Cardiac Resynchronization Therapy Startup Costs With $72K Monthly Runway

You’re sizing the capital and cash needed to open a US cardiac resynchronization therapy (CRT) service, not choosing devices or proving clinical value This outline separates unpriced CAPEX from documented launch overhead of $72,283 per month, which includes $37,700 in fixed operating costs and $34,583 in Year 1 support wages The outcome is a startup budget that covers build-out, equipment, pre-opening setup, working capital, and first operating year funding assumptions
Estimate cardiac resynchronization therapy CAPEX before adding working capital or operating losses
Startup CAPEX Calculator
This estimates capitalized startup assets only for a cardiac resynchronization therapy service, from an existing cardiology platform through a leased outpatient suite to a dedicated EP-capable build.
CAPEX only This calculator excludes inventory, payroll runway, rent runway, deposits, debt service, working capital, malpractice premiums, payer delays, financing costs, and post-opening operating losses. Show total CAPEX, CAPEX per procedure room, and missing quote flags; the source list includes diagnostic echo and EKG machines without a dollar amount.
How does the CAPEX tab support CRT funding?
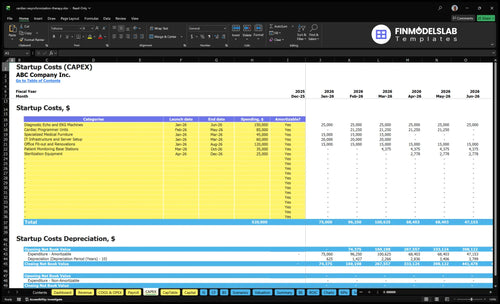
The Cardiac Resynchronization Therapy Services Financial Model Template CAPEX tab lists startup costs, timing, amounts, and depreciation; review assumptions now.
CAPEX tab highlights
- Build-out and shielding
- Imaging and EP equipment
- Echo, EKG, IT, furniture
- Licensing and payer setup
- Training and pre-opening payroll
- Month 1 to 60
- Apply depreciation after CAPEX
- $72,283 overhead; 17%, 7%
- Compare quotes and ramp
- Check payer timing, cash
How should founders plan funding for a cardiac resynchronization therapy service?
Founders should fund Cardiac Resynchronization Therapy Services around six buckets: CAPEX, pre-opening expenses, opening inventory, working capital, launch timing, and reimbursement delay. Build a monthly model with utilization ramp, revenue by provider type, direct costs, fixed costs, and cash runway so you can see when cash gets tight. For Year 1, use 1 senior electrophysiologist, 1 associate electrophysiologist, 2 cardiac device specialists, 2 nurse practitioners, and 1 remote monitoring technician.
Funding buckets
- CAPEX for buildout and equipment
- Pre-opening costs before first case
- Opening inventory for device needs
- Working capital for cash gaps
Model assumptions
- 55% to 70% utilization by role
- 12% device and lead kit costs
- 5% lab facility fees
- Validate quotes, leases, and payer timing
What is the biggest startup cost for a cardiac resynchronization therapy service?
The biggest startup cost for Cardiac Resynchronization Therapy Services is procedure infrastructure, not office furniture or marketing. That means a radiation-shielded procedure room, fluoroscopy or imaging, EP-capable monitoring, cardiac monitors, a defibrillator, a crash cart, a procedure table, sterile workflow, and a recovery area. Treat this as CAPEX and keep it separate from the $12,000 monthly clinic rent; if you use shared lab space, the upfront spend drops but you may add facility fees of about 5% of Year 1 revenue.
Startup cost driver
- Room buildout drives opening readiness.
- Shielding is part of CAPEX.
- Imaging and monitoring come first.
- Furniture is not the main cost.
What to quote
- Room, equipment, shielding as one package.
- Compliance should be priced upfront.
- Shared lab lowers initial cash need.
- Facility fees can hit Year 1 revenue.
What hidden costs should founders expect when starting a cardiac resynchronization therapy service?
Founders should budget hidden launch costs beyond CAPEX: credentialing, payer enrollment, radiation registration, accreditation readiness, malpractice binders, billing setup, device inventory timing, staff training, referral outreach, and cash reserves until collections start. Monthly fixed costs are $37,700—including $15,000 malpractice, $12,000 rent, $4,500 software, $2,200 utilities and medical waste, $3,000 licenses and professional development, and $1,000 supplies—and Year 1 support payroll adds $34,583 a month. If you want the launch math turned into a plan, see How To Write A Business Plan For Cardiac Resynchronization Therapy Services?
Launch Cost Traps
- Build in credentialing delay time.
- Expect payer enrollment lag.
- Pay for accreditation readiness early.
- Hold device inventory cash.
Monthly Cash Drag
- 3% referral outreach hits launch cash.
- 4% billing and collections fees add up.
- $34,583 support payroll starts day one.
- Working capital must bridge collections gaps.
Build a CRT service startup cost breakdown that separates CAPEX, pre-opening expenses, working capital, and excluded funding needs
Startup cost summary
Startup costs cover core lab equipment, facility build-out, and opening cash needs for a cardiology device service.
| Cost Category | Base Estimate | Main Cost Driver | CAPEX Calculator |
|---|---|---|---|
| Diagnostic Echo and EKG Machines | $150,000 | Imaging and diagnostic equipment | Yes |
| Office Fit-out and Renovations | $120,000 | Facility build-out and radiation shielding | Yes |
| Cardiac Programmer Units | $85,000 | Initial device programming hardware | Yes |
| IT Infrastructure and Server Setup | $60,000 | Clinical systems and remote monitoring setup | Yes |
| Sterilization Equipment | $25,000 | Sterile processing and procedure room readiness | Yes |
| Working capital reserve | $886,000 | 72,283 monthly overhead and launch runway | No |
Cardiac Resynchronization Therapy Services Core Five Startup Costs
Facility Build-Out and Procedure Suite Startup Expense
Build-Out CAPEX
Put the suite fit-out in CAPEX, not rent. This covers leased-space improvements, room layout, radiation shielding, electrical load, HVAC, recovery bays, sterile storage, patient flow, and emergency access. Keep $12,000 per month for clinic office rent separate, and if you use shared lab time, model facility economics through a 5% Year 1 revenue fee.
Quote the Suite
Here’s the quick math: the build-out line should be backed by contractor, shielding, electrical, and HVAC quotes, plus any room-ready costs for infection control and recovery space. Ask if launch uses existing hospital space, an office-based procedure suite, or a dedicated EP-capable facility. That choice drives the whole startup budget.
- Get room-specific contractor quotes
- Confirm shielding and power needs
- Map patient and emergency flow
Cut Rework
Save money by fitting the room once, not twice. Use existing hospital infrastructure when it already meets safety and flow rules, and avoid overbuilding if shared procedural capacity is enough. The mistake is paying for a full suite before confirming volume, access, and staffing. One clean fit-out decision can prevent months of wasted carry cost.
- Match build-out to volume
- Avoid duplicate room specs
- Check code and access early
Open-Ready Check
Before opening, confirm room configuration, shielding sign-off, electrical capacity, HVAC testing, recovery bay setup, sterile storage, infection-control workflow, patient route, and emergency access. If the suite is leased or shared, document who owns each facility cost and whether the 5% Year 1 facility fee or the $12,000 monthly rent line applies.
Clinical Equipment and Technology Startup Expense
Equipment Scope
For CRT, count clinical gear as CAPEX, not rent. Include fluoroscopy or imaging, electrophysiology (EP) recording or monitoring, cardiac monitors, defibrillator, crash cart, sterile processing, procedure tables, device-programming tech, diagnostic echo and EKG machines, IT hardware, and remote monitoring systems. Tag each item as owned, leased, shared, or facility-provided before you total the launch budget.
Lower the Buy-In
Don’t assume every item must be bought new. Lease the big-ticket devices, use refurbished monitors where allowed, and let a hospital or affiliated lab carry shared equipment when the workflow supports it. Keep the crash cart and sterile-processing path clear, then match each asset to the safest ownership model.
- Lease imaging, not just buy it.
- Use shared lab capacity where possible.
- Document who services each device.
Split Software
Keep electronic health record and remote monitoring software out of equipment CAPEX. That software is modeled at $4,500 per month, so it belongs in operating spend, not the equipment line. One clean rule helps: hardware is bought or leased once, software is paid every month.
Quote Gap
Any missing dollar amount in this CAPEX block means the startup total is not ready yet. Ask for vendor quotes on each major item, plus lease terms, shared-facility fees, and service contracts. Without those inputs, you can list the equipment stack, but you cannot publish a full launch number.
Licensing, Accreditation, and Payer Setup Startup Expense
Setup Gates
State licensure, radiation registration, payer contracting, and billing setup have to be lined up before launch. In some states, office-based surgery, ambulatory surgery center, or certificate-of-need review can add extra steps. The cash issue is simple: fixed costs start in Month 1, but revenue may lag opening.
Filing Costs
This line item covers legal setup, accreditation readiness, medical director documentation, and the filing work needed to open cleanly. Budget $3,000 per month for professional development and licenses, plus billing and collection fees at 4% of Year 1 revenue. That is separate from facility build-out and equipment.
- State license: state-specific lead time.
- Radiation registration: before first procedure.
- Accreditation: ready before opening.
- Payer status: pending until enrollment clears.
- Billing setup: live before claims go out.
Payer Timing
To keep cash tight, start payer enrollment early, confirm whether your site is hospital-based, office-based, or a dedicated procedure suite, and document who serves as medical director. That lowers rework and helps you see which filings can run in parallel. Lead times vary by state, so build slack into the launch calendar.
- Start payer contracts before build-out ends.
- Track each filing by owner and due date.
- Hold cash for Month 1 claim lag.
Cash Phases
Pre-open, cash goes out for filings, legal work, and setup. At opening, the main risk is payer status still pending, so claims can arrive after payroll and rent start. In steady state, keep the 4% billing and collection fee in your margin model and the $3,000 monthly license budget in overhead.
Staffing Readiness and Credentialing Startup Expense
Launch Staffing
This cost covers the people and process work needed before first case: onboarding, training, privileging, payer credentialing, and procedure protocols. Year 1 staffing assumes 1 senior electrophysiologist, 1 associate electrophysiologist, 2 cardiac device specialists, 2 nurse practitioners, and 1 remote monitoring technician.
Support Payroll
Year 1 support payroll totals $415,000 a year, or $34,583 monthly. Here’s the quick math: $110,000 practice administrator + $65,000 billing and coding specialist + 2 × $45,000 front desk coordinators + $95,000 clinical nurse lead + $55,000 patient liaison. Treat this as fixed launch burn.
- Lock start dates by role
- Separate clinician and support pay
- Budget by credentialing milestone
Credentialing Timing
The main risk is hiring before approvals are live. Start enrollment, privileging, and protocol review early, then stage hires to case volume. If payer setup slips, revenue can lag while $34,583 of support wages still runs each month, so cash planning should follow the approval calendar, not the lease date.
Month 1 Cash Pressure
Use three dates to control launch cash: payer effective date, privileging approval, and first procedure date. If any of those move, delay nonessential hires and keep remote monitoring and front desk coverage lean until volume is real.
Initial Inventory, Supplies, and Insurance Startup Expense
What it covers
Initial inventory for CRT should separate owned inventory, consigned inventory, per-case supplies, insurance binders, and opening cash reserves. Include CRT generators, leads, implant kits, sterile packs, disposables, and contrast or medications where used. Implantable device costs may be bought, consigned, or billed through facility arrangements, so the startup file should match the operating model.
How to model it
Here’s the quick math: model device and lead kits at 12% of Year 1 revenue, then 10% by Year 5. Size first-month stock from expected cases and unit quotes, not guesses. Add $15,000 a month for malpractice from Month 1, plus $2,200 monthly for utilities and medical waste.
How to keep cash tight
Use vendor consignment for high-cost implants when you can, and keep bought stock to the cases on hand. Don’t overbuild sterile packs or disposables; tie orders to scheduled procedures and refill points. One line item should show the case supply reserve, because it protects quality without tying up cash in idle inventory.
Opening cash reserve
The opening reserve should cover the first buying cycle, the $15,000 monthly liability bill, and the $2,200 monthly utilities and waste load before collections catch up. If the first month’s case volume is uneven, cash matters more than stock depth. Keep this reserve separate from owned and consigned inventory.
Compare lean, base, and full CRT service startup cost scenarios without unsupported vendor pricing
Scenario Table
Launch costs rise as you move from shared rooms and imaging to a dedicated EP suite. These scenarios help size cash needs for a shared start, an outpatient setup, or a full build.
| Scenario | Lean LaunchLowest CAPEX | Base LaunchShared capacity | Full LaunchHighest control |
|---|---|---|---|
| Launch model | Adds CRT to an existing cardiology or hospital-affiliated platform with shared core services. | Runs as an outpatient service with leased or shared procedure capacity. | Builds a dedicated EP-capable site with full shielding, imaging, recovery, equipment, and compliance control. |
| Typical setup | Uses shared room, imaging, recovery, compliance, and staffing support. | Uses the 5% catheterization lab facility fee and a $72,283 monthly overhead anchor. | Carries the highest CAPEX for fit-out, rooms, devices, and support systems. |
| Cost drivers |
|
|
|
| Planning rangeCAPEX only | Lowest funding needLeanest start | Midrange funding needBalanced start | Highest funding needDedicated suite |
| Best fit | Best for a group adding CRT to an existing site and wanting fast startup with shared infrastructure. | Best for operators who want a controlled start without building a full EP suite. | Best for sponsors that want full control and can fund a larger build. |
Planning note: Scenario ranges are model-based planning assumptions, not exact vendor quotes or lease bids.
Related Products
- Cardiac Resynchronization Therapy Services Porter's Five Forces Analysis
- Cardiac Resynchronization Therapy Services BCG Matrix
- Cardiac Resynchronization Therapy Services Business Model Canvas
- What Are The 5 KPI Metrics For Cardiac Resynchronization Therapy Services Business?
- Cardiac Resynchronization Therapy Services Business Plan Template in Pre-Written Word
- How Increase Profits Cardiac Resynchronization Therapy Services?
- What Does It Cost To Run Cardiac Resynchronization Therapy Services?
- Cardiac Resynchronization Therapy Services Financial Model Template in Excel
- How Much Can a CRT Services Owner Make on $938M Year 1 Revenue?
- How To Open A Cardiac Resynchronization Therapy Service In 6–12 Months
- How To Write A Business Plan For Cardiac Resynchronization Therapy Services?
- Cardiac Resynchronization Therapy Services Marketing Mix
- Cardiac Resynchronization Therapy Services Marketing Plan
- Cardiac Resynchronization Therapy Services Business Proposal
- Cardiac Resynchronization Therapy Services PESTEL Analysis
- Cardiac Resynchronization Therapy Services Pitch Deck Example Editable PPTX
- Cardiac Resynchronization Therapy Services Business SWOT Analysis
- Cardiac Resynchronization Therapy Services Value Proposition Canvas
Frequently Asked Questions
The provided model shows $72,283 in documented monthly opening overhead before unpriced CAPEX and physician compensation That includes $37,700 in fixed costs and $34,583 in Year 1 support wages The largest listed monthly fixed items are malpractice insurance at $15,000, clinic rent at $12,000, and software at $4,500