 Owner income$6.7M–$79.5M
Owner income$6.7M–$79.5MHow Much Can a CRT Services Owner Make on $938M Year 1 Revenue?

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$6.7M–$79.5M  Net margin70.9%–81.5%
Net margin70.9%–81.5% Revenue for target pay$9.4M–$97.6M
Revenue for target pay$9.4M–$97.6M Business difficultyHard
Business difficultyHard


A cardiac resynchronization therapy services owner can only take home what remains after device costs, facility fees, billing, outreach, fixed overhead, staff pay, physician compensation, debt service, and reserves In the supplied first-year assumptions, revenue is $938 million and listed costs excluding physician compensation total about $281 million, leaving $657 million before specialist pay, debt, taxes, and retained cash By the mature-year scenario, modeled revenue reaches $9756 million, but that still is not guaranteed owner income The biggest swing factors are case volume, payer collections, physician model, device-related costs, fixed overhead, and how much cash the business keeps back
Owner income$6.7M–$79.5MNet margin70.9%–81.5%Revenue for target pay$9.4M–$97.6MBusiness difficultyHardWant to test your CRT owner income?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate, not guaranteed salary, tax advice, or owner distribution advice.
Want to check owner income in the CRT model?
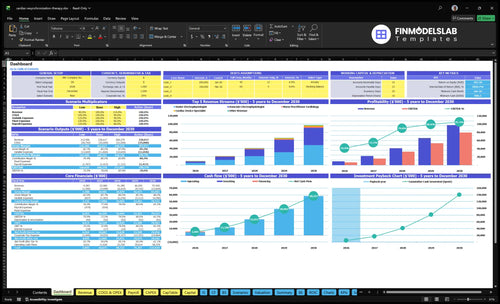
The screenshot shows revenue, margin, costs, reserves, and owner take-home assumptions; open the Cardiac Resynchronization Therapy Services Financial Model Template.
Owner-income model highlights
- Senior electrophysiologist activity
- Associate electrophysiologist activity
- Cardiac device specialist activity
- Nurse practitioner cardiology activity
- Remote monitoring technician activity
- Revenue: $938M to $9,756M
- Gross margin: 830% to 860%
- Overhead: $377k monthly
- Surplus: $657M to $7,895M
- Planning tool only
How many CRT procedures are needed to make owner income?
There isn’t one CRT procedure count that guarantees owner income. For Cardiac Resynchronization Therapy Services, the Year 1 model already includes 117 senior electrophysiologist cases, 79 associate cases, and follow-up and monitoring services, while fixed overhead is $37,700 a month, or $452,400 a year, before the $110,000 administrator salary. Here’s the quick math: annual procedures = (target owner pay + fixed costs + physician comp + debt and reserves) ÷ contribution per case, where contribution per case means what’s left after direct costs, and payer mix plus denied claims can change break-even fast.
Year 1 load
- 117 senior cases
- 79 associate cases
- Follow-up services included
- $452,400 annual overhead
What moves break-even
- Target owner pay drives volume
- Physician comp sits on top
- Debt and reserves add pressure
- Payer mix changes collections
Does owner involvement change CRT services owner income?
Yes — in Cardiac Resynchronization Therapy Services, owner involvement changes both income mix and risk. An active physician-owner can earn clinical compensation plus possible distributions, but that work can’t be counted twice as profit. A managing owner can take an operator salary, while a passive investor only works if specialist coverage, compliance, and referrals hold up as staffing grows from 1 senior and 1 associate electrophysiologist in Year 1 to 5 senior and 6 associate electrophysiologists by Year 5.
Active owner pay
- Physician-owner gets clinical pay.
- May also take distributions.
- Don’t double-count salary as profit.
- More work, more direct risk.
Passive owner risk
- Operator salary can sit with manager.
- Electrophysiologists still need pay.
- Coverage and credentialing must stay tight.
- Passive stakes depend on referrals.
Is a cardiac resynchronization therapy services business profitable?
Cardiac Resynchronization Therapy Services can be profitable in the supplied model, with $938M in Year 1 revenue and about $657M in pre-physician-comp operating surplus; use How To Write A Business Plan For Cardiac Resynchronization Therapy Services? to separate practice profit from clinical pay before calling it bankable.
Profit Math
- Year 1 revenue: $938M
- Direct costs listed: 17.0%
- Variable costs listed: 7.0%
- Operating surplus: about 70.0%
Key Caveats
- Separate physician compensation first
- Fixed overhead: $4,524k
- Administrator salary: $110k
- Watch denials, debt, taxes, compliance
Want the six drivers behind CRT owner income?
1
$9.4M-$97.6MProcedure Volume
More CRT implants and follow-ups drive the top line, and revenue scales from $9.4M in Year 1 to $97.6M in Year 5.
2
Net rev/casePayer Mix
Owner cash depends on how much billed work turns into collected revenue, since there is no single reimbursement rate.
3
2→11Physician Productivity
Throughput rises as electrophysiologist staffing grows from 2 to 11, so more billable cases can land without bottlenecks.
4
170%→140%Direct Costs
Device kits, lab fees, outreach, and billing fees eat margin, and the model still shows direct costs easing from 170% to 140%.
5
$37.7K/moFixed Overhead
A fixed base near $37.7K a month has to be spread across enough volume, or owner take-home gets pinned down.
6
$886KCash Timing
Reserves, debt service, and claim timing control how much profit can be pulled out, and month 1 minimum cash is $886K.
Cardiac Resynchronization Therapy Services Core Six Income Drivers
CRT Procedure And Follow-Up Volume
CRT Procedure and Follow-Up Volume
Cardiac resynchronization therapy (CRT) volume is the main top-line driver. More implants and follow-up visits mean more collected revenue and a better spread of fixed overhead. In the model, revenue rises from $938M in Year 1 with 1 senior electrophysiologist, 1 associate, 2 device specialists, 2 nurse practitioners, and 1 remote monitoring technician to $9,756M in Year 5 as staffing scales.
Here’s the quick math: senior capacity moves from 650% to 900%, and associate capacity from 550% to 850%. That only helps if referral flow, patient eligibility, scheduling, credentialing, lab access, and physician time all keep up. If any one of those caps volume, demand stops turning into owner income.
Track the pipeline before you add staff
Measure referrals, consult-to-procedure conversion, monthly implants, and follow-up load by clinician. A full schedule is not enough; you need enough eligible patients, open lab time, and fast scheduling to convert demand into cash. More volume only helps when the case flow is real and the team can clear it.
Use a simple weekly dashboard:
- New referrals by source
- Eligible patients by month
- Implant slots available
- Follow-up visits completed
- Remote monitoring backlog
When those counts rise together, fixed overhead gets diluted and owner pay has room to grow.
1
Payer Mix And Collections
Payer Mix And Collections
Collections decide whether completed CRT cases turn into cash. The model uses collected price assumptions of $45,000 per senior electrophysiologist treatment in Year 1 and $50,000 in Year 5, plus $42,000 to $46,000 for associate treatments; there is no single Medicare or commercial reimbursement number to quote. Authorization, coding, denials, underpayments, and lag can leave profit on paper but not in the bank.
That gap hits owner pay fast. On a multimillion-dollar revenue base, even a small collection shortfall can wipe out distributions before rent savings do. The key metric is the net collection rate (cash collected divided by allowed charges), tracked by payer, by physician, and by aging bucket. If cash is slow, profit can look fine while payroll and debt service still squeeze distributions.
Control Clean Claims Fast
Measure what turns billed cases into cash. Review payer contracts, clean-claim rate, denial rate, underpayment rate, and days in accounts receivable (A/R). Clean claims should go out right the first time, and every denial needs a root cause log so coding and authorization errors stop repeating.
- Track A/R by payer weekly.
- Age denials over 30 days.
- Compare allowed vs. paid amounts.
- Fix coding before batch billing.
Here’s the quick math: if collected price falls below plan, owner draws fall with it. Use aging reports to spot slow payers early, then tighten contract review and follow-up work before collections drift for a full quarter.
2
Physician Productivity And Specialist Compensation
Electrophysiologist Productivity And Pay
Productivity is the main revenue engine here, because each electrophysiologist’s monthly treatment count drives case volume. With 1 senior and 1 associate in Year 1, the model implies about 27 treatments per month total, rising to about 180 per month in Year 5 with 5 senior and 6 associate electrophysiologists. More cases usually lift owner income, but only if compensation doesn’t eat the margin first.
This driver includes monthly treatments per doctor, specialist headcount, and the pay model used for senior and associate physicians. The key risk is double counting: in an owner-operator setup, some clinical pay is really owner income, but in an employed-specialist setup, that same pay is a business cost. Keep clinical compensation separate from profit so distributions are not overstated.
Measure Pay Per Case, Not Just Headcount
Track treatments per physician per month, total specialist payroll, and profit before owner distributions. Here’s the quick math: if staffing scales from 2 physicians to 11 physicians, output jumps fast, but so can payroll. That makes pay per treatment the control point, not just total salary spend. A small change in comp design can decide whether growth turns into cash.
Test whether senior and associate productivity stays near the model’s move from 15 to 18 monthly senior treatments and 12 to 15 monthly associate treatments. If production rises but specialist cost rises faster, owner take-home falls. Use a simple monthly report: cases per doctor, comp per case, and cash left after payroll. That’s the number that tells you what the owner can actually pay themselves.
3
Direct Procedure Costs And Device Economics
Direct Procedure Costs Per CRT Case
For Cardiac Resynchronization Therapy, direct case costs set gross profit before overhead, debt, taxes, and owner draw. The supplied model puts CRT device and lead kits at 120% of revenue in Year 1, easing to 100% by Year 5, while cath lab facility fees move from 50% to 40%. That means small changes in procurement, disposables, and case complexity can move cash fast.
Here’s the quick math: if device pricing, lead use, and lab fees slip, per-case margin falls before fixed costs are even paid. The supplied gross margin after these direct costs improves from 830% to 860%; what matters is the direction, not just the label. A better buy price or cleaner supply use means more profit left for staffing and the owner.
Track Cost Per Implant, Not Just Revenue
Measure each case with the same inputs: procedure price, device and lead kit cost, facility fee, disposables, and vendor terms. If procurement takes longer than 14 days or case mix gets more complex, cash conversion slows and owner pay gets squeezed even when volume holds. Keep this financial and operational, not clinical.
- Track gross profit per case weekly.
- Separate kit, lab, and disposable cost.
- Test vendor pricing by case type.
- Watch inventory days and payment timing.
- Flag any cost creep above budget.
Use a simple rule: if direct costs rise faster than collected case revenue, distributions get smaller. Standardize ordering, tighten vendor contracts, and forecast by case mix so the owner sees margin drift early. One expensive supply change can erase a lot of surgery-day revenue.
4
Fixed Overhead And Operating Infrastructure
Fixed Overhead Load
Fixed overhead is the monthly cost you pay before one more CRT case shows up. Here, the listed base is $37,70 0 a month: malpractice $15,000, rent $12,000, software $4,500, utilities and medical waste $2,200, licenses $3,000, and supplies $1,000. That annualizes to $452,400, before the $110,000 practice administrator cost.
This load is heavy early on. The same cost base is 48% of Year 1 revenue but under 5% of Year 5 revenue, so slow referrals can strain cash even if per-case margin is strong. One clean line: volume makes this cheaper to carry, not smaller.
Track the Monthly Burn Rate
Measure fixed overhead as a share of collected revenue, not just booked cases. Track monthly burn = fixed costs plus administrator pay, then compare it with referral flow, scheduled procedures, and collections. If case volume slips, owner pay should wait until the run rate is covered. That keeps low volume from eating cash.
Use a break-even test each month: $37,700 ÷ gross profit per case, then add the administrator cost if it is paid from the practice. Watch denial lag, open slots, and idle staff time. If procedures do not rise fast enough, the fixed base hits take-home income before revenue can absorb it.
5
Reserves, Debt Service, And Cash Timing
Cash Timing and Reserves
Owner pay comes from cash, not profit alone. This model shows $657M Year 1 and $7895M Year 5 pre-physician-comp operating surplus, but that is before debt service, reserves, taxes, reinvestment, and distributions. A profitable CRT service can still run short if claims lag or build-out debt hits early.
Set reserves in months of operating costs and payroll, not as a leftover number. The key inputs are claim timing, payer delays, equipment financing, compliance costs, and growth hiring. One slow payer cycle can block owner draws even when procedures are booked.
Build a cash floor
Track days in accounts receivable, monthly debt payments, and payroll run rate every month. If receivables stretch or new hires come on before collections catch up, take-home pay gets squeezed fast.
- Hold reserve cash in payroll months
- Separate debt service from profit
- Watch claim lag by payer
- Stress test slow-collection months
What this estimate hides: reserve needs rise when equipment is financed, compliance costs spike, or expansion is funded too aggressively.
6
Compare lean, base, and high CRT owner-income scenarios
Owner income scenarios
Owner income moves with case volume, reimbursement, staffing, and how fully the electrophysiology team is used. Higher capacity and better mix lift EBITDA, but physician pay, debt service, and compliance still cut take-home.
| Scenario | Low CaseEarly ramp | Base CaseScaled platform | High CaseMature capacity |
|---|---|---|---|
| Launch model | Lower income comes from Year 1 ramp, with $9.383M revenue and tight capacity use. | Modeled income reflects Year 3 scale, with $41.385M revenue and better overhead absorption. | Stronger income assumes Year 5 scale, with $97.565M revenue and the best capacity use. |
| Typical setup | Year 1 runs at 65% senior capacity and 55% associate capacity, with 15 senior cases, 12 associate cases, 40 device cases, 60 nurse cases, and 200 monitoring cases per month. | Year 3 assumes 80% senior capacity and 75% associate capacity, with 16 senior cases, 14 associate cases, 45 device cases, 65 nurse cases, and 220 monitoring cases per month. | Year 5 runs at 90% senior capacity and 85% associate capacity, with 18 senior cases, 15 associate cases, 50 device cases, 70 nurse cases, and 250 monitoring cases per month. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $6.7MEarly ramp | $32.7MScaled platform | $79.5MMature capacity |
| Best fit | Best for stress-testing launch risk, reimbursement delays, and hiring pace. | Best for a practice that can hold volume and keep schedules tight. | Best for testing full build-out, specialist depth, and capacity limits. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Cardiac Resynchronization Therapy Services Porter's Five Forces Analysis
- Cardiac Resynchronization Therapy Services BCG Matrix
- Cardiac Resynchronization Therapy Services Business Model Canvas
- What Are The 5 KPI Metrics For Cardiac Resynchronization Therapy Services Business?
- Cardiac Resynchronization Therapy Services Business Plan Template in Pre-Written Word
- How Increase Profits Cardiac Resynchronization Therapy Services?
- What Does It Cost To Run Cardiac Resynchronization Therapy Services?
- Cardiac Resynchronization Therapy Startup Costs With $72K Monthly Runway
- Cardiac Resynchronization Therapy Services Financial Model Template in Excel
- How To Open A Cardiac Resynchronization Therapy Service In 6–12 Months
- How To Write A Business Plan For Cardiac Resynchronization Therapy Services?
- Cardiac Resynchronization Therapy Services Marketing Mix
- Cardiac Resynchronization Therapy Services Marketing Plan
- Cardiac Resynchronization Therapy Services Business Proposal
- Cardiac Resynchronization Therapy Services PESTEL Analysis
- Cardiac Resynchronization Therapy Services Pitch Deck Example Editable PPTX
- Cardiac Resynchronization Therapy Services Business SWOT Analysis
- Cardiac Resynchronization Therapy Services Value Proposition Canvas
Frequently Asked Questions
Owner income depends on what remains after costs, not on revenue alone In the supplied first-year model, revenue is $938M and listed costs before physician compensation total about $281M, leaving $657M before specialist pay, debt, reserves, taxes, and distributions That surplus is a planning figure, not guaranteed take-home pay