Healthcare Real Estate Development Startup Costs: $928M Project CAPEX
Key Takeaways
Land control can swing upfront cash needs sharply.
Soft costs rise with zoning, permits, and legal work.
Construction is the biggest cost, at $685M total.
Reserves matter; cash trough hits month 20.
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates capitalized startup assets only for a healthcare real estate development, not operating cash or payroll runway.
!
What this leaves out This calculator covers capitalized startup assets only. It excludes payroll runway, working capital, debt service, deposits, inventory, marketing, post-opening operating expenses, and tenant medical equipment.
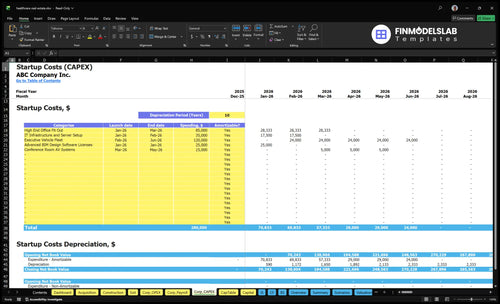
What does the Healthcare Real Estate Development CAPEX screenshot show?
What drives healthcare real estate development costs?
Healthcare Real Estate Development costs are driven less by the shell and more by MEP systems, HVAC, plumbing, electrical, fire and life safety, elevators, parking, accessibility, medical-use layouts, entitlement complexity, and tenant improvement allowances. In modeled budgets, a $30M Dialysis Wing is far below a $180M Surgery Block, and build times run from 10 to 22 months, so longer projects raise carry risk. Keep landlord base building separate from tenant clinical buildout, and treat staffing and clinical equipment as separate unless the developer is delivering a turnkey healthcare facility.
Main cost drivers
MEP systems add heavy cost.
HVAC drives clinical build budgets.
Fire and life safety add scope.
Accessibility and parking add expense.
Scope split
Base building is not clinic fit-out.
Tenant improvements are separate cost lines.
Provider staffing stays off the build budget.
Clinical equipment stays separate unless turnkey.
How much capital do you need to start healthcare real estate development?
You don’t need one magic number; you need separate capital for the developer-company setup and for each funded project. For Healthcare Real Estate Development, the researched 7-property plan shows $280k launch CAPEX, $243M acquisition cost, and $685M construction budget; see How Much Does An Owner Make In Healthcare Real Estate Development? for the owner-income side.
Capital Stack
$280k company launch CAPEX
$243M total acquisition cost
$685M total construction budget
7-property researched development plan
Timing Risk
First ASC Center: Month 3
First acquisition cost: $25M
Construction starts: Month 5
Cash trough: $21.749M, Month 20
What hidden costs should healthcare real estate developers plan for?
If you’re planning Healthcare Real Estate Development, the hidden costs are mostly soft costs and timing costs: due diligence overruns, title work, surveys, environmental review, land-use counsel, lender fees, appraisals, legal, insurance, property taxes, interest carry, lease-up marketing, broker commissions, tenant coordination, contingency, and reserves. For a clean starting point, see How Do I Write A Healthcare Real Estate Development Business Plan? and keep these items separate from vertical construction CAPEX. Budget year one with 40% for sales commissions and brokerage, 25% for project legal and compliance, and $283k in monthly fixed overhead; the Month 20 cash trough shows timing can sink a deal before the sale closes.
Plan the soft costs
Due diligence overruns hit early.
Title, surveys, and environmental review add fees.
Legal, lender, and appraisal costs stack fast.
Use contingency and reserves for delays.
Protect cash timing
Lease-up marketing and broker commissions are variable.
Tenant coordination can push cash out.
Property taxes and interest carry keep running.
Keep salaried team costs outside CAPEX.
Calculate Fuding Needs
Startup cost summary
This table covers property buys, build costs, launch assets, and non-CAPEX cash needs for a healthcare real estate developer.
Fixed overhead, salaries, and post-opening cash trough
No
Healthcare Real Estate Development Core Five Startup Costs
Land and Site Control Startup Expense
Land Cost
Seven owned sites means $0 rental cost but $243M in purchase cash. The model includes examples like a $12M Dialysis Wing, $25M ASC Center, $42M Medical Hub, $55M Health Plaza, and $60M Surgery Block. Owned, leased, optioned, or contributed land changes the upfront cash need fast.
Site Control Costs
Purchase price is only part of site control. Add deposits, option agreements, broker fees, title work, surveys, environmental review, and site due diligence. To estimate it, use parcel count, quoted price, deposit terms, and third-party report fees. One line item can hide a lot of cash before design or construction starts.
Count every parcel.
Price each closing.
Quote all reports.
Cash Need
Owned land pushes cash out early; leased, optioned, or contributed land lowers that check size. Refine the estimate by parcel condition, zoning status, healthcare demand, and tenant precommitment. A clean, entitled site with committed users needs less cash at closing than a raw parcel that still needs approvals.
Upfront Plan
Start with the site-control path that matches the project: buy outright when timing is tight, use options when zoning or demand is still being tested, and keep title, survey, and environmental work in the budget either way. The real question is not just price; it’s how much cash you must commit before the parcel is ready to build.
Pre-Development, Entitlement, Design, and Permitting Startup Expense
Soft Costs
Pre-development, entitlement, design, and permitting are soft costs, not dirt or concrete. Budget for architects, civil engineers, MEP design, land-use counsel, zoning approvals, site plans, building permits, code review, and healthcare-specific standards. State and local rules vary, and certificate-of-need is not universal. Keep these costs separate from hard construction so the cash plan stays clean.
What It Covers
This line item covers the work needed before boots hit the site: drawing sets, engineering studies, permit filings, hearings, and compliance review. For planning, tie the budget to the number of months between acquisition and start of construction. Here, an ASC Center was acquired in Month 3 and construction started in Month 5, so soft-cost carry matters.
Architectural drawings and revisions
Engineering and permit fees
Healthcare code review and filings
How to Manage It
Control this spend by locking scope early, sequencing entitlements before full design, and using local counsel only where the jurisdiction needs it. A clean way to model it is as a variable project legal and compliance cost at 25% in Year 1, then stepping down over the model. That keeps soft costs visible without mixing them into hard construction.
Use local code checks first
Limit redesign loops
Track soft costs by project
Timing and Compliance
Don’t treat entitlement timing as fixed. If zoning, site plan approval, or permit review slips, the gap between acquisition and construction gets longer, and carry rises. Healthcare facilities often need stricter design review than standard commercial projects, so the budget should hold enough time and cash for redraws, hearing delays, and permit corrections.
Medical Facility Construction and Buildout Startup Expense
Scope
Medical buildout covers shell construction, tenant improvements, exam-room layouts, MEP systems, HVAC, plumbing, electrical, fire and life safety, elevators, and infection-control-ready finishes. In the seven owned-project model, total construction budget is $685M, with examples from a $30M Dialysis Wing to a $180M Surgery Block.
Estimate
Price it in layers: landlord base building versus tenant-specific clinical buildout. Use square feet, room counts, and vendor bids for HVAC, plumbing, electrical, and life safety. The buildout runs 10 to 22 months, so interest carry and cash reserves must cover the full draw period, not just hard costs.
Control
Keep the shell separate from the clinical fit-out, then lock room templates early. That lowers redesign and change orders without hurting compliance. The big mistake is underfunding carry on long jobs; a 22-month schedule needs more reserve than a 10-month one. Bid infection-control finishes and elevators up front, not after the permit set.
Cash Timing
The cash need is driven by draw timing, not just the headline budget. Longer builds stretch lender fees, interest during construction, and reserves, so a project with a 22-month schedule can tie up far more cash than a similar 10-month job. Plan financing around the slowest permit and construction path.
Site Work, Parking, Access, and Infrastructure Startup Expense
Access Cost
This is not generic commercial site work. It covers grading, drainage, utilities, stormwater, roads, sidewalks, patient drop-off, ambulance access, signage, parking, and ADA paths. Cost swings with parcel condition, local code, and facility type, and imaging, surgery, dialysis, and outpatient sites often need heavier utility and access planning.
Budget Inputs
Estimate it from utility capacity, ingress and egress, parking demand, stormwater limits, and civil quotes. Keep it inside project CAPEX when it is part of land development or construction scope. In this model, seven owned properties carry $243M of land purchase cost and $0 rental cost, so site work sits on top of acquisition and build-out cash.
Get utility letters first.
Price off civil drawings.
Test parking to code.
Cut Rework
Save money by checking access early and designing to the parcel, not a template. The big trap is assuming a flat lot and simple parking count; that can miss off-site road work, stormwater detention, or utility upgrades. For surgery and dialysis, a bad site can add cost and delay before the first permit is even filed.
Price the worst access case.
Match layout to patient flow.
Challenge every off-site add-on.
Due Diligence
Before closing, ask for utility capacity, easements, curb-cut rules, parking ratio limits, stormwater detention rules, and ADA route requirements. On a deal that closes in Month 3 and starts construction in Month 5, there is no room for redesign. If patient flow or ambulance access fails, the site cost becomes a schedule and carry-cost issue.
Financing, Carrying Costs, Contingency, and Lease-Up Startup Expense
Carry Costs
Keep lender fees, interest during construction, insurance, property taxes, appraisal, legal, lease-up marketing, broker commissions, tenant coordination, reserves, and contingency outside vertical construction. These are soft costs, not build costs. If you blur the lines, you hide the cash peak and understate the funding need.
Cost Inputs
Build this line from months of carry, loan size, fee quotes, and the lease-up plan. Modeled sales commissions and brokerage run 40% in Year 1 and Year 2, then 35%, 30%, and 30%. Project legal and compliance runs 25% in Year 1, then 20%, 15%, 12%, and 10%.
Use lender term sheet fees.
Price interest by month.
Quote broker and legal rates.
Reserve Discipline
The cash trough of $21749M in Month 20 says the reserve has to be in place before Month 21 breakeven. That reserve should cover carry, taxes, insurance, and lease-up spend, plus contingency. If tenant coordination slips, the reserve is what keeps the project alive.
Lease-Up Control
Lower this cost by locking tenant timing early, tightening broker scopes, and matching marketing spend to signed demand. Keep legal, compliance, and lease-up as separate soft-cost lines so you can see which delay is burning cash.
Compare 3 Startup Cost Scenarios
Startup cost scenarios
Startup cost swings hard with site size, buildout scope, and timing. A smaller medical property plan costs far less than a full campus, and funding needs rise with each added project.
Lean, Base, and Full launch paths for healthcare property development.
Scenario
Lean LaunchSmall site plan
Base LaunchBalanced rollout
Full LaunchLarge campus build
Launch model
Starts with a Dialysis Wing or Specialty Clinic and keeps the first phase tight.
Starts with an ASC Center or Medical Hub and builds a mid-scale platform.
Starts with a Health Plaza or Surgery Block and pushes into a full campus model.
Typical setup
Uses one smaller owned asset, lighter buildout, and a narrow project team.
Combines owned acquisition, full project management, and standard medical buildout.
Uses a larger owned site, heavier construction, and a bigger team to manage delivery.
Cost drivers
Site control
smaller acquisition
limited construction
compliance work
lean staffing
Land acquisition
medical buildout
project team
legal and compliance
sales commissions
Large acquisition
heavy construction
specialty fit-out
higher staffing
funding carry
Planning rangeCAPEX only
$42,000,000 - $63,000,000Lower capital
$105,000,000 - $167,000,000Mid-scale budget
$205,000,000 - $240,000,000High capital
Best fit
Fits founders testing site control and smaller medical property deals first.
Fits operators who want a repeatable launch with room to add assets over time.
Fits sponsors with strong backing who can fund a larger multi-year development plan.
!
Planning note: These scenario ranges are researched planning assumptions, not exact quotes or guaranteed project bids.