 Owner income$80.1M–$264.2M
Owner income$80.1M–$264.2MHow Much Does a Hospital Owner Make? $751M Pre-Debt Cash Flow

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Owner income$80.1M–$264.2M  Net margin78%–83%
Net margin78%–83% Revenue for target pay$103.1M–$319.9M
Revenue for target pay$103.1M–$319.9M Business difficultyHard
Business difficultyHard


Key Takeaways
- Payer mix drives collectable revenue, not billed charges.
- Volume helps only when reimbursement beats variable costs.
- Labor efficiency protects margin; agency staff can erase it.
- Debt, capex, and reserves cut owner cash.
Owner income$80.1M–$264.2MNet margin78%–83%Revenue for target pay$103.1M–$319.9MBusiness difficultyHardWant to test your hospital owner income?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. Actual owner income depends on revenue, margins, payroll, taxes, debt, and reinvestment. It is not guaranteed salary, tax advice, or owner distribution advice. This model also excludes regulatory approvals, nonprofit limits, financing terms, and Medicare or Medicaid rule changes.
Want to check owner income in the Hospital financial model?
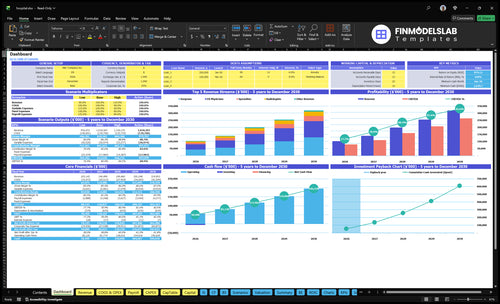
This dashboard shows owner-income outputs, revenue build, margin bridge, staffing, fixed costs, debt service, reserve logic, and scenario charts. Open the Hospital Financial Model Template.
Owner-income model highlights
- EBITDA and cash flow
- Separate service line revenue
- Clinician and volume assumptions
- Reserve and reinvestment logic
How much revenue is needed to pay a hospital owner?
There’s no single revenue number for a Hospital; the right way is to back into owner pay from distributable cash, not guess from gross sales. Add owner pay, debt service, taxes, reserves, and reinvestment, then divide by operating margin to get required net patient revenue. Using the provided Year 1 margin, $10M of target pre-debt cash needs about $137M of revenue, and bed count, payer mix, occupancy, service lines, denials, and staffing all move that target.
Back into cash first
- Start with owner pay.
- Add debt service and taxes.
- Include reserves and reinvestment.
- Divide by operating margin.
What changes the target
- $10M cash can mean $137M revenue.
- Bed count changes scale fast.
- Payer mix changes collections.
- Occupancy and denials shift margin.
Is owning a hospital profitable?
Hospital ownership can be profitable, but it is not passive income. Profit depends on regulatory compliance, physician relationships, managed-care contracts, payer mix, quality metrics, capital intensity, and owner role. The supplied case shows strong pre-debt, pre-tax cash flow, but no debt service, reserve requirement, tax load, capital expenditure schedule, or license approval cost is provided.
Profit drivers
- Managed-care contracts set pricing power.
- Payer mix changes the cash picture.
- Quality metrics support referrals and reimbursement.
- Active owners need strong revenue cycle control.
Key risks
- Compliance gaps can hurt the license fast.
- Capital needs stay heavy and ongoing.
- Investor-only owners still carry liquidity risk.
- Clinical governance must stay tight.
How do hospital profit margins affect owner income?
At $1,031M of Year 1 revenue, a 1-point margin swing is about $10M in annual EBITDA, so Hospital owners feel even small changes fast. The cost path is also telling: direct costs fall from 195% in Year 1 to 161% in a mature year, while visible payroll rises from $222M to $301M. For the full setup math, see How Much Does It Cost To Open A Hospital?
Margin drivers
- Reimbursement moves revenue fast
- Staffing ratios change labor cost
- Agency labor can spike spend
- Supply pricing hits margin directly
Margin controls
- Uncompensated care cuts cash yield
- Claim denials delay collections
- Collection timing affects cash flow
- Protect safe staffing and quality
Want the six main hospital income drivers?
1
$700-$22.5KPayer Mix
Higher reimbursement on surgery and other high-acuity cases lifts take-home far faster than low-rate visits.
2
668-770/moPatient Volume
More treatments per month spread fixed costs and push EBITDA up.
3
111xService Mix
A heavier case mix toward surgery and imaging raises revenue per encounter.
4
60%-88%Labor Efficiency
Better staffing and capacity use keeps payroll from outrunning case growth.
5
1 moRevenue Cycle
Faster billing and fewer denials turn earned revenue into cash sooner.
6
$1.64MCapital Load
The opening cash floor and equipment spend decide how much profit stays usable.
Hospital Core Six Income Drivers
Payer Mix and Reimbursement
Payer Mix
Payer mix controls how much billed care turns into cash. Use net patient revenue, not gross charges: commercial, Medicare, Medicaid, self-pay, and uncompensated care each collect at different rates. In this model, Year 1 is $1,031M and mature year is $3,200M before payer-specific adjustments, so a stronger commercial mix lifts owner income faster than the same visit volume with more self-pay.
The risk is slower collections, more denials, and higher accounts receivable. A hospital can add surgeries and still miss cash targets if the mix shifts toward low-paying or unpaid cases. Here’s the quick math: a 1% collection swing on $1,031M changes cash by about $10M, which can decide whether there is room for owner distributions.
Track Cash by Payer
Measure net patient revenue by payer, denial rate, charity care, self-pay share, and days in accounts receivable. The key inputs are commercial share, Medicare share, Medicaid share, self-pay share, and uncompensated care. More commercially reimbursed surgeries can lift cash faster than higher self-pay emergency volume, even when total volume looks strong.
- Commercial mix by service line
- Denial rate by payer
- Days in AR trend
- Self-pay and charity care share
Tighten authorization, coding, and denial work before chasing more volume. Add cases only when reimbursement clears direct labor, supplies, and capacity cost, so added visits support cash flow instead of tying up working capital. If reimbursement lags, owner pay usually slips next.
1
Occupancy and Patient Volume
Occupancy and Patient Volume
Occupancy and patient volume means how many beds and service slots the hospital fills across inpatient and outpatient care. In this model, capacity runs at 600% to 720% in Year 1 and 780% to 880% in a mature year, with monthly revenue rising from $86M to $267M. More volume lifts income only when added reimbursement beats staffing, supplies, and capacity costs.
Track licensed beds, average daily census, admissions, emergency visits, surgeries, radiology studies, and outpatient visits. If volume needs agency staff, extra call coverage, or new equipment, owner pay can shrink even as revenue grows. The quick rule is simple: fill capacity with profitable cases, not just more cases.
Measure Volume Profitably
Test each service line on net revenue per visit and contribution after variable cost. Compare the extra reimbursement against direct labor, supplies, and any added room, machine, or coverage cost before you push volume higher. If a line cannot clear its own variable cost, it is busy but not useful for profit.
Use a weekly dashboard with these inputs:
- Licensed beds and average daily census
- Admissions and emergency visits
- Surgeries and radiology studies
- Outpatient visits
- Agency labor, overtime, and equipment adds
Set a floor for added staffing or equipment, then slow growth when margin weakens. That keeps cash available for bills, debt, and owner distributions.
2
Service-Line Mix and Acuity
Service-Line Mix
Service mix changes both revenue and margin. In Year 1, surgery is $421M, emergency is $378M, specialty is $114M, radiology is $90M, and physical therapy is $28M. The owner wins only when higher-paying lines cover their extra cost load, including staff, equipment, call coverage, and quality controls. Otherwise, volume just adds work, not take-home income.
Model each line on its own. Emergency, imaging, maternity, surgery, specialty, outpatient, and medical-surgical care should not be blended together, because each one uses different labor, supplies, and capacity. Incremental reimbursement must beat direct costs and capacity costs before owner pay improves. That is the core test, not gross revenue alone.
Track Margin by Line
Use service-line contribution margin to see what really pays. Track volume, price, direct labor, supplies, credentialing, call pay, and equipment cost for each line. Here’s the quick math: if a line adds revenue but also forces new coverage or specialized staff, the extra cash can shrink fast. What this estimate hides is the fixed cost of keeping the service open.
- Track revenue by service line.
- Track direct cost by service line.
- Separate fixed from variable capacity costs.
- Test whether margin clears added coverage.
- Keep the highest-yield lines staffed first.
If a line needs expensive staffing or equipment, don’t chase it just for top-line growth. Owner income improves only when the mix shift lifts contribution margin after all direct and capacity costs are paid. That is where the cash for distributions comes from.
3
Clinical Labor Efficiency
Clinical Labor Efficiency
Hospital income depends on labor staying safe and tight. Payroll rises from $222M in Year 1 to $301M in the mature year, a jump of about $79M or 36%. That includes the $400,000 Chief Medical Officer and $300,000 Hospital Administrator. If nurse ratios, physician coverage, and department heads run hot, owner income drops fast.
Here’s the quick math: more census only helps when labor per case stays controlled. Benefits, overtime, and agency labor can wipe out margin even when volume rises. So the real test is whether staffing supports safe care at the lowest workable mix, not whether payroll looks lean on paper.
Track Labor Per Case
Measure nurse ratios, physician coverage, overtime hours, agency hours, and benefits by department. Tie each one to census and case mix so you can see where labor cost rises faster than patient volume. That shows whether added revenue is paying for itself or just funding more shift fill.
Watch agency nursing first. It is the fastest way to lose margin when demand spikes. Build staffing plans that protect safety, then compare budgeted payroll of $222M to the mature-year run rate of $301M so you can spot cost creep before it hits owner draw.
- Track overtime by unit.
- Separate agency from core staff.
- Model physician coverage daily.
- Review admin headcount monthly.
4
Revenue Cycle and Bad Debt
Collected Cash, Not Charges
Revenue cycle is the path from care to cash: coding, authorization, billing accuracy, denial work, collections, charity care, self-pay, and accounts receivable days. Owner pay tracks collected revenue, not billed charges. With $1,031M in Year 1 revenue, even a 1% collection swing moves cash by about $10M.
Here’s the quick math: if claims sit unpaid, cash arrives late and distributions shrink even when volume is strong. The main risk is good clinical throughput with weak timing, rising bad debt, and more write-offs. That can squeeze margins and force the owner to wait on draws until payers and patients actually pay.
Track Denials, Days, and Self-Pay
Measure the pieces that convert work into cash: clean-claim rate (claims paid without edits), denial rate, authorization hits, collection rate, charity care, self-pay exposure, and A/R days. Track them by service line and payer, because surgery, emergency, and specialty claims can behave very differently. If one line drives bad debt, it can erase the cash gain from higher census.
- Watch collected revenue weekly.
- Break out denials by cause.
- Age A/R by payer.
- Cap self-pay leakage early.
Use the data to test fixes: tighter coding, faster follow-up, clearer patient bills, and faster denial appeals. The goal is simple: shorten the cash lag so operating profit turns into owner distributions instead of sitting in receivables.
5
Debt Service, Capex, and Reserves
Debt, Capex, and Reserves
A hospital can show profit and still produce little owner cash. After operating costs, you still need to fund debt service, capital expenditures (capex), and reserves before any owner draw. The model’s disclosed source fixed costs are $475,000 per month, or $57M per year, for lease, utilities, EHR and medical record systems, insurance, security, cleaning, waste, and software.
Here’s the quick math: owner pay = collected cash - operating costs - debt service - capex - reserves. No debt service, capex, or reserve amount is provided, so those must be modeled as separate cash claims. If equipment replacement, accreditation work, or tech upgrades rise, distributable cash falls fast, even when patient volume and margin look healthy.
Model the cash waterfall
Track each cash bucket separately so profit does not get confused with cash you can pay out. Start with collected revenue, then subtract the disclosed fixed run-rate of $475,000 per month, plus any loan payments, equipment purchases, compliance costs, and reserve deposits. If you skip this, owner draws will look real on paper but disappear in the bank account.
- List debt payment dates and amounts.
- Schedule equipment replacement by year.
- Set a reserve target in months.
- Separate maintenance from growth capex.
- Update the draw only after funding all buckets.
6
Objective: Compare low, base, and high hospital owner income scenarios
Owner income scenarios
Owner income swings with treatment volume, payer mix, staffing, and capital load. Higher capacity can lift EBITDA, but debt, taxes, reserves, and reinvestment still cut take-home.
| Scenario | Low CaseVolume risk | Base CaseCore plan | High CaseUpside case |
|---|---|---|---|
| Launch model | This is the lower earnings path if volume stays below plan and take-home tracks the first-year build. | This is the modeled middle path if the hospital hits the Year 3 operating plan. | This is the stronger earnings path if utilization, pricing, and capacity all run above the base plan. |
| Typical setup | Year 1 assumptions: $1,031M revenue, 195% direct costs, $57M fixed costs, $222M visible payroll, and $751M EBITDA before debt, taxes, reserves, and reinvestment. | Year 3 assumptions: $1,995M revenue, 178% direct costs, $57M fixed costs, $268M visible payroll, and $1,556M EBITDA before debt, taxes, reserves, and reinvestment. | Mature-year assumptions: $3,200M revenue, 161% direct costs, $57M fixed costs, $301M visible payroll, and $2,597M EBITDA before debt, taxes, reserves, and reinvestment. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $751M proxyLower take-home | $1,556M proxyPlanning anchor | $2,597M proxyUpside test |
| Best fit | Use this to stress-test slower ramp, payer mix pressure, and early staffing strain. | Use this as the main operating case for budgeting, hiring, and lender talks. | Use this to test upside from fuller beds, better throughput, and tighter cost control. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Hospital Porter's Five Forces Analysis
- Hospital BCG Matrix
- Hospital Business Model Canvas
- Monitor Key Performance Metrics for Hospital Profitability
- Hospital Business Plan Template in Pre-Written Word
- Increase Hospital Profitability: 7 Strategies for Margin Growth
- How Much Does It Cost To Run A Hospital Each Month?
- Hospital Startup Costs: $28M+ CAPEX Before Staffing And Runway
- Hospital Financial Model Template in Excel
- How to Open a Hospital: 18–36+ Month Launch Roadmap
- How to Write a Hospital Business Plan: 7 Essential Steps
- Hospital Marketing Mix
- Hospital Marketing Plan
- Hospital Business Proposal
- Hospital PESTEL Analysis
- Hospital Pitch Deck Example Editable PPTX
- Hospital Business SWOT Analysis
- Hospital Value Proposition Canvas
Frequently Asked Questions
A hospital owner can take home only the cash left after debt, taxes, reserves, and reinvestment In this planning case, Year 1 revenue is $1031M and EBITDA is $751M before those deductions Mature-year EBITDA reaches $2597M Those are not guaranteed distributions