Month Launch Plan
You’re opening a regulated imaging facility, so the launch path runs through modality scope, site fit, equipment, compliance, staffing, payer setup, and referrals This guide covers a 9–18 month opening process and a five-year planning model with Year 1 capacity starting at 25%–40% by service Your next step is to lock the service mix, then test whether staffing, systems, and referral volume support opening month readiness
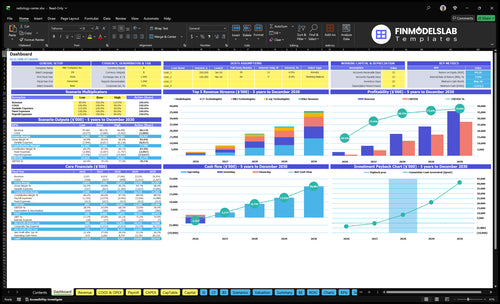
Time to Open12 monthsLaunch runwayLaunch Sequence8 stagesScope firstKey BottleneckEquipment delayLead timeFirst Revenue StepScheduled scansOrders live
Launch timeline
This is a short web summary of the launch plan; the XLSX export has the full Gantt Chart.
What are common mistakes opening a radiology center?
Common mistakes opening a Radiology Center are picking a modality mix the site can’t support, underestimating payer credentialing, opening before referrals are lined up, and letting RIS/PACS, billing, staffing, and equipment acceptance testing slip. If you model Year 1 wrong, the center still needs $119,450 per month in fixed overhead and payroll covered, and with 86% contribution after modeled variable costs, breakeven is about $138,895 per month.
Common launch misses
Match modalities to site demand
Start payer credentialing early
Build referrals before go-live
Test RIS/PACS and billing first
Go-live gate checks
Block launch until compliance passes
Hire before the first scan date
Complete equipment acceptance testing
Model ramp friction, denials, downtime
What licenses are needed to open a radiology center?
A Radiology Center needs approvals for the facility, radiation equipment, staff licensing, safety workflows, occupancy, and payer enrollment before it can scan patients; treat this as a launch dependency, not legal advice. For a center built around 3 imaging lines and a 24-hour report goal, check What Is The Most Critical Metric To Measure The Success Of Radiology Center? early because Medicare and commercial payer files can affect the first $1 of reimbursed revenue.
Opening approvals
Check state facility rules
Register radiation-producing equipment
Secure permits and occupancy approval
Verify physician and technologist licenses
Revenue readiness
Submit Medicare and payer files
Assess American College of Radiology accreditation
Build HIPAA privacy and security workflows
Add MQSA certification for mammography
How long does it take to open a radiology center?
A Radiology Center usually takes 9–18 months to open, starting with modality scope and site approval, then buildout, shielding, equipment delivery, installation, inspections, accreditation, staffing, payer enrollment, and referral development. MRI and CT often push the timeline longer because room specs, power, shielding, calibration, physicist testing, and acceptance testing all have to line up. If payer credentialing lags, scans can be physically ready but still not reimbursed, and if referral outreach starts after installation, the first month can feel quiet.
Choose site and modality mix before signing the lease.
Compliance gaps can block scans and reimbursement.
Equipment, staffing, and testing control opening dates.
Referral and payer readiness drive first-month revenue.
Modality Scope and Site Fit
Modality Site Fit
Before you sign, decide whether the site can handle X-ray, CT, MRI, or ultrasound. The wrong layout can stall opening because these rooms need the right power, shielding, equipment access, patient flow, and parking. If the site cannot support MRI or CT room specs, you can end up redesigning after lease signing, which pushes day-one service back.
For planning, tie the site to Year 1 volume assumptions: MRI at 25% capacity, CT at 30%, and X-ray at 40%. That keeps the room plan realistic and helps the opening month schedule stay clean. This work also depends on vendor specs and state radiation rules, so the site has to pass both the layout review and the compliance check.
Check Site Fit Before Lease Sign
Start with a modality mix and room spec sheet, then review shielding, landlord approvals, intake flow, and parking before you commit. One clean sentence: if the room cannot support the machine, the lease is too early.
Verify vendor power and space specs.
Confirm state radiation requirements.
Map patient flow from entry to scan.
Review parking and referral access.
Get landlord approval in writing.
What delays launch is simple: a late room change, a failed shielding plan, or a CT/MRI fit issue that forces rework after construction starts. That can slow opening month scheduling and add cost before the first scan.
1
Compliance and Accreditation Path
Compliance and Accreditation Path
Compliance and accreditation can block scanning, reimbursement, or both. For a radiology center, the launch risk is not just paperwork; it is whether state rules, radiation registration, HIPAA workflows, safety roles, and payer approval are done before the first patient is booked. If those files lag, the site can be built but still not ready to bill.
This path depends on equipment type, ownership structure, payer strategy, and the services offered. MRI and CT usually trigger more modality-specific obligations than X-ray, so the approval stack has to match the exact service mix. If accreditation or payer files arrive after install, you can lose dead weeks between physical readiness and reimbursed scans.
File the approval stack first
Start with a compliance tracker and assign one radiation safety lead. Map state radiation registration, safety roles, HIPAA processes, and modality rules, then document protocols and staff training before opening. Build Medicare and commercial payer requirements in parallel so billing can start as soon as scanning does. That protects the first revenue ramp, which is modeled at about $251,725 per month.
Confirm state registration timing.
Match files to each modality.
Document protocols before go-live.
Test payer workflows early.
Keep the launch date tied to the slowest approval, not the fastest vendor promise. If the paperwork is not done, the center may still carry rent, payroll, and equipment costs while the scanners sit ready but unused.
2
Equipment Procurement and Installation
Equipment Install Readiness
Equipment procurement and installation is the date lock for a radiology center. Delivery, room prep, shielding, calibration, service contracts, physicist testing, and acceptance testing have to land in order, or the opening slips even if the lease is signed and staff are hired. A signed equipment schedule tied to buildout milestones is the real readiness signal.
The biggest risk is MRI and CT, because room specs, power, shielding approval, and testing are less forgiving. If utilities or IT integration run late, you can open with payroll in place but no scanner ready, which creates idle weeks and pushes first scans out. One clean handoff beats a rushed launch.
Lock the Install Sequence
Before opening, lock the install sequence in writing: vendor selection, room design, delivery route review, installation plan, quality testing, and downtime coverage. Keep the installer, physicist, IT team, and buildout crew on the same calendar so the room is ready when the equipment arrives.
Verify lease and utility dates.
Confirm shielding approval timing.
Test image system links early.
Assign downtime coverage now.
Do a dry run before go-live: route a case through delivery, install, calibration, and acceptance testing, then record who signs off at each step. If any approval is missing, the first scan date is still a guess.
3
Staffing and Clinical Coverage
Licensed Coverage First
Staffing decides whether the center can open on time and run from day one. The launch plan needs live coverage for 1 radiologist, 2 MRI technologists, 2 CT technologists, 2 X-ray technologists, 1 radiology nurse, and 1 practice manager, plus front desk and billing coverage. If licensure, credential checks, or modality skills lag, the scanners may be ready but the schedule will not be.
Here’s the quick math: that roster is built to support 25%–40% Year 1 utilization. That only works if interpretation, nursing, reporting, and patient flow are covered at the same time. The key dependency is payer credentialing and accreditation files; if those land late, you can have staffed rooms but still miss reimbursed scans and first revenue.
Lock the Day-One Roster
Map each role to a shift before opening, then verify licenses, privileges, and modality competencies in writing. One missing MRI or CT technologist can cut scan capacity fast, and one missing radiologist can slow report turnaround. Keep a backup plan for absences, especially for high-demand shifts and first-week ramp.
Do the work in this order: hire, verify credentials, train on safety, assign schedules, then test backup coverage. Use an opening checklist tied to front desk, billing, nursing, and management handoffs. If equipment arrives before staff are cleared, the site burns time and payroll without reaching full clinical output.
Confirm licenses before scheduling
Test modality competencies early
Document backup coverage by shift
Match staffing to equipment go-live
4
RIS/PACS/Billing Workflow
RIS/PACS and Billing Go-Live
This workflow is the bridge from scan to cash. RIS (radiology information system) handles scheduling and orders, PACS (picture archiving and communication system) stores images and supports viewing, and billing turns the completed study into a claim. If any handoff fails, the center can open on time and still miss revenue on day one.
Readiness means a successful test from referral intake through claim submission, not just software access. That includes scheduling templates, prior authorization, radiologist reporting, patient notices, billing rules, denial tracking, and HIPAA security. If payer rules or referring physician access are late, first-week scans can stack up unpaid and slow cash from the start.
Test the Full Order-to-Cash Path
Run sample orders for every modality before opening. Verify that a referral becomes a scheduled exam, an authorized exam, a stored image set, a signed report, a sent notice, and a clean claim. One clean loop matters more than a long checklist because it proves the center can bill on day one.
Assign one owner for RIS, PACS, billing.
Confirm payer rules before go-live.
Test denial tracking and claim edits.
Document physician access and report delivery.
Watch the weak spot: untested integration. If the system works in pieces but not end to end, staff will miss orders, rework claims, and chase fixes after patients are already scheduled. Fixing denial rules in test mode is faster than fixing them after the first scan is done.
5
Payer Contracts and Referral Pipeline
Payer Access and Referrals
Payer participation, authorized orders, and referral flow decide whether the center can bill on day one. If Medicare enrollment, commercial payer files, and authorization workflows are not ready, you can open with scanners live but no reimbursable patients. That creates dead weeks, weak cash collection, and unhappy referring doctors.
Readiness means payer files submitted, authorization workflows tested, and outside doctors ready to send orders into scheduling. For a radiology center targeting $251,725 in modeled Year 1 monthly revenue, the ramp depends on how fast referrals convert into scheduled scans, not just whether the equipment is installed.
Lock the Referral Path Before Opening
Build the launch sequence around billing and referral access, not around the machine arrival date. Verify accreditation, radiologist credentials, facility details, and billing setup before payer outreach. Then test one real order from intake to authorization to scheduling so you know the workflow works. If that loop breaks, first-day volume will not match the plan.
Map Medicare enrollment timing.
Send commercial payer packets early.
Create a short referral packet.
Visit local specialists in person.
Set urgent care referral contacts.
Confirm scheduling access for partners.
One clean rule: no payer file, no predictable cash. If referral sources are not trained and able to place orders, the center can open on time and still miss early revenue.