Hospital Startup Costs: $28M+ CAPEX Before Staffing And Runway

This hospital startup cost breakdown covers known CAPEX of at least $28M for magnetic resonance imaging, computed tomography, and electronic health record implementation across the first 9 months, plus facility, regulatory, staffing, supplies, and working capital assumptions The model period runs Month 1 to Month 60, with Year 1 staffing capacity built around 15 surgeons, 25 emergency department physicians, 20 specialists, 10 radiologists, and 15 physical therapists These are planning assumptions, not vendor quotes, appraisals, financing terms, or regulatory guarantees
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates capitalized startup assets only for a hospital, using facility buildout, equipment, IT, furniture, and contingency.
CAPEX only Excludes inventory, working capital, pre-opening payroll, debt service, lease payments, deposits, financing fees, and post-opening cash burn. Add those in separate funding lines if needed.
What does the Hospital CAPEX tab show?
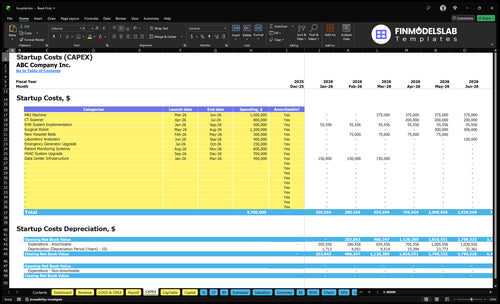
Screenshot shows Hospital Financial Model Template CAPEX tab lists startup costs, Month 1–60 timing, depreciation, amortization, and funding. Review assumptions.
CAPEX screenshot highlights
- $15M MRI CAPEX
- $800k CT CAPEX
- $500k EHR setup
- Surgical robot timing
- Working capital, funding
- $25M payroll, 195% variables
- $475k fixed costs
- Provider revenue ramp
What is the biggest hospital startup cost?
For a Hospital startup, the biggest cost is usually facility development, with medical equipment close behind. New construction, acquisition, renovation, and adaptive reuse can swing the budget a lot because utility, life-safety, and code work change fast. Here’s the quick math: one MRI unit can cost about $15M, a CT scanner about $800k, and an EHR implementation about $500k.
Facility cost drivers
- New build costs the most
- Code and safety upgrades add up
- Adaptive reuse still needs heavy work
- Location and layout change the budget
Equipment budgets
- Imaging drives large spend fast
- Surgical and emergency need separate budgets
- Lab, pharmacy, and sterilization need their own funds
- Small licenses are not the main issue
How much money do you need to open a hospital?
To open a Hospital, plan around the total funding need, not just construction: the known hard-cost floor is $28M before facility buildout and before the surgical robot amount. Add early liquidity of about $2.05M for three months of fixed overhead plus leadership payroll, and pressure-test the plan against What Is The Most Critical Measure Of Success For Your Hospital? because bed count, service mix, location, payer mix, and ownership model can move the requirement fast.
Base Funding Stack
- Start with $28M hard-cost floor
- Add facility CAPEX and buildout
- Add clinical equipment and health IT
- Add regulatory readiness and supplies
Liquidity Cushion
- Fixed overhead: $475k/month
- Leadership payroll: $208k/month
- Three-month cushion: $2.05M
- Excludes clinical labor and collections lag
What hidden hospital startup costs are easy to miss?
If you’re budgeting a hospital, the easy-to-miss costs are the non-CAPEX items: pre-opening payroll, physician credentialing, payer contracting, accreditation prep, insurance binders, compliance consulting, architectural review, biomedical testing, supply stocking, EHR training, cybersecurity setup, and working capital runway. See How Much Does The Owner Of A Hospital Typically Make? for the revenue side, because the cost side can hit before patient volume does. $475k in monthly fixed overhead, plus $75k insurance, $50k utilities, and $30k EHR support, means runway matters fast; Year 1 leadership payroll is $25M, and Year 1 variable costs total 195% of revenue.
Hidden setup costs
- Pre-opening payroll starts before revenue.
- Credentialing and payer setup take time.
- Accreditation and compliance add real cash burn.
- Training, testing, and stocking are not optional.
Runway pressure
- $475k monthly fixed overhead is heavy.
- $75k insurance and $50k utilities stack up.
- $30k EHR support keeps cash moving out.
- 195% variable costs can outpace early revenue.
Calculate Fuding Needs
Startup Cost Summary
This table summarizes the main hospital startup CAPEX items and the excluded opening cash buffer.
| Cost Category | Base Estimate | Main Cost Driver | CAPEX Calculator |
|---|---|---|---|
| MRI Machine | $1,500,000 | Equipment price and installation scope | Yes |
| Surgical Robot | $1,200,000 | Device price and integration scope | Yes |
| CT Scanner | $800,000 | Scanner price and setup scope | Yes |
| EHR System Implementation | $500,000 | Software implementation and setup scope | Yes |
| Data Center Infrastructure | $450,000 | Servers, storage, and network buildout | Yes |
| Opening Cash Buffer | $1,640,000 | Minimum cash needed to cover early operating losses | No |
Hospital Core Five Startup Costs
Facility Development Startup Expense
Build Scope
This line covers land or building acquisition, leasehold improvements, site work, construction, and renovation. A new build usually needs more money than leasing an existing shell, but it may better fit clinical-grade utilities, backup power, oxygen and medical gas, fire systems, OR space, patient rooms, imaging shielding, and code compliance. It excludes medical equipment and payroll.
Lease Load
Under the source lease assumption of $250k per month from Month 1 to Month 60, rent totals $15M before build-out, deposits, or tenant work. If you buy or lease an existing facility, this can be the biggest fixed cash drain while the rest of the scope gets completed.
Sizing Inputs
I need bed count, square footage, service lines, operating rooms, state code constraints, and whether the facility is already licensed. Those inputs drive the size of the shell, the amount of emergency department access, and the level of accessibility, shielding, and life-safety work.
- Bed count
- Square footage
- Service lines
- Operating rooms
- State code constraints
- Licensed already?
Cost Control
To control cost without hurting compliance, reuse an existing facility only when the room sizes, access, and code path already match the plan. The usual misses are underbudgeting fire and life-safety, backup power, and medical gas. One clean rule: if the site cannot pass the clinical workflow, it is not a cheap site.
Medical Equipment And Department Setup Startup Expense
Department split
Don’t pack equipment into one line. Split it by service area: hospital beds, monitors, surgical gear, imaging, lab, emergency department, pharmacy, sterilization, rehabilitation, and biomedical testing. That makes the budget match the care mix, and it shows where you should buy versus lease instead of guessing on one blended number.
MRI and CT timing
Here’s the hard CAPEX: $15M for magnetic resonance imaging from Month 3 to Month 6, and $800k for computed tomography from Month 4 to Month 7. The surgical robot lands from Month 5 to Month 8, but no dollar amount was provided, so keep it as a timing item only.
- Use vendor quotes by department
- Match spend to go-live month
- Keep robot cost unpriced
Build the estimate
Estimate each department with units × unit price, then add install, testing, and coverage months. Ask for quotes on each asset class, plus ownership terms for lease or purchase. The main inputs are service mix, bed count, imaging volume, lab scope, ED load, and rehab demand. One line item hides the real cost shape.
- Separate capital from leased gear
- Quote each department alone
- Track install and test dates
Keep quality tight
To hold down startup cash without hurting care, phase purchases by launch order and avoid buying unused capacity early. Tie imaging, lab, and OR equipment to the first months of service, then compare lease versus ownership by asset life and usage. What this estimate hides is support gear, service contracts, and downtime risk.
Health IT And EHR Startup Expense
EHR Launch Cost
For a hospital, the electronic health record is a launch cost, not a nice-to-have. The base build is $500k from Month 1 to Month 9, then $30k a month for support and $10k a month for admin software. That money keeps registration, billing, clinical notes, meds, lab and imaging links, and reporting working together.
Cost Inputs
Build the estimate from implementation fee, monthly support, and go-live work. Include training, interface testing, data migration, user access controls, downtime procedures, and go-live support. Ask for quote terms, number of users, interfaces, and months of coverage. Base cash need through Month 9 is $860k = $500k + 9 × $40k.
- Implementation fee
- Monthly support months
- Users and interfaces
Trim Waste
Trim waste by staging rollout in waves, locking interface scope, and testing downtime before go-live. Do not cut training or access controls; those mistakes slow billing and can delay cash. The safest savings come from reducing extra interfaces and avoiding change orders.
- Phase noncritical interfaces first
- Train super users early
- Lock scope before go-live
Claims-Cash Risk
If setup slips, claims hit the payer late and cash gets trapped in work queues. Registration errors, coding delays, and failed lab or imaging links can slow reimbursement fast. Treat user access, downtime drills, and go-live support as controls that protect revenue, not extras.
Licensing, Accreditation, And Professional Services Startup Expense
What It Covers
This line covers state hospital licensing, Certificate of Need work where required, Medicare enrollment, accreditation prep, survey readiness, legal counsel, architectural review, compliance consulting, payer contracting, revenue cycle setup, policies, and clinical governance. It is a regulatory and advisory cost, not construction or equipment CAPEX, so it should sit beside launch fees in the opening budget.
How To Estimate
Estimate it from facility type, bed count, service lines, ownership structure, and whether the hospital seeks Medicare participation. Ask for separate quotes for legal, compliance, architecture, payer setup, and revenue cycle work. One clean rule: tie scope to the license package, not to bricks and equipment, or you’ll blur fixed launch costs with buildout spend.
How To Control Cost
Use one local healthcare attorney and one lead compliance advisor, then keep all reviewers on the same scope sheet. That cuts duplicate work, but don’t trim survey prep or policy buildout just to save cash. The big savings come from clear scope, early state review, and getting payer and revenue cycle setup aligned before opening, so rework stays low.
State-Specific Drivers
Costs swing hard by state rules. A hospital with more beds, more service lines, or complex ownership usually needs more legal, architectural, and compliance hours, plus more policy work before any survey. Approval is not guaranteed, and neither is survey success, so budget for extra rounds of document review, mock readiness checks, and state-specific filings.
Pre-Opening Payroll And Staffing Startup Expense
Payroll Scope
Pre-opening payroll is separate from post-launch labor. It covers executive hires, clinical leadership, physicians or contracted staff, nurses, technicians, radiology, lab, pharmacy, revenue cycle, administration, recruiting, credentialing, onboarding, and training. Year 1 leadership payroll totals $25M, including $400k CMO, $300k hospital administrator, $600k department heads, $650k head nurses, and other core leaders.
Budget Inputs
Model this as headcount times months of pre-open coverage, plus contract labor and training time. Tie the ramp to Year 1 capacity across 15 surgeons, 25 emergency physicians, 20 specialists, 10 radiologists, and 15 physical therapists. Add recruiting, credentialing, onboarding, and go-live support before first patient.
Cost Control
The safest cut is timing , not coverage. Hire leaders first, then stage clinical and support teams as licensing, EHR work, and service-line readiness lock in. Don’t carry full payroll too early; every extra month before launch adds another payroll run and raises cash burn.
Ramp Timing
Sequence hiring to the launch calendar, not the full org chart. Put the earliest dollars into credentialing, onboarding, and training, then open each service line only when staffing and patient flow are ready.
Compare 3 Startup Cost Scenarios
Hospital launch scenarios
Hospital startup cost swings with bed count, service mix, equipment, and staffing speed. Lean, Base, and Full show how a tighter footprint lowers cash need while a broader acute-care build pushes it up.
| Scenario | Lean LaunchSpecialty build | Base LaunchModel aligned | Full LaunchHigh capex |
|---|---|---|---|
| Launch model | Lean launch starts with a specialty-led site, fewer beds, and limited imaging, so the upfront build stays lighter but the service mix is narrower. | Base launch follows the source model with multi-service care, known high fixed overhead, and a Year 1 provider capacity that matches the planned clinical mix. | Full launch adds broader acute-care services, more operating rooms, heavier equipment, and a larger clinical team, so capital demand rises fast. |
| Typical setup | Use a leased or smaller facility, one to two service lines, basic diagnostics, and a smaller Year 1 staffing ramp with about 3-4 months of working capital. | Use a full hospital footprint, core imaging, several service lines, and a steady staffing ramp with about 6-9 months of working capital. | Use a larger bed count, broader service lines, heavier imaging and surgical equipment, and a bigger staff ramp with about 9-12 months of working capital. |
| Cost drivers |
|
|
|
| Planning rangeCAPEX only | $8M - $15MLower cash need | $25M - $35MMiddle band | $45M - $75MHighest need |
| Best fit | Best for founders testing one focused care line, but it leaves less room for broad acute-care demand. | Best for operators building a multi-service hospital with enough capital to fund the first ramp and absorb payer timing. | Best for well-funded groups that want a broad hospital platform and can carry the cost of bigger equipment and staffing. |
Planning note: These ranges are researched planning assumptions, not vendor quotes, and should be checked against local lease, labor, and equipment bids.
Related Products
- Hospital Porter's Five Forces Analysis
- Hospital BCG Matrix
- Hospital Business Model Canvas
- Monitor Key Performance Metrics for Hospital Profitability
- Hospital Business Plan Template in Pre-Written Word
- Increase Hospital Profitability: 7 Strategies for Margin Growth
- How Much Does It Cost To Run A Hospital Each Month?
- Hospital Financial Model Template in Excel
- How Much Does a Hospital Owner Make? $751M Pre-Debt Cash Flow
- How to Open a Hospital: 18–36+ Month Launch Roadmap
- How to Write a Hospital Business Plan: 7 Essential Steps
- Hospital Marketing Mix
- Hospital Marketing Plan
- Hospital Business Proposal
- Hospital PESTEL Analysis
- Hospital Pitch Deck Example Editable PPTX
- Hospital Business SWOT Analysis
- Hospital Value Proposition Canvas
Frequently Asked Questions
Plan working capital separately from CAPEX because hospital cash comes in after staffing, supplies, and claims work begin In this model, monthly fixed overhead is $475k and Year 1 leadership payroll is about $208k per month A three-month runway for those two items alone is about $205M, before clinical labor, medical supplies, payer delays, and reserves