How To Open A Sports Medicine Clinic In 6 To 12 Months
To open a sports medicine clinic, you typically need a licensed provider structure, compliant outpatient space, malpractice coverage, an electronic health record system, clinical equipment, trained staff, payer credentialing, and referral relationships before opening A practical launch timeline is often 6 to 12 months, but licensing, leasehold improvements, and insurance credentialing can push the opening date The researched planning assumptions show Year 1 monthly treatment capacity of about 834 visits across the clinical team before ramp risk First revenue usually comes from referral partners, local athletes, teams, and self-pay injury evaluations booked into the opening schedule
Time to Open6-12 monthsOpening prepLaunch Sequence6 stagesCompliance firstKey BottleneckCredentialing gatePayer delaysFirst Revenue StepPaid evalBooking live
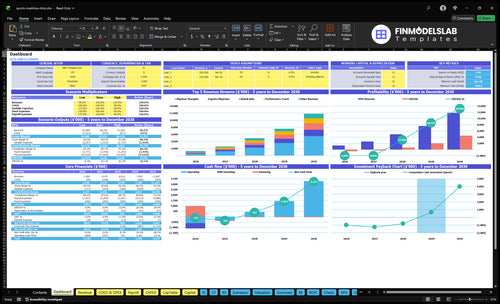
Launch timeline
Short web summary of the launch plan; the XLSX export includes the detailed Gantt Chart.
How long does it take to open a sports medicine clinic?
A Sports Medicine Clinic usually takes 6 to 12 months to open. The real opening date depends on payer credentialing, leasehold improvements, equipment delivery, inspections, provider onboarding, and billing setup. The sequence matters more than the calendar, and Month 1 lease and fixed overhead start burning cash before revenue.
Do not book an opening-week schedule until licensed staff, malpractice coverage, electronic health record, eligibility checks, claim submission, and referral intake all work in test mode.
What drives timing
6 to 12 months is the practical range
Credentialing can slow launch
Inspections can push dates back
Equipment delivery can delay setup
What must work first
Licensed staff must be in place
Malpractice coverage must be active
EHR and billing must be tested
Claims and referrals must run cleanly
How do you get patients for a sports medicine clinic?
Your first patients come from referral relationships built before launch, not from broad ads. Start with orthopedic groups, primary care practices, schools, athletic clubs, gyms, coaches, physical therapists, employers, and local sports organizations, and turn each conversation into booked evaluations; for startup context, see How Much Does It Cost To Open A Sports Medicine Clinic?. First revenue should come from injury evaluations, rehab visits, diagnostics, and performance sessions.
Build referrals
Meet orthopedic groups before launch.
Ask for booked evaluations.
Use local sports organizations.
Track each source by appointment.
Price the first visits
$130 physical therapy visits.
$280 sports physician visits.
$160 performance coaching.
$450 diagnostics.
What launch mistakes create readiness risk for a sports medicine clinic?
A Sports Medicine Clinic is not ready when marketing is ready; it’s ready when payer setup, referral flow, billing, clinical protocols, staffing, emergency steps, and scheduling all work on day one. If onboarding takes 14+ days after hire, capacity can look open but fail operationally. Use a go/no-go checklist and test eligibility, consent, claims, denial handling, vendors, and opening-week handoffs before you take bookings.
Launch risks
Open only after payer setup works
Test referral pipeline before launch
Validate billing and denial handling
Confirm emergency coverage and schedules
Go-live checks
Check insurance eligibility first
Review consent and documentation templates
Verify supply vendors and handoffs
Train staff before first appointments
Key Takeaways
Licensing and supervision must clear before opening day.
Credentialing and test claims protect launch cash flow.
Location, buildout, and equipment must support patient flow.
Named referral sources drive opening-week appointment volume.
Provider Licensing And Clinical Governance
Provider Licensing First
Licensing and clinical governance are the first gate. A sports medicine clinic cannot open on time if the sports physician, physical therapists, performance coach, rehab aide, and diagnostic specialist scopes are not set under state rules. The medical director or supervising physician, malpractice insurance, and written protocols need to be locked before hiring or marketing. No scope, no opening.
The biggest risk is state-specific scope and supervision rules. If a rehab aide needs direct oversight, or a diagnostic specialist cannot perform a task in your model, opening week becomes a compliance problem instead of a care launch. The readiness signal is simple: every provider cleared to treat, document, bill, and escalate care.
Lock Scope Before You Schedule
Map each service to one licensed role, then write the supervision rule next to it. The Year 1 staffing plan includes 4 physical therapists, 1 sports physician, 1 performance coach, 2 rehab aides, and 1 diagnostic specialist, so each job needs a clear scope before onboarding. Use written protocols to test triage, charting, billing, and escalation before the first patient books.
Confirm state scope rules first.
Set supervision in writing.
Bind malpractice coverage before visits.
Approve service protocols by role.
Test documentation and escalation flow.
If the supervising physician terms, insurance, or role limits are still open, do not market services yet. A clinic can look staffed and still be unready if no one is cleared for their exact work. The launch target is a clean handoff from intake to care with no scope gap on day one.
1
Payer Credentialing And Billing Readiness
Payer Credentialing
If you want to open on time, this is the gatekeeper. Without commercial insurance, Medicare where applicable, and workers’ compensation setup, you may be able to see patients but not bill cleanly, which turns day one into a cash squeeze and slows collections.
This also covers self-pay policies, coding workflows, eligibility checks, claim submission, and revenue cycle testing. The model’s 50 percent Year 1 referral fee or commission assumption needs a compliance check first, because medical referral payments can be restricted.
Test Billing Before Opening
Before launch, verify payer IDs, fee schedules, and who is enrolled under each contract. Then run clean test claims, test front-desk collections scripts, and confirm staff know what to say when insurance is pending or out of network.
One missed setup item can delay cash by weeks. A simple readiness check is: every payer loaded, every code path mapped, and every first-visit workflow tested from check-in to claim submission.
Confirm payer enrollment status.
Test eligibility at check-in.
Validate claim edits and denial rules.
Train staff on self-pay collection.
2
Clinic Location And Buildout
Clinic Location And Buildout
Location drives day-one revenue here. A sports medicine clinic needs parking, easy access, ADA-compliant entry, exam rooms, rehab space, clear signage, and a clean flow from check-in to evaluation to rehab to checkout. If the layout creates dead zones or bottlenecks, patients feel it immediately and staff lose time.
The cash risk is real: the model carries a $15,000 monthly lease from Month 1, so every delay burns rent before the first visit. The main failure point is delayed inspections or an unfinished treatment area, because that can push opening back even when hiring and scheduling are ready.
Lock The Floor Plan
Walk the site like a patient. Start at parking, then check entry, reception, exam rooms, rehab space, and checkout. The space is ready only when a patient can move through the full visit path with no dead zones and no pinched handoffs between medical care and rehab.
Before signing off, verify lease terms, signage, inspection timing, and the buildout schedule. Keep a punch list for anything that blocks opening, especially treatment rooms and access routes. If inspections slip, the opening date slips too, and the lease clock keeps running.
Confirm parking and entry access.
Test ADA access end to end.
Map exam and rehab flow.
Track inspections and punch-list items.
Open only when treatment space is finished.
3
Equipment, Systems, And Workflow
Equipment And EHR Readiness
This launch driver decides whether the clinic can see patients on day one. It covers exam tables, rehab and mobility gear, taping and bracing supplies, diagnostic tools, consent forms, documentation templates, scheduling, billing software, vendor setup, and the EHR (electronic health record). The modeled EHR license is $1,500 per month, so that cash has to be funded before the first visit.
The test is a mock patient visit from scheduling through charting and billing. If a table, template, or software step is missing, providers slow down in opening week, notes back up, and claims can miss the first billing cycle. No workflow, no clean launch.
Rehearse First Visit
Load the templates, forms, and charge rules before patients book. Then run one full visit with front desk, provider, and billing so you can catch weak handoffs, missing fields, and vendor delays while there is still time to fix them.
Confirm delivery dates for all equipment.
Test scheduling to billing end to end.
Upload consent forms and visit templates.
Assign a backup for delayed vendors.
If equipment arrives late or templates need rework, the clinic opens with less room, slower charting, and a weaker patient experience. That can also delay claims and push cash out later than planned.
4
Staffing And Scheduling Coverage
Match Staffing to Visit Capacity
For a sports medicine clinic, staffing has to match the service mix before opening day. The Year 1 model uses 4 physical therapists, 1 sports physician, 1 performance coach, 2 rehab aides, and 1 diagnostic specialist. With capacity assumptions from 600% for diagnostics to 750% for rehab aides, the schedule must be real or the clinic opens with paper capacity and front-desk bottlenecks.
If call coverage, visit slots, or provider handoffs are thin, day-one patients wait longer, visits get rushed, and booked volume falls below plan. The launch effect should be fewer missed calls, cleaner visits, and realistic appointment capacity, not an overbooked calendar that breaks on the first busy morning.
Test Coverage Before Open
Build the schedule around a mock week, not just an org chart. Train front desk, billing support, scheduling coverage, role handoffs, and provider escalation before the first patient arrives, then test a simulated call, check-in, eval, rehab visit, and billing close. That shows whether the team can handle real flow without missing calls or stacking delays.
Map each role to exact hours.
Backfill lunch, breaks, and no-shows.
Write handoff rules for each visit type.
Confirm who escalates clinical issues.
What this setup hides is simple: if one role is uncovered, the whole day slows down. A weak schedule can turn ready rooms into idle time, late starts, and unhappy athletes, even when the providers are licensed and the equipment is ready.
5
Referral And Patient Acquisition Pipeline
Referral Pipeline Before Opening
This clinic can be clinically ready and still miss launch if referrals are weak. With modeled Year 1 volume at about 834 monthly visits, you need a real source pipeline before day one: schools, clubs, gyms, coaches, orthopedic providers, primary care practices, employers, and local sports events. The readiness signal is simple: opening-week appointments tied to named sources, not vague interest or social reach.
Book Evaluations, Not Likes
Track booked evaluations, referral source, and show rate before opening. That tells you whether demand is real and whether the front desk can fill the calendar from day one. If bookings come in without source names, you can’t tell which partners are working, and you can’t fix the pipeline fast enough.