 Time to Open6-12 monthsLaunch runway
Time to Open6-12 monthsLaunch runwayHow To Open A Cardiac Resynchronization Therapy Service In 6–12 Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Time to Open6-12 monthsLaunch runway  Launch Sequence6 stagesClinical lead
Launch Sequence6 stagesClinical lead Key BottleneckCredentialing gateLab access
Key BottleneckCredentialing gateLab access First Revenue StepCRT implantsAuth cleared
First Revenue StepCRT implantsAuth cleared


Key Takeaways
- Credentialed physicians are the launch gate, not a detail.
- Lab readiness drives safety, scheduling, and case capacity.
- Payer setup comes before scheduling eligible patients.
- Follow-up capacity protects safety and referral trust.
Time to Open6-12 monthsLaunch runwayLaunch Sequence6 stagesClinical leadKey BottleneckCredentialing gateLab accessFirst Revenue StepCRT implantsAuth clearedLaunch timeline
Short web summary of the launch plan; the XLSX export includes the detailed Gantt Chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8Month 9Month 10Month 11Month 12
Licensing compliance
- Gap review
- Policy draft
- License filings
- Compliance audit
Facility and lab
- Space design
- Fit-out work
- Lab install
- Sterile workflow
- Emergency drill
Physician credentialing
- Privilege packets
- CV review
- Hospital approval
- Coverage roster
Payer enrollment
- Payer list
- Enrollment forms
- Auth rules
- Billing setup
Staffing and devices
- Key hires
- Device vendor
- Team training
- Device interrogation
- Remote enrollment
Referrals and go-live
- Referral outreach
- Intake screening
- Scheduling block
- Follow-up visits
- Go-live drill
- First cases
Why test the Cardiac Resynchronization Therapy Services model before launch?
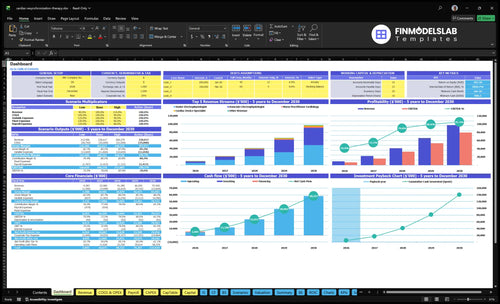
The screenshot shows revenue, costs, cash needs, assumptions, and break-even logic for Cardiac Resynchronization Therapy Services Financial Model Template. Open the model.
Key model checks
- Launch timing and payer delays
- $781,950 Year 1 revenue
- Staffing grows 7 to 34
- 12% kits, 5% fees
- Break-even and runway path
How do CRT services get patients and first revenue?
CRT services usually get first patients through clinical referrals, not ads, and the best sources are heart failure cardiologists, general cardiologists, primary care physicians, hospitals, discharge planners, device clinics, and payer-approved pathways. First revenue starts with a referred heart failure consult, then eligibility review, documentation, payer authorization, implant scheduling, and post-implant follow-up. For the launch plan, Year 1 capacity is modeled at 15 monthly treatments for the senior electrophysiologist and 12 for the associate before utilization adjustment; if you want the planning flow in business-plan form, see How To Write A Business Plan For Cardiac Resynchronization Therapy Services?.
Where patients come from
- Heart failure cardiologists send referrals first
- General cardiologists are core referral sources
- Primary care physicians can spot candidates
- Hospitals and device clinics drive handoffs
How first revenue starts
- Start with a referred heart failure consult
- Move to eligibility review and documentation
- Get payer authorization before scheduling
- Use targeted outreach at 3% of Year 1 revenue
Year 1 launch focus
- Keep outreach relationship-driven
- Use payer-approved pathways early
- Build post-implant follow-up quickly
- Target utilization before scale
Year 2 growth shift
- Raise outreach to 25% of revenue
- Keep referral ties active
- Watch consult-to-implant conversion
- Expand only after workflow holds
What is the biggest mistake opening CRT services?
The biggest mistake in Cardiac Resynchronization Therapy Services is opening before payer authorization, device inventory, trained staff, and post-implant monitoring all work together. A scheduled implant can still fail if approval is missing, the right lead kit is not on hand, or the device rep is not coordinated. And with Year 1 remote monitoring set at 200 monthly encounters per technician at 60% capacity, follow-up is a day-one capacity issue, not an afterthought.
Test before first implant
- Dry-run referral intake.
- Confirm prior authorization.
- Match lead kits to cases.
- Coordinate the device rep.
Verify care after implant
- Test sterile workflow.
- Check recovery handoff.
- Set device interrogation steps.
- Enroll remote monitoring on day one.
What do you need to open a CRT service?
To open Cardiac Resynchronization Therapy Services, you need credentialed electrophysiology leadership, facility privileges, licensed care operations, payer enrollment, vendor setup, trained staff, and written safety workflows; use How To Write A Business Plan For Cardiac Resynchronization Therapy Services? to map these into a launch plan. First revenue starts only when referred eligible patients get payer authorization before implant scheduling.
Launch must-haves
- Credentialed senior electrophysiologist leadership
- Facility privileges and licensed care operations
- Medicare and commercial payer enrollment
- Device vendor setup and handling controls
Year 1 checklist
- 7 roles: 1 senior, 1 associate electrophysiologist
- 2 device specialists, 2 nurse practitioners
- 1 remote monitoring technician
- Confirm rules with counsel, payers, administrators
Validate CRT service readiness before opening
Launch readiness checklist
Use this go-live approval checklist to confirm the service is ready before opening and taking first patient referrals.
Clearance
- State licensure approvedCritical
The service cannot open until state healthcare licensing is in place.
- Medical staff privileges securedCritical
Procedure access depends on named physicians holding the right privileges.
- Medicare enrollment activeCritical
Claiming cannot start until Medicare enrollment is live.
- Commercial payer enrollment filedHigh
Commercial approval should be filed early so referrals do not stall at billing.
Suite
- Cath lab access confirmedCritical
CRT implantation needs confirmed cath lab time and access.
- Fluoroscopy equipment checkedCritical
Fluoroscopy support must work before the first implant case.
- Sterile processing clearedCritical
Sterile processing keeps device handling and infection control on track.
- Recovery workflow rehearsedHigh
Patients need a clear recovery path after implantation and before discharge.
Supply
- CRT kit inventory lockedCritical
The first cases need confirmed CRT device and lead kit stock.
- Lead replacement workflow signedHigh
A fast replacement path reduces delays when a lead is missing or damaged.
- Consignment terms approvedHigh
Consignment or inventory terms should limit cash strain at launch.
- Vendor support roster confirmedMedium
Named vendor support helps fix device issues during the first cases.
Staffing
- Senior electrophysiologist assignedCritical
Year 1 assumes one senior electrophysiologist is in place.
- Associate electrophysiologist assignedCritical
Year 1 assumes one associate electrophysiologist is in place.
- Device specialist team staffedCritical
The Year 1 model assumes two cardiac device specialists.
- Nurse practitioner coverage setHigh
The Year 1 model assumes two cardiology nurse practitioners.
- Remote monitoring coverage setHigh
The Year 1 model assumes one remote monitoring technician.
Workflow
- Prior authorizations mappedCritical
Prior auth has to work before the first referral turns into revenue.
- Coding workflow reviewedCritical
Clean coding lowers claim denials and speeds cash collection.
- Wound checks scheduledHigh
Post-op wound checks protect safety and reduce avoidable readmits.
- Device interrogation liveHigh
Interrogation must be ready for device checks and remote review.
- Adverse-event escalation setCritical
A clear response plan is needed if a patient or device event turns urgent.
Financial
- Year 1 utilization validatedCritical
The launch model assumes 65% senior, 55% associate, 70% device, 70% NP, and 60% remote use.
- Minimum cash buffer fundedCritical
The model shows minimum cash of $886k in Month 1, so funding must be ready.
- Payroll and overhead loadedHigh
Fixed costs and wages must be loaded before go-live so margins are real.
- Go-live signoff completeCritical
Final signoff should confirm payer, inventory, safety, staffing, and follow-up readiness.
Want to check the six CRT launch drivers?
HTML error: driver 1 description is too long.Clinical Leadership And Credentialing
CRT Physician Credentialing
CRT cannot open until the implanting physician is fully credentialed. The first gate is signed facility privileges for a cardiologist or electrophysiologist with cardiac device implantation readiness, plus approved clinical protocols, a documented case selection process, and a coverage plan. Without that, the business can schedule consults, but it cannot perform implants or book day-one revenue.
Year 1 staffing assumes 1 senior electrophysiologist and 1 associate electrophysiologist, so both files need to move on time. The work also includes malpractice coverage, peer review requirements, payer enrollment, procedure protocols, and emergency escalation rules. If referrals start before privileges and payer records are active, cases pile up with no legal path to treat them.
Lock Privileges Before Booking
Build the credentialing packet first: facility privileges, malpractice coverage, peer review documents, payer enrollment, procedure protocols, and escalation rules. The readiness signal is simple: the implanting physician can actually work in the room, and the facility accepts the workflow. If any one of those pieces is missing, opening slips and first procedures slide out.
Use a go/no-go list before scheduling patients: credentialing file complete, clinical protocols approved, coverage plan signed, and payer records live. That keeps the launch from turning into a waitlist with no implants, no claims, and no cash coming in. One clean rule helps: no credentialed physician, no implant calendar.
1
Facility And Electrophysiology Lab Readiness
EP Lab Readiness
CRT can open without a new buildout, but it cannot start day one unless the lab supports the full case chain: fluoroscopy, sterile processing, anesthesia support, emergency response, recovery workflow, and accreditation alignment. A hospital or ambulatory surgery center partner can shorten the path into the 6–12 month range, but only if block time, room setup, and implant flow are already agreed.
The bottleneck is a room that can host a case but cannot finish it safely. If recovery staffing, device storage, infection control, or adverse-event response are weak, opening slips, schedules get unreliable, and patient safety takes the hit on the first procedure.
Lock the case chain
Before you book patients, verify the full operating path: where the implant happens, who staffs recovery, how emergencies escalate, and who owns sterile processing and device storage. The readiness test is simple: every step from room turn to discharge is written, staffed, and approved.
- Confirm fluoroscopy access and block time.
- Document anesthesia and emergency coverage.
- Set recovery staffing and discharge flow.
- Align infection control and accreditation tasks.
- Test implant, storage, and adverse-event steps.
If any one piece is missing, you may have a room but not a launch. That means idle schedule slots, delayed cases, and more working cash tied up while the facility chain catches up.
2
Payer Enrollment And Authorization Workflow
Payer Enrollment and Prior Authorization
CRT can’t open cleanly if the payer file is not live. Medicare and commercial enrollment, plus a clear prior authorization workflow, are the gatekeepers for claim approval, patient scheduling, and first cash in the door. If eligible patients are booked before authorization clears, you get delays, denials, and avoidable write-offs.
This setup includes provider enrollment, facility enrollment alignment, eligibility checks, medical necessity documentation, denial tracking, and collections handoff. Plan billing and collection fees at 4% of revenue in Year 1, falling to 3% by Year 5. One clean rule: no auth, no case.
Lock the billing path before the first schedule
Before opening, verify that payer enrollment is active for the provider and the facility, and that staff owns each step from eligibility to collections. Build a payer-specific checklist for medical necessity notes, auth submission, denial follow-up, and payment posting so the team does not improvise on live cases.
Use a simple launch test: the first referred patient should move from intake to eligibility check, then to authorization, then to scheduled procedure without a billing gap. If scheduling gets ahead of auth, cash timing slips and claims friction rises right away.
- Confirm Medicare and commercial status
- Align provider and facility enrollment
- Assign auth and denial ownership
- Require medical necessity documentation
3
Device Vendor And Inventory Setup
Device And Lead Inventory
This launch driver matters because CRT cases only happen when the right device, lead kit, and rep support are ready. If the lab has time but the implant set is missing, the case slips, the patient waits, and opening-day revenue gets pushed out.
Readiness starts with signed vendor onboarding, an inventory or consignment plan, a case-day ordering process, a backup supply plan, and a clean device documentation workflow. Kits are modeled at 12% of revenue in Year 1, easing to 10% by Year 5, so supply control is also margin control.
Lock Supply Before First Cases
Verify vendor credentialing, device and lead kit par levels, and representative scheduling before you open the calendar. Set the implant log, recall tracking, and replacement escalation owner now, so staff know who handles missing parts and urgent swaps.
- Confirm exact device and lead SKUs.
- Test case-day ordering before launch.
- Keep backup stock for urgent replacement.
- Assign one person to documentation.
What this hides: weak paperwork slows replacements, and poor stock control can trap cash in the wrong inventory. Keep the workflow tight enough that each case can be checked for the correct device, the correct lead, and rep coverage before the patient is in the room.
4
Referral Network And Patient Intake
Referral Intake
Cardiac Resynchronization Therapy (CRT) cannot open on time if referrals land in a messy inbox. The launch risk is marketing without clinical intake: you may get names, but not eligible cases, so consults slip and day-one revenue gets pushed back.
Build the intake path to capture diagnostics, medical records, payer details, eligibility review, and authorization status before scheduling. The referral base should focus on specialists, cardiologists, primary care physicians, hospitals, discharge planners, and device clinics, with outreach modeled at 3% of revenue in Year 1 and 25% in Year 2.
Pre-Open Intake Workflow
Before launch, verify the full handoff from referral to consult. That means physician outreach, discharge planner education, referral forms, intake triage, diagnostic document collection, consult scheduling, and feedback loops to referring clinicians. If any step is missing, first eligible cases stall and the opening runs behind schedule.
- Assign one owner for intake triage.
- Test document capture before opening.
- Track authorization status on every case.
- Close the loop with referrers fast.
One clean intake path is what turns outreach into booked procedures and keeps the launch ramp predictable from day one.
5
Post-Implant Follow-Up And Remote Monitoring
Day-One Follow-Up Capacity
CRT follow-up cannot wait. If the clinic cannot handle post-procedure visits, wound checks, device interrogation, remote monitoring enrollment, patient calls, and adverse-event response on day one, the launch is not ready. That gap shows up fast in patient safety, referral trust, and payer confidence.
The Year 1 plan assumes 2 cardiac device specialists at 40 monthly treatments each and 70% capacity, plus 1 remote monitoring technician at 200 monthly encounters and 60% capacity. Here’s the quick math: that supports about 56 treatments and 120 monitoring encounters a month. If implants grow faster than follow-up, the clinic will fall behind.
Build The Monitoring Workflow Before First Implant
Before opening, verify follow-up scheduling, device clinic protocols, remote monitoring setup, alert routing, escalation rules, patient education, and documentation. Assign one owner for each step, and test the handoff from implant day to the first post-op check so nothing depends on memory.
Use a simple launch test: every patient should leave with a scheduled follow-up, a working monitoring enrollment process, and a clear contact path for alerts. If the team cannot route and respond to device alerts within the planned staffing model, delay volume growth until the workflow is stable.
- Confirm post-op visit slots before opening.
- Test wound-check and interrogation workflows.
- Map alert routing and escalation rules.
- Train staff on patient calls and documentation.
- Match implant pace to monitoring capacity.
6
Related Products
- Cardiac Resynchronization Therapy Services Porter's Five Forces Analysis
- Cardiac Resynchronization Therapy Services BCG Matrix
- Cardiac Resynchronization Therapy Services Business Model Canvas
- What Are The 5 KPI Metrics For Cardiac Resynchronization Therapy Services Business?
- Cardiac Resynchronization Therapy Services Business Plan Template in Pre-Written Word
- How Increase Profits Cardiac Resynchronization Therapy Services?
- What Does It Cost To Run Cardiac Resynchronization Therapy Services?
- Cardiac Resynchronization Therapy Startup Costs With $72K Monthly Runway
- Cardiac Resynchronization Therapy Services Financial Model Template in Excel
- How Much Can a CRT Services Owner Make on $938M Year 1 Revenue?
- How To Write A Business Plan For Cardiac Resynchronization Therapy Services?
- Cardiac Resynchronization Therapy Services Marketing Mix
- Cardiac Resynchronization Therapy Services Marketing Plan
- Cardiac Resynchronization Therapy Services Business Proposal
- Cardiac Resynchronization Therapy Services PESTEL Analysis
- Cardiac Resynchronization Therapy Services Pitch Deck Example Editable PPTX
- Cardiac Resynchronization Therapy Services Business SWOT Analysis
- Cardiac Resynchronization Therapy Services Value Proposition Canvas
Frequently Asked Questions
Start by securing electrophysiology leadership, facility access, payer enrollment, vendor setup, and referral intake A practical launch path often takes 6–12 months through an existing accredited hospital or ambulatory surgery center The Year 1 model assumes 7 clinical roles: 1 senior electrophysiologist, 1 associate electrophysiologist, 2 device specialists, 2 cardiology nurse practitioners, and 1 remote monitoring technician