 Owner income$220K base
Owner income$220K baseDirect Primary Care Practice Owner Income: $220K Plus EBITDA

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$220K base  Net margin0% to 60.1%
Net margin0% to 60.1% Revenue for target pay$987K
Revenue for target pay$987K Business difficultyHard
Business difficultyHard


You’re estimating owner take-home from a US direct primary care practice, not treating revenue as salary This model covers a five-year membership ramp, with $987,000 Year 1 revenue, $220,000 physician payroll, Month 7 breakeven, reserves, reinvestment, and exclusions for personal taxes, debt structure, and individual compensation advice
Owner income$220K baseNet margin0% to 60.1%Revenue for target pay$987KBusiness difficultyHardWant to test your DPC owner income?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. Actual owner income depends on revenue, margins, payroll, taxes, reserves, and timing. It is not guaranteed salary, tax advice, or owner distribution advice. The model also shows Month 7 breakeven and about 552000 in minimum cash need.
Want to pressure-test the full Direct Primary Care Practice forecast?
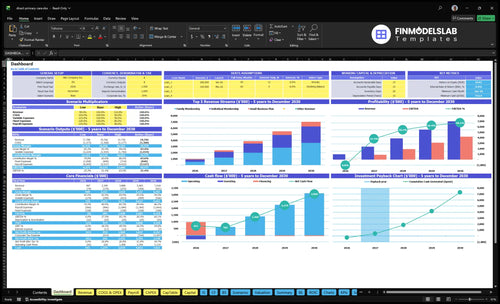
The Direct Primary Care Practice Financial Model Template adds dashboard, assumptions, income statement, cash flow, break-even, payback, and scenario tabs. It tests member ramp, pricing tiers, physician FTE growth, payroll from $490K to $128M, revenue from $987K to $7,018M, EBITDA from $0 to $4,219M, and minimum cash of $552K. Open the model.
Owner pay planning checks
- Owner take-home planning
- Revenue and margin
- Scenario stress tests
How many patients does a direct primary care doctor need?
A Direct Primary Care Practice needs about 706 average active paying members in Year 1, based on $987K revenue ÷ ($116.50 monthly fee × 12); track paying members, not inquiries, and pair this with What Five KPIs Should Direct Primary Care Practice Track?. By Year 5, $7.018M revenue ÷ ($173.30 × 12) implies about 3,375 average memberships; if that is spread across 30 physician FTE, the math is 113 members per physician, not 1,125.
Panel math
- 706 Year 1 average members
- $116.50 weighted monthly fee
- $987K Year 1 revenue
- Month 7 breakeven depends on ramp
Capacity checks
- 3,375 Year 5 average memberships
- $173.30 Year 5 monthly fee
- 30 physician FTE capacity base
- Churn and access quality cap panels
Can direct primary care replace a physician salary?
Yes—if you're asking whether a Direct Primary Care Practice can pay a physician a $220K annual salary from day one, the model says yes. But Year 1 EBITDA is $0 after payroll, so that cash is salary, not owner distributions. By Year 2, EBITDA reaches $897K, and by Year 5 it reaches $4.219M before taxes, debt service, reserves, and reinvestment; payback is 20 months, so cash planning has to come first.
Cash timing
- Month 1 supports salary.
- Year 1 EBITDA stays at $0.
- Payback lands in 20 months.
- Distributions wait for cash build.
Owner economics
- $220K is the physician salary.
- Year 2 EBITDA reaches $897K.
- Year 5 EBITDA reaches $4.219M.
- Taxes and reserves cut take-home cash.
What direct primary care operating costs reduce owner income most?
Payroll is the biggest squeeze on owner income in a Direct Primary Care Practice, and the ramp is brutal: it moves from $490K in Year 1 to $128M in Year 5. Even with strong gross margin, take-home stays tight because fixed overhead runs about $14K per month and variable costs start at 135% of revenue before easing to 95% by Year 5.
Biggest cost drains
- Payroll is the main pressure point.
- Fixed overhead stays around $14K/month.
- Rent is $85K, with $25K malpractice.
- Utilities add $12K, plus admin costs.
Why income stays tight
- Variable costs start at 135% of revenue.
- Supplies and telehealth/EHR drive early pressure.
- Marketing rises from $120K to $300K.
- High gross margin does not mean high take-home.
Want the six DPC income drivers?
1
706-3,375Active Members
More enrolled members spread the same clinic base, so owner take-home scales faster than costs.
2
$116-$173Membership Fee
A higher weighted fee raises cash per member and lifts margin without adding visits.
3
10-30 FTEPhysician Capacity
More physician FTE opens more patient slots, so growth keeps flowing before service slows.
4
$490K-$1.28MStaff Mix
Payroll is the biggest controllable cost, so the right FTE mix protects take-home as the panel grows.
5
$14K/moFixed Overhead
The $14K monthly overhead line sets break-even, and every extra member above it adds more cash.
6
$85->$60Enrollment Efficiency
Lower CAC means each new member costs less to win, which shortens payback and raises owner yield.
Direct Primary Care Practice Core Six Income Drivers
Active Paying Member Count
Active Paying Member Count
Each active paying member adds recurring cash, but it also adds visit volume, messaging, and care follow-up. In the provided model, the Year 1 weighted monthly fee is $11,650, and contribution after 135% variable costs is about $10,078 per member per month. That makes member count the main driver of revenue and margin.
The scale effect is strong: the model says 100 extra active members add about $101K monthly contribution before payroll and fixed costs. By Year 5, contribution rises to about $15,684 per member per month, so retention matters more than sign-ups. If churn rises or physician capacity fills up, owner pay stops scaling cleanly.
Track member count, not just sign-ups
Measure active members, monthly churn, and members per physician together. Here’s the quick math: more members help only when retained members stay inside physician capacity and access stays strong. If same-day visits slip, churn can erase the extra contribution fast.
- Active members by month
- Monthly churn rate
- Members per physician
- Contribution per member
Use that scorecard to decide when to add staff or slow enrollment. Member growth improves owner take-home income only after payroll and fixed costs are covered. If the panel grows faster than care capacity, the business gets busier without giving the owner much more cash.
1
Average Monthly Membership Fee
Average Monthly Membership Fee
Average monthly membership fee is the price each active member pays every month, before any add-ons. Here’s the quick math: the weighted fee rises from $11,650 in Year 1 to $17,330 in Year 5, so revenue per member improves even if headcount stays flat. That lifts cash flow and owner draw, but only if members keep renewing.
Mix matters. Family memberships grow from 30% to 38%, individual plans fall from 45% to 35%, and small business plans move from 25% to 27%. Fee increases help margin only when retention and local value hold; if churn rises, the higher price can backfire.
Track Fee Mix, Not Just List Price
Track monthly fee by plan, active member count, and churn by cohort. Compare realized revenue per active member with the weighted target so you can see whether family plans or employer plans are lifting the average fee. If the average fee rises but renewals slip, take-home income usually falls.
Test price changes in small steps and watch renewals, referrals, and visit use. The key input is not one ideal price; it is the balance between higher monthly revenue and stable retention. Build the forecast around plan mix, because shifts toward families or small business accounts change monthly cash fast.
2
Physician Panel Capacity
Physician Panel Capacity
Physician panel capacity is the ceiling on active members each doctor can safely handle. In the model, physician FTE grows from 10 in Year 1 to 30 in Year 5, and active memberships rise from about 706 to about 3,375. More capacity lifts recurring revenue, but only if access stays fast enough to keep members paying.
Same-day access, longer visits, virtual care, and clinical scope set sustainable panel size. The model also states about 1,125 members per physician by Year 5, so that assumption should be tested against visit volume and retention. If panels get too full, wait times rise, churn can rise, and owner profit can fall even with more members.
Keep the panel tied to access
Track active members per physician FTE, same-day slot fill, telehealth share, visit length, and churn. These inputs show whether capacity is still supporting revenue or starting to hurt it. If a fuller panel lowers renewals, the extra membership revenue can disappear into rework, complaints, and lower take-home pay.
- Members per physician FTE
- Same-day access
- Visit length
- Telehealth mix
- Churn rate
- Clinical scope
Set a panel cap from service math, not from ambition. Test growth until next-day demand, message volume, or renewal rates start to soften. That is the point where income quality weakens, because each added member no longer produces clean margin and stable cash flow.
3
Clinical And Administrative Staffing
Clinical and Administrative Staffing
Staffing is the tradeoff between service quality and owner pay. In Year 1, payroll is $490K across physician, registered nurse, medical assistant, practice manager, and marketing/business development roles, so lean staffing helps margins during ramp. But under-staffing can slow enrollment and raise churn, which cuts recurring revenue and delays the owner’s take-home.
Track payroll against growth
Measure staffing with FTE, active members, churn, and owner workload. The model reaches $128M of payroll by Year 5 as physician, nurse, assistant, and admin FTE expand, so each hire needs to protect access, retention, and enrollment speed. If same-day access slips or the owner is still covering admin work, payroll is too thin for the service promise.
- Track payroll per active member.
- Watch wait time and churn.
- Add staff only when demand supports it.
4
Fixed Overhead And Startup Costs
Fixed Overhead Pressure
$14K in monthly fixed overhead means the practice has to cover rent, malpractice, and admin costs before the owner sees pay. Here’s the quick math: at $987K in revenue, that is about $168K a year, or roughly 17% of sales. At the modeled Year 5 revenue level of $7.018M, the same overhead falls to about 2.4% of sales.
$250K of startup capex for systems, equipment, setup, security, website, and signage is launch cash, not monthly opex. It still affects owner income because it delays payback and can force the business to grow before it can safely pay distributions. If membership ramp is slow, fixed costs create break-even pressure fast.
Track Burn Against Signed Members
Separate one-time capex from monthly operating expense in the forecast. Track cash burn, meaning monthly cash outflow, plus the member count needed to cover the $14K fixed base before owner draw. If rent or malpractice changes, update bre ak-even right away.
- Watch fixed cost per active member.
- Test ramp speed against cash runway.
- Lock launch spend before opening day.
- Reforecast when revenue mix changes.
Owner pay gets easier only when recurring revenue stays ahead of overhead. If the practice reaches scale fast, fixed costs shrink as a share of sales; if it doesn’t, every slow month pushes profit and take-home down.
5
Retention And Enrollment Efficiency
Retention and Enrollment Efficiency
In a membership clinic, income comes from active members who stay paid, not just sign-ups. Better retention keeps monthly cash predictable, and better enrollment efficiency lowers customer acquisition cost (CAC) from $85 in Year 1 to $60 in Year 5, so the same marketing dollar buys more members. If churn rises, revenue still slips and owner pay gets less stable.
Here’s the quick math: at $120K marketing spend and $85 CAC, you can acquire about 1,412 members; at $300K and $60 CAC, that rises to 5,000. That only turns into durable income if onboarding, employer contracts, referrals, and reputation keep those members active. Lifetime value can’t be measured well without churn data, and it isn’t provided.
Track churn before you scale ads
Measure new sign-ups, active members, churn rate, and CAC every month. Use a simple funnel: leads, consultations, paid members, then retained members at 30, 90, and 180 days. If CAC improves but retention weakens, the marketing budget buys short-lived revenue, not dependable cash flow.
- Track retention by cohort month.
- Split individual, family, employer plans.
- Compare CAC to first-year gross margin.
- Test onboarding touchpoints in week one.
- Use referrals to lower paid CAC.
The owner wins when each acquired member stays long enough to cover acquisition cost and keep paying monthly. If onboarding takes 14+ days or access is slow, churn risk rises and marketing spend turns into temporary revenue instead of steady profit and draw.
6
Compare low, base, and high DPC owner income scenarios
Owner income scenarios
Income shifts with enrollment speed, CAC, and membership mix. The model reaches Month 7 breakeven, needs a $552K cash floor, and builds EBITDA from $0 to $4,219K by Year 5.
| Scenario | Low CaseLow Case | Base CaseBase Case | High CaseHigh Case |
|---|---|---|---|
| Launch model | Owner income stays thin until enrollment improves and reserves stay high. | Owner income follows the modeled ramp and starts to open up after breakeven in Month 7. | Owner income improves faster when enrollment ramps early and more cash clears reserves. |
| Typical setup | Revenue ramps slower than planned, CAC stays above $85, the mix skews to lower-fee memberships, and cash stays locked to protect the $552K floor. | Revenue runs from $987K in Year 1 to $7,018K in Year 5, EBITDA moves from $0 to $4,219K, and the $552K cash floor limits early distributions. | The practice gets a stronger family and employer mix, CAC trends toward $60, provider capacity scales sooner, and more EBITDA becomes available for distributions. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | Minimal distribution poolLow Case | Modeled draw pathBase Case | Expanded distribution poolHigh Case |
| Best fit | Use this to test a slow start with tight cash and little owner payout. | Use this as the working case for owner pay and cash timing. | Use this to test upside if growth outpaces the base plan and capacity expands sooner. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or actual distributions.
Related Products
- Direct Primary Care Practice Porter's Five Forces Analysis
- Direct Primary Care Practice BCG Matrix
- Direct Primary Care Practice Business Model Canvas
- What Five KPIs Should Direct Primary Care Practice Track?
- Direct Primary Care Practice Business Plan Template in Pre-Written Word
- How Increase Profits Direct Primary Care Practice?
- What Are Operating Costs For Direct Primary Care Practice?
- Direct Primary Care Startup Costs: $552K Cash Need To Month 6
- Direct Primary Care Financial Model Template in Excel
- How To Open A Direct Primary Care Practice In 7 Months
- How To Write A Business Plan For Direct Primary Care Practice?
- Direct Primary Care Practice Marketing Mix
- Direct Primary Care Practice Marketing Plan
- Direct Primary Care Practice Business Proposal
- Direct Primary Care Practice PESTEL Analysis
- Direct Primary Care Pitch Deck Example Editable PPTX
- Direct Primary Care Practice Business SWOT Analysis
- Direct Primary Care Practice Value Proposition Canvas
Frequently Asked Questions
In this model, an owner-physician can plan around a $220,000 physician payroll role, with distributions depending on profit and reserves EBITDA is $0 in Year 1, then $897,000 in Year 2 and $4219 million in Year 5 That profit pool is before personal taxes, debt service, and retained cash decisions