Direct Primary Care Startup Costs: $552K Cash Need To Month 6

You’re planning a membership-based primary care practice before recurring patient revenue fully covers payroll, rent, insurance, and launch marketing This startup cost outline covers $250K in CAPEX, pre-opening expenses, staffing readiness, technology setup, supplies, insurance, and the $552K minimum cash need shown in Month 6 These are researched planning assumptions, not vendor quotes or guaranteed budgets
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates capitalized startup assets only for a direct primary care practice.
What this excludes This calculator covers capitalized startup assets only. It excludes working capital, payroll runway, inventory, deposits, debt service, marketing spend, licensing fees, and other non-capital pre-opening costs.
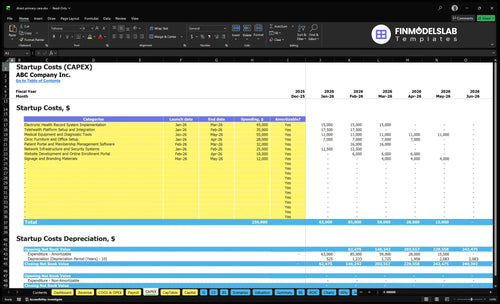
What does this financial model screenshot show?
This shows the CAPEX tab: startup costs, launch timing, amounts, and depreciation/amortization. Open Direct Primary Care Practice Financial Model Template and adjust assumptions.
Key screenshot highlights
- Startup costs listed
- Depreciation flagged clearly
- Cash runway checked
What drives direct primary care office buildout cost the most?
A Direct Primary Care Practice buildout cost is driven mostly by founder choices, not contractor quotes: facility size, exam room count, whether the space was already medical, landlord allowance, accessibility needs, utilities, signage, and waiting-area scope. In the base model, $28K goes to clinic furniture and office setup and $12K to signage, while rent is $8,500 per month and utilities plus maintenance are $1,200 per month. Here’s the quick math: overbuilding before panel density rises can create real Month 6 cash pressure.
Main cost drivers
- Pick a smaller facility first
- Limit exam rooms early
- Use a medical-ready space
- Keep waiting area simple
Cash pressure to watch
- $8,500 monthly rent
- $1,200 utilities and maintenance
- $28K furniture and setup
- $12K signage
How should I fund a direct primary care practice?
For a Direct Primary Care Practice, fund the ramp, not just launch day: the base case needs $552K minimum cash by Month 6, reaches breakeven in Month 7, and pays back in Month 20. Here’s the quick math: year 1 membership mix is 45% individual at $99/month, 30% family at $199/month, and 25% small business at $49/month. With a $120K marketing budget and $85 CAC, test slower panel growth, higher rent, delayed opening, and higher staffing needs before you choose debt, equity, savings, or partner funding.
Funding need
- $552K minimum cash by Month 6
- Breakeven in Month 7
- Payback in Month 20
- $120K marketing budget in year 1
Model tests
- Test slower panel growth
- Test higher rent
- Test delayed opening
- Test higher staffing needs
What hidden costs of starting a direct primary care practice do founders miss?
The hidden costs are mostly pre-opening items, not the clinic buildout: malpractice deposits, legal review of membership agreements, compliance setup, medical board registration, a CLIA waiver if applicable, software onboarding, cybersecurity, launch marketing, supplies, and payroll before members start paying. If you want the setup sequence, How To Launch Direct Primary Care Practice? lays it out cleanly. Here’s the quick math: the base fixed load is about $4,300/month from $2,500 malpractice insurance, $600 licenses and compliance, $400 general liability, and $800 office supplies.
Before opening
- Pay malpractice deposits up front.
- Review membership agreements legally.
- Set up compliance and board registration.
- Budget software, cybersecurity, marketing, and payroll.
After launch
- Plan for $2,500 malpractice monthly.
- Carry $600 for licenses and compliance.
- Carry $400 for general liability.
- Set aside $800 for supplies and hybrid billing admin.
Calculate Fuding Needs
Startup Cost Summary
This table separates startup CAPEX from excluded cash needs for a direct primary care practice.
| Cost Category | Base Estimate | Main Cost Driver | CAPEX Calculator |
|---|---|---|---|
| Medical Equipment and Diagnostic Tools | $55,000 | Diagnostic equipment scope and vendor grade | Yes |
| Electronic Health Record System Implementation | $45,000 | Implementation depth and integration work | Yes |
| Telehealth Platform Setup and Integration | $35,000 | Setup scope and software integration | Yes |
| Patient Portal and Membership Management Software | $32,000 | Portal features and membership workflow | Yes |
| Clinic Furniture and Office Setup | $28,000 | Buildout scope and furnishing quality | Yes |
| Minimum Cash Reserve | $552,000 | Launch losses, payroll ramp, and operating reserve through Month 6 | No |
Direct Primary Care Practice Core Five Startup Costs
Facility and buildout Startup Expense
Lease Deposit
A direct primary care office needs cash before opening: lease deposit, minor renovations, exam room setup, waiting area fit-out, accessibility work, signage, and utility hookup. In the base model, monthly rent is $8,500 and utilities plus maintenance are $1,200, so rent drag is $9,700 a month before staff or medical gear.
Buildout Budget
Model the upfront cash as separate lines: lease deposit, $28K for clinic furniture and office setup CAPEX, and $12K for signage CAPEX. The buildout also needs exam room flow, a small waiting area, storage, and accessibility work. Any landlord allowance should reduce cash outlay, but only if it is written into the lease.
Keep It Lean
Keep the layout simple: enough exam rooms for the visit pattern, basic finishes, and standard utility setup. Get local quotes for drywall, flooring, plumbing, and electrical, since contractor pricing changes by market. Don’t underbuild accessibility or signage; fixing those later usually costs more than doing them once.
Allowance Check
If the landlord offers an improvement allowance, treat it as a funding offset, not free money. Track the amount, timing, reimbursement rules, and any rent tradeoff. If reimbursement happens after work is done, you still need cash to front the buildout.
Medical equipment and clinical assets Startup Expense
Core gear
$55K covers durable medical equipment and diagnostic tools, not day-to-day supplies. Think exam tables, stools, wall diagnostic sets, scales, and any EKG or point-of-care devices, plus vaccine refrigeration, lab draw setup, sterilization, and procedure gear if you offer those services.
What drives it
Size this line from the number of exam rooms, the in-house procedures you’ll perform, and whether you’ll store vaccines or draw labs. Here’s the quick math: room count × setup package, plus add-ons for cold storage, sterilization, and procedure tools. Consumables stay separate and are modeled at 8% of Year 1 revenue.
- Count rooms first
- Price each device
- Keep supplies separate
Spend smarter
Match purchases to actual service mix, not wish list extras. Used equipment can cut upfront cash needs, but only if it’s reliable and compliant. The cleanest savings come from deferring low-use items until patient volume justifies them. Don’t bury consumables in equipment capex; that distorts the startup budget and the monthly burn.
- Buy for current scope
- Ask for used quotes
- Delay low-use devices
Budget split
Equipment is the upfront clinical build; supplies are the recurring use items. For a direct primary care launch, keep the $55K asset budget separate from the 8% of Year 1 revenue supply line so you can see cash needs, replacement timing, and margin pressure clearly.
Technology, EHR, and membership billing Startup Expense
Launch Stack
Direct primary care tech is a launch build, not a small monthly add-on. The base stack is $155K upfront: $45K EHR implementation, $35K telehealth setup, $32K patient portal and membership software, $25K network security, and $18K website and enrollment. Add phones, computers, and printers inside the buildout.
Cost Inputs
Estimate it from vendor quotes, user count, and rollout scope. Split one-time setup from recurring fees, then model platform charges at 55% of Year 1 revenue. That keeps onboarding, integration, and security cash visible early. The mistake is treating EHR and billing like a tiny subscription when the first-year cash need is mostly implementation.
Monthly Drag
The monthly drag is not just software fees. You also need phones, cybersecurity, support, and the tools that keep scheduling, telehealth, and billing moving. Budget one capital line for launch and one recurring fee line tied to Year 1 revenue. If cash is tight, underfunding shows up first in integration delays.
Cash Timing
Plan for $155K of upfront tech CAPEX plus variable platform fees at 55% of Year 1 revenue. Onboarding and integration hit cash before members ramp, so this line needs launch funding, not just monthly operating room.
Licensing, legal, insurance, and compliance Startup Expense
Legal setup
One-time legal setup covers entity formation, membership agreement review, state-specific direct primary care compliance, medical board registration, and a CLIA waiver if you run tests in-house. Budget it as pre-opening cash, not a monthly fee. State rules vary, and this is not legal advice.
Monthly insurance
Base monthly premiums are $2,500 for malpractice, $600 for professional licenses and compliance, and $400 for general liability, or $3,500 per month before workers’ compensation. If you hire staff, price workers’ comp from payroll and job class. Keep this in operating expense, not startup CAPEX.
Compliance checks
Ask early about workers’ compensation and whether your service mix needs a CLIA waiver. Those two items change with staffing and in-house testing. Here’s the quick filter: if payroll starts, get a workers’ comp quote; if you draw or run tests, confirm lab rules before opening.
- Verify state filing steps
- Quote payroll-linked workers’ comp
- Match tests to CLIA scope
Cash timing
Keep one-time setup, deposits, and monthly premiums in separate lines so opening cash is clear. That makes it easier to see what you owe before the first member pays and what repeats every month after launch.
Staffing readiness, launch marketing, and initial supplies Startup Expense
Payroll burn
This startup cost is mostly people and launch spend, not equipment. At the stated Year 1 staffing rates, payroll is about $4.9M, before the $120K marketing budget and supplies at 8% of revenue. That makes staffing readiness the biggest cash decision, especially while the physician owner ramps and the panel is still small.
Staffing build
Model staffing as 10 FTE (full-time equivalents) physician at $220K, 10 FTE registered nurse at $85K, 10 FTE medical assistant at $42K, 10 FTE practice manager at $75K, and 10 FTE marketing manager at $68K. The math totals $4.9M a year, or about $408K a month, before launch payroll timing.
- Carry pre-open months of payroll.
- Train before patient volume peaks.
- Hire the manager early.
Launch marketing
The $120K marketing budget covers website launch, local outreach, and patient onboarding materials, plus the marketing lead who runs it. At $85 CAC (customer acquisition cost), that spend implies about 1,412 new members ($120,000 ÷ $85). Keep this separate from retention marketing and monthly advertising so you can see what it costs to open the doors.
- Launch the website first.
- Track CAC by channel weekly.
- Budget onboarding materials separately.
Initial supplies
Clinical consumables belong in operating burn, not one-time buildout, and they run at 8% of revenue. That means every $100K of revenue needs about $8K for gloves, swabs, patient form s, and room restock, while uniforms and office supplies should be bought once for opening week. This keeps launch cash clean and avoids double counting monthly supply use.
Compare 3 Startup Cost Scenarios
Startup cost scenarios
Room count, staffing, and marketing runway move startup cash need fast. Lean, base, and full cases help you size the practice around the founder's coverage plan and growth pace.
| Scenario | Lean LaunchSolo physician | Base LaunchStandard launch | Full LaunchMulti-provider growth |
|---|---|---|---|
| Launch model | A founder-led clinic with fewer exam rooms, lean staff coverage, and a shorter marketing runway. | A physician-led clinic built around the model's anchor costs and a normal first-year operating plan. | A larger launch with more rooms, broader staff coverage, and extra working capital for a faster member push. |
| Typical setup | One physician, limited room buildout, and only the core equipment needed to start seeing members. | One full clinic site with standard rooms, core equipment, startup software, and the base staff mix. | More exam rooms, more equipment, and higher staffing coverage to support multiple physicians or heavier visit volume. |
| Cost drivers |
|
|
|
| Planning rangeCAPEX only | $350,000 - $550,000Lower cash need | $550,000 - $850,000Base case | $850,000 - $1,250,000Higher cash need |
| Best fit | Best for a solo physician testing local demand and keeping monthly overhead tight. | Best for a standard launch that wants enough cash to open, market, and cover the first ramp. | Best for multi-provider growth and founders planning to scale past a single-physician start. |
Planning note: These ranges are planning assumptions built from the model inputs, not exact vendor quotes or fixed build costs.
Related Products
- Direct Primary Care Practice Porter's Five Forces Analysis
- Direct Primary Care Practice BCG Matrix
- Direct Primary Care Practice Business Model Canvas
- What Five KPIs Should Direct Primary Care Practice Track?
- Direct Primary Care Practice Business Plan Template in Pre-Written Word
- How Increase Profits Direct Primary Care Practice?
- What Are Operating Costs For Direct Primary Care Practice?
- Direct Primary Care Financial Model Template in Excel
- Direct Primary Care Practice Owner Income: $220K Plus EBITDA
- How To Open A Direct Primary Care Practice In 7 Months
- How To Write A Business Plan For Direct Primary Care Practice?
- Direct Primary Care Practice Marketing Mix
- Direct Primary Care Practice Marketing Plan
- Direct Primary Care Practice Business Proposal
- Direct Primary Care Practice PESTEL Analysis
- Direct Primary Care Pitch Deck Example Editable PPTX
- Direct Primary Care Practice Business SWOT Analysis
- Direct Primary Care Practice Value Proposition Canvas
Frequently Asked Questions
This model needs $552K of minimum cash by Month 6 That reserve carries the practice through $250K of CAPEX, $490K of Year 1 wages, $120K of Year 1 marketing, and fixed monthly overhead of $14K The key is funding the gap before breakeven in Month 7