 Time to Open24 monthsSetup window
Time to Open24 monthsSetup windowHow to Open a Hospital: 18–36+ Month Launch Roadmap

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Time to Open24 monthsSetup window  Launch Sequence8 stagesCompliance first
Launch Sequence8 stagesCompliance first Key BottleneckLicense gateState rules
Key BottleneckLicense gateState rules First Revenue StepClean claimsCoding live
First Revenue StepClean claimsCoding live


Key Takeaways
- Approvals are the launch gate; without them, nothing opens.
- Facilities and life-safety systems must pass before admissions.
- Licensed staff and training drive safe first-day capacity.
- Revenue starts with payer setup, clean claims, and referrals.
Time to Open24 monthsSetup windowLaunch Sequence8 stagesCompliance firstKey BottleneckLicense gateState rulesFirst Revenue StepClean claimsCoding liveHospital launch timeline
This is a short web summary of the hospital launch timeline; the XLSX export contains the detailed Gantt Chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8Month 9Month 10Month 11Month 12
Regulatory
- Feasibility check
- Approval filing
- License prep
- Survey prep
- Life-safety check
Buildout
- Lease close
- Space design
- Buildout phase
- Safety install
- Final walkthrough
Systems
- EHR setup
- Data center
- Imaging install
- Lab analyzers
- Monitoring systems
Staffing
- Leadership hire
- Nurse hiring
- Physician credentialing
- Department heads
- Mock shifts
Payers
- Payer enrollment
- Coding setup
- Fee schedule
- Claims test
- Denial workflow
Go-live
- Referral outreach
- Transfer protocols
- Mock survey
- Soft opening
- Full go-live
Want to test launch assumptions before go-live?
Use the Hospital Financial Model Template to test dashboard, revenue ramp, staffing, costs, cash runway, and break-even before go-live, including delayed opening and slower admissions.
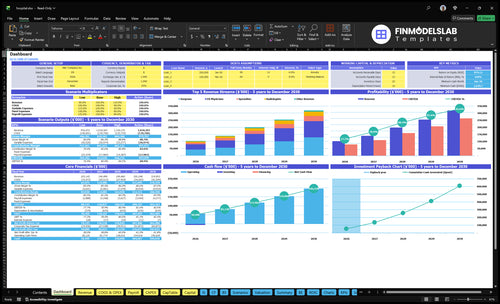
Launch model highlights
- 85-provider staffing schedule
- $86M service revenue
- 195% direct cost load
- $475k monthly overhead
What licenses do you need to open a hospital?
To open a Hospital, you usually need state hospital licensure, Certificate of Need approval where required, Centers for Medicare & Medicaid Services certification or deemed-status accreditation, local building and fire permits, life-safety clearance, and pharmacy or lab approvals if offered; treat each item as a launch gate, not a paperwork sequence, and tie readiness to What Is The Most Critical Measure Of Success For Your Hospital?.
Core approvals
- Secure the state hospital license
- Check CON rules in 35 states plus DC
- Meet CMS rules under 42 CFR Part 482
- Use approved accreditation if allowed
Launch risks
- Pass building, fire, and NFPA 101 life-safety reviews
- Prepare pharmacy and CLIA lab approvals
- Finish bylaws, credentialing, and emergency plans
- Confirm details with counsel and regulators
How long does it take to open a hospital?
A new acute care Hospital usually takes 18–36+ months to open because approvals, construction, equipment, staffing, surveys, payer enrollment, and first-admission readiness all move in linked workstreams. The real schedule is set by the slowest approval, not the ribbon-cutting date. If you’re buying an existing site, it can move faster when license transfer, facility compliance, and payer participation are already usable.
What slows opening
- Certificate of Need review can add months
- Site approval can stall the build
- Life-safety corrections delay surveys
- EHR implementation and credentialing take time
What can move faster
- Acquisition can skip some build time
- License transfer can speed launch
- Phased opening uses fewer departments
- Payer contracting must still be ready
How do hospitals get their first patients?
A Hospital gets its first patients only after approved service lines are open, access workflows are live, clinicians are credentialed, and payer enrollment is set so billing can start; for cost context, see How Much Does It Cost To Open A Hospital?. First patients usually come from physician referrals, emergency access where allowed, transfer relationships, community awareness, and employer or payer relationships. Year 1 planning should expect capacity at 65% for surgeons, 70% for ER physicians, 68% for specialists, 60% for radiologists, and 72% for physical therapists.
Where patients come from
- Physician referrals drive early volume.
- Emergency access brings urgent cases.
- Transfer links feed inpatient admits.
- Employer and payer ties build demand.
What makes revenue start
- Admission or encounter must occur.
- Care must be documented.
- Charge capture and coding must run.
- Claims need submission and denial follow-up.
Confirm the hospital is safe, licensed, staffed, and revenue-ready before opening
Launch readiness checklist
Use this go-live approval checklist to confirm the hospital is ready before opening.
Compliance
- State hospital license approvedCritical
No opening without the core hospital license and state operating approval.
- Certificate of Need clearedCritical
Where required, this gate blocks site spend before regulators bless the plan.
- CMS or accreditation pathway setHigh
A clear CMS or accreditation path is needed before billing and inspections start.
Facility
- Patient rooms readyCritical
Beds, care areas, and circulation must work before the first patient arrives.
- Emergency systems testedCritical
Backup power, alarms, and critical systems protect patients in month one.
- Accessibility and infection control clearedHigh
Access routes, sanitation, and isolation controls must pass before go-live.
Systems
- EHR workflows testedCritical
Order entry, charting, and discharge steps must work end to end before launch.
- Imaging and lab installedHigh
Imaging and lab links must be live so diagnostics do not stall care.
- Medication administration flows passCritical
Medication handoff needs a safe path from order to bedside.
Vendors
- Medical supplies stockedCritical
Supplies and disposables must be on hand before the first admissions wave.
- Pharmaceuticals contracts liveCritical
Medication supply gaps can stop treatment and delay discharge.
- Waste, cleaning, security setHigh
Support vendors need active service levels for waste, cleaning, and security.
Staffing
- 85 Year 1 providers confirmedCritical
The Year 1 plan totals 85 providers across five groups, so gaps hit access fast.
- Credentialing files completeCritical
No one should start without current license, credentialing, and payer files.
- Privileges and call coverage setHigh
Shift, on-call, and handoff coverage must be locked before opening.
Revenue
- Referral network and transfers activeHigh
If referrals and transfer paths are weak, beds sit empty at launch.
- Payer enrollment and contracts readyCritical
Claims cannot flow without payer enrollment and clean contract terms.
- Opening-month model signed offCritical
The model should absorb $475k fixed overhead before payroll and the 195% Year 1 supply load.
Want to see the six hospital launch drivers?
1Regulatory Path
18–36+ moLicenses, Certificate of Need, and survey approval decide whether opening can happen at all.
2Life-Safety Readiness
Pass inspectPassed inspections and tested systems clear the building for admissions and first care.
3Clinical Staffing
85 providersYear 1 needs 85 providers credentialed and scheduled, or beds sit idle and openings slip.
4Clinical Systems
Day 1 EHREHR, orders, meds, lab, and discharge workflows must work before the first patient arrives.
5Payer Cycle
$86M/moClean enrollment, coding, and claims flow turn roughly $86M monthly charges into cash.
6Patient Ramp
60%–72%Referrals and transfer paths drive volume; Year 1 capacity ranges from 60% radiology to 72% PT.
Regulatory Pathway
Regulatory Pathway
A hospital cannot open without approvals, so this is a hard go/no-go gate, not a soft milestone. The launch plan has to fit the 18–36+ month approval window, or opening slips even if construction and staffing are done. The key readiness signal is a clear path on the state license, Certificate of Need where required, CMS or accreditation plan, local approvals, survey binder, and governing documents.
Here’s the quick math: if any one approval is late, the whole opening date moves. That risk is highest when facility design, staffing, emergency preparedness, and clinical policies are not sequenced early. One clean line: no approvals, no patients.
- Map the license sequence first.
- Confirm CON status early.
- Build the survey binder fast.
- Lock medical staff bylaws.
Build the approval path first
Start with application sequencing, then write the policies, bylaws, and inspection prep around it. The hospital also needs emergency preparedness, staffing plans, and clinical policies ready before survey and licensing review. If these pieces sit in different workstreams, approval timing becomes the bottleneck and cash burn continues while the opening date stays uncertain.
Track each dependency like a launch task: facility design, staffing, local approvals, and the CMS or accreditation path. What this estimate hides is rework risk; if one document is off, the review cycle can reset. Keep a single owner on the approval calendar and test every required file before submission.
- Assign one approval owner.
- Test every required document.
- Align design with survey needs.
- Do not assume timing is flexible.
1
Facility and Life-Safety Readiness
Facility and Life-Safety Readiness
The hospital cannot open on time unless patient rooms, clinical departments, utilities, emergency power, fire safety, accessibility, and infection-control systems all pass inspection and work on day one. If the life-safety review fails or the punch list stays open, admissions slip, staff wait, and the first day of care gets delayed.
This is the bridge between construction and real operations. Equipment install, department stocking, and survey clearance must line up with the opening date, or you end up with rooms that look done but still can’t take patients. That delay also pushes cash needs up, because payroll, utilities, and vendor bills keep running before revenue starts.
Commission Before You Stock
Run the opening checklist in order: commissioning, infection-control checks, equipment validation, and emergency drills. Tie each step to construction completion, vendor installs, and the survey window so the launch date stays realistic.
- Clear the punch list first.
- Test backup power and alarms.
- Stock only approved departments.
- Verify room workflows on site.
- Document every pass and fix.
Watch for the common trap: equipment arrives before the room is approved, or the room is approved before the workflow is tested. Either way, the hospital may look close to ready but still fail to admit patients safely.
2
Clinical Staffing and Credentialing
Clinical Staffing
This hospital cannot open beds or service lines until licensed people are hired, credentialed, privileged, scheduled, and trained. The Year 1 plan totals 85 clinicians across 15 surgeons, 25 ER physicians, 20 specialists, 10 radiologists, and 15 physical therapists, so any gap here pushes opening dates and cuts day-one capacity.
Here’s the quick math: if even one core role is missing, call coverage, department leadership, nursing schedules, and orientation records can slip. That raises early cancellation risk and makes the first patient ramp less safe, especially when service-line scope, survey readiness, and EHR access all need to line up before launch.
Hire, Privilege, Train
Build the launch plan around complete credentialing files, privileging, onboarding, staffing ratios, and simulation training. The readiness check is simple: every scheduled clinician should be cleared, assigned, and trained before the first booked case or shift.
- Lock hiring against service-line scope.
- Finish privileging before scheduling.
- Confirm call coverage by department.
- Document orientation and simulation completion.
- Test staffing plans with EHR access live.
What this estimate hides is timing risk. If credentialing runs long, the hospital may have rooms ready but no safe way to staff them, which forces delayed openings, thinner coverage, and more first-week cancellations.
3
Clinical Systems and Workflows
Clinical Systems Must Work First
Day-one safety depends on the EHR, order sets, admissions, medication administration, lab, imaging, discharge planning, infection control, quality reporting, and emergency preparedness all working before the first patient arrives. If these pieces are built but not tested together, the hospital can open late or, worse, open with unsafe gaps in care flow.
The real gate is not build completion. It is tested workflows, trained users, and downtime procedures that hold up in a full mock patient journey. One missed handoff between departments can delay meds, lab results, or discharge orders, and that hits both patient safety and first-day throughput.
Test the Whole Patient Path
Verify the EHR build, department protocols, pharmacy and lab interfaces, and documentation templates in the same sequence patients will use them. A hospital should not count a workflow as ready until admissions to discharge has been run end to end, including emergency backup steps and role-based training.
Track the launch risks tied to staffing, payer setup, and vendor readiness, because those dependencies can stall system sign-off even after software is installed. The bottleneck is usually not the build itself; it is the first cross-department test when nursing, pharmacy, lab, imaging, and case management all have to work together.
- Run mock patient journeys before opening.
- Train every user on downtime steps.
- Confirm lab and pharmacy interfaces.
- Document who owns each handoff.
4
Payer Enrollment and Revenue Cycle
Payer Enrollment and Revenue Cycle
Cash timing is the launch issue here. Care only turns into revenue after documentation, coding, charge capture, claim submission, and collection all work. The hospital can see patients on day one, but without payer enrollment and contract setup, cash can lag while volume looks fine.
With modeled Year 1 gross monthly service revenue of about $86M before payer adjustments, even a 1% break in claims or denials is about $860k of monthly cash at risk. One clean claim path matters more than headline charges.
Ready the claim path first
Verify Medicare provider enrollment, commercial payer setup, billing rules, claim edits, denial handling, and cash posting before opening. The readiness signal is live payer enrollment, signed contracts, clean-claim testing, and EHR charge rules that match the coders’ work.
- Match provider records to enrollment files.
- Test clean claims in the EHR.
- Load coding protocols and charge rules.
- Assign denial follow-up and cash posting.
- Confirm licensure and EHR setup first.
If enrollment slips, patients still show up, staff still work, and cash still waits. That pushes working capital needs up fast and can force delayed billing, manual workarounds, and slow first-month collections.
5
Referral Network and Patient Ramp
Referral Network and Patient Ramp
This launch driver is about volume on day one. A hospital can open its doors and still miss first-month revenue if referral physicians, transfer partners, and payer channels are not already sending patients through a trusted access path. Broad advertising won’t fill beds fast enough; the referral intake, call center, and scheduling flows have to be live before opening.
The risk is uneven ramp by service line. Year 1 capacity assumptions run from 60% for radiology to 72% for physical therapy, so staffing and appointment books need to match expected demand by department. If approved services, credentialed clinicians, and payer participation are not in place, first admissions slow down and cash comes in later than planned.
Build the access paths before opening
Set up referral physician outreach, transfer agreements, employer relationships, and payer relationships before launch week. Then test the full path: referral intake, patient access, scheduling, and discharge follow-up. If a referred patient cannot be booked fast, the hospital may still be “open” but not functionally ready.
- Confirm service lines are approved.
- Verify clinicians are credentialed.
- Test referral intake end to end.
- Map staffing to each department’s ramp.
- Track no-show and hold times daily.
One clean rule: no access path, no ramp. If the community launch plan is weak or scheduling rules are slow, the first revenue weeks lag even when the beds, rooms, and equipment are ready.
6
Related Products
- Hospital Porter's Five Forces Analysis
- Hospital BCG Matrix
- Hospital Business Model Canvas
- Monitor Key Performance Metrics for Hospital Profitability
- Hospital Business Plan Template in Pre-Written Word
- Increase Hospital Profitability: 7 Strategies for Margin Growth
- How Much Does It Cost To Run A Hospital Each Month?
- Hospital Startup Costs: $28M+ CAPEX Before Staffing And Runway
- Hospital Financial Model Template in Excel
- How Much Does a Hospital Owner Make? $751M Pre-Debt Cash Flow
- How to Write a Hospital Business Plan: 7 Essential Steps
- Hospital Marketing Mix
- Hospital Marketing Plan
- Hospital Business Proposal
- Hospital PESTEL Analysis
- Hospital Pitch Deck Example Editable PPTX
- Hospital Business SWOT Analysis
- Hospital Value Proposition Canvas
Frequently Asked Questions
Yes, private hospitals can operate in the US, but opening depends on state licensure, Certificate of Need rules where applicable, facility inspections, Medicare certification or accreditation path, and payer enrollment For a new acute care facility, plan around an 18–36+ month launch window and prove staffing, life-safety, EHR, and billing readiness before first admissions