 Owner income$95k
Owner income$95kHow Much Kinesiology Practice Owners Make At $313K/Month

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$95k  Net margin-60% to 27%
Net margin-60% to 27% Revenue for target pay$104k
Revenue for target pay$104k Business difficultyHard
Business difficultyHard


You’re estimating owner take-home, not a guaranteed wage This US kinesiology practice model starts with $31,335 in monthly collected revenue in the first year, then tracks revenue, costs, reserves, owner pay, and profit across a five-year planning period
Owner income$95kNet margin-60% to 27%Revenue for target pay$104kBusiness difficultyHardWant to test your owner income?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate only, not guaranteed salary, tax advice, or owner distribution advice.
Want to check owner income in the Kinesiology Practice forecast?
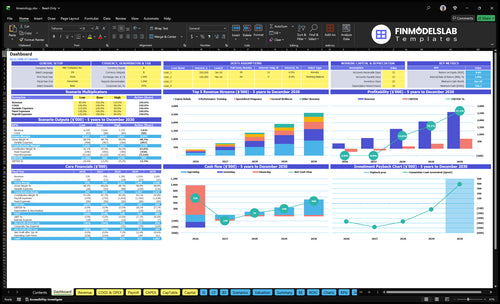
Open the full clinic forecast in the Kinesiology Practice Financial Model Template; it shows revenue, costs, reserves, and owner take-home in one view.
Owner-income model highlights
- Owner take-home outputs
- Revenue and staffing costs
- Scenario testing and cash flow
- 500% to 850% utilization
- $7,500 overhead monthly
What affects kinesiology practice profit margin?
Profit margin in a Kinesiology Practice comes down to completed visits, utilization (how full the calendar is), payroll, rent, marketing, payment fees, software, and no-shows. For startup cost context, see How Much Does It Cost To Open A Kinesiology Practice?; with 90% of first-year revenue tied to direct non-labor costs, only 10% is left before payroll and fixed overhead. At $7,500/month in fixed overhead, idle capacity hurts fast, and booked-but-unpaid sessions do not fund owner pay.
Revenue drivers
- Completed visits drive cash collected
- Utilization lifts revenue fast
- No-shows cut margin hard
- Booked visits need payment to count
Cost pressure
- Direct non-labor costs can hit 90%
- Only 10% stays before payroll
- Fixed overhead is $7,500/month
- Rent, fees, software all trim margin
Is a kinesiology practice profitable as a solo owner?
A Kinesiology Practice can be profitable for a solo owner, but the ceiling is set by appointment capacity, not demand. Doing the clinical work yourself protects margin, while a staffed clinic can grow from 5 service-provider slots in Year 1 to 19 by Year 5 across rehab, performance, wellness, corporate, and specialized programs. Still, owner income does not rise automatically, because utilization, scheduling, admin load, and cash reserves have to keep up.
Solo owner margin
- Keep the clinical work in-house.
- Protect margin by avoiding payroll early.
- Revenue still stops at booked hours.
- One owner means one capacity ceiling.
Scaling tradeoffs
- Growth can reach 19 slots by Year 5.
- More staff means more payroll risk.
- Utilization must stay high.
- Admin load and cash reserves matter.
How much does a kinesiology practice owner take home?
A Kinesiology Practice owner may take home $95,000/year if they personally fill the Clinic Director seat; that is compensation, not profit distribution. In the first-year model, revenue is $31,335/month against $7,500/month fixed overhead and $350,000/year known payroll, so staffed-clinic owner profit depends on utilization; see What Is The Current Growth Trend Of Kinesiology Practice? for growth context.
Owner Pay
- $95,000/year Clinic Director compensation
- Not the same as owner profit
- Solo payroll may look better
- Capacity caps solo take-home
Quick Math
- $376,020/year modeled revenue
- $90,000/year fixed overhead
- $29,167/month known payroll
- -$5,332/month before durable profit
What drives kinesiology practice owner income?
1
500%-850%Appointment Utilization
Filled treatment hours drive most of the cash because more booked visits spread rent and staff pay across more revenue.
2
$100-$250Average Fee
Higher collected fees raise revenue per session, and the gap between rehab, wellness, and corporate work moves take-home fast.
3
$350KClinician Labor
Payroll is the biggest cost block, so every extra clinician only helps if the schedule stays full.
4
$250Service Mix
Shifting more sessions into higher-priced programs lifts revenue without adding much extra space.
5
$7.5K/moOverhead Control
Rent, software, insurance, and admin costs are fixed, so lean overhead gets you to breakeven sooner.
6
50%Referral Flow
Strong referrals and repeat clients cut paid marketing needs, which matters when early marketing spend is heavy.
Kinesiology Practice Core Six Income Drivers
Billable Appointment Volume
Billable Session Volume
Completed sessions drive owner income, not booked slots. Year 1 planning uses 100 injury rehab treatments per rehab clinician at 600% utilization and 90 performance sessions at 550%. If visits don’t close, revenue slips even when the calendar looks full.
Idle rooms still carry rent, and cancellations cut collections while payroll and software stay due. That means a full-looking schedule can still miss profit. The quick math is simple: more completed treatments per clinician hour lift contribution, but adding space too early just adds fixed cost.
Track Closed Visits, Not Bookings
Measure what turns into cash: completed sessions, cancellation rate, room utilization, and collected revenue. Forecast from completed visits only, since booked appointments do not pay the bills if they no-show or cancel late.
- Completed sessions per clinician
- Booked-to-completed rate
- Room fill by day
- Collected fee per visit
- Open slots by service type
Keep fixed overhead tight until schedules hold. With $7,500 of monthly fixed overhead already due, every extra completed visit helps owner pay faster. Fill existing capacity first, then add space.
1
Average Collected Fee
Average Collected Fee
Average collected fee is the cash you actually keep per completed visit after discounts, denials, and package adjustments. Year 1 collected rates are $120 for injury rehab, $130 for performance training, $100 for general wellness, $250 for corporate ergonomics, and $150 for specialized programs. Higher posted prices only help if clients finish care and payment comes through.
Here’s the quick math: a $150 collected visit beats a $180 list price that does not collect. This driver flows straight into revenue, then gross margin, because rent, software, and payroll stay due even when collections slip. If denials rise or packages get adjusted down, owner pay gets squeezed fast.
Track collected dollars, not sticker price
Measure collected revenue ÷ completed visits by service line. Also track discount rate, denial rate, package adjustment rate, and completion rate, since fee quality depends on both pricing and follow-through. If visit completion falls, the average collected fee can drop even when the list price looks strong.
- $120 injury rehab collected fee
- $130 performance training collected fee
- $100 general wellness collected fee
- $250 corporate ergonomics rate
- $150 specialized program fee
Raise fees only when demand holds and plans get completed. If collections soften, cash flow tightens first, then owner draw, because fixed costs do not wait for late payments.
2
Service Mix And Programs
Service Mix And Programs
The mix of services changes income because each hour of therapist time can produce a different amount of revenue. In the year-1 model, corporate ergonomics is priced at $250 but has 0 therapists and 0% utilization, so it adds $0 until staffed and booked.
By contrast, specialized programs add $6,000/month from 1 therapist, 80 treatments, $150 per visit, and 500% utilization. That mix drives better revenue per provider hour, which lifts gross profit and gives the owner more room to pay themselves after payroll and rent.
Track Revenue Per Provider Hour
Measure collected revenue, not just booked visits. Track price, completed treatments, utilization, and room occupancy by program, then compare each service against therapist payroll. A higher sticker price does not help if the room sits empty.
- Compare revenue by service line.
- Watch therapist hours used.
- Drop weak-fill blocks fast.
- Protect payroll from empty rooms.
Use evaluations, rehab plans, performance programs, and wellness follow-ups to keep schedules full without making medical outcome claims. If one program fills and another stalls, rebalance the mix before adding staff or space, because idle capacity still carries fixed cost and slows owner draw.
3
Practitioner Staffing Model
Practitioner Payroll Load
Payroll is the gatekeeper for owner income. The disclosed Year 1 base payroll is $350,000: a $95,000 Clinic Director, 2 rehab kinesiologists at $65,000 each, 1 performance kinesiologist at $65,000, and 1 wellness kinesiologist at $60,000. That is about $29,167/month before any extra labor costs.
Gross margin after practitioner labor has to be measured before owner pay. If utilization is still ramping, payroll stays fixed while collected revenue lags, so cash gets tight fast. Hiring ahead of demand can turn growth into a wage burden instead of profit.
Track Labor Before You Add Headcount
Keep hiring tied to utilization, collected revenue per clinician, and payroll as a share of revenue. Treat owner compensation as separate from practitioner labor, so you can see the real margin left to pay yourself.
- Payroll: $350,000 base load
- Utilization: fill before hiring
- Owner pay: margin after labor
Do not add another clinician until current schedules can support the salary and still leave cash for overhead. If utilization matures slowly, stage hires and forecast monthly collections so the owner’s draw does not get crowded out.
4
Fixed Overhead Control
Fixed Overhead Floor
Fixed overhead is the monthly cost that stays due even when visits slow. Here it totals $7,500/month: rent $5,000, utilities $800, practice software $400, cleaning $400, liability insurance $300, office supplies $250, property insurance $200, and website support $150. That number is the break-even floor before owner pay, so it sets how much visit volume the practice must cover first.
What this hides is cash timing. If schedules dip, rent and insurance still go out, but collections fall. So the owner’s take-home income gets squeezed fast unless reserves are in place. Every extra $1,000 of fixed cost needs more completed visits just to keep the same profit level.
Hold the Monthly Cap
Track each fixed line item every month and ask one question: does it help collect more visits or protect cash? Use the fixed cost list below as the control set:
- Rent: $5,000
- Utilities: $800
- Practice software: $400
- Cleaning: $400
- Liability insurance: $300
- Office supplies: $250
- Property insurance: $200
- Website support: $150
Keep the cap at $7,500 unless added cost clearly supports more completed visits. Build reserves for slow months, because fixed overhead does not drop when the schedule opens up. That protects owner pay when collections come in lighter than plan.
5
Retention And Referral Flow
Retention And Referral Flow
When clients complete care plans and rebook, income becomes steadier instead of relying on one-off visits. That matters because rent, payroll, and payment processing do not drop when a session cancels, so every no-show hurts collected revenue more than it saves cost. Referral flow from physicians, trainers, employers, and past clients can also reduce paid marketing spend.
Track repeat visits, completed plans, cancellation rate, and source mix. The owner’s take-home pay improves when more booked clients show up, finish treatment, and return for follow-up care, because cash comes in with fewer gaps and the schedule depends less on new lead spending.
Track Rebooks And No-Shows
Measure retention by source, not just by total booked visits. If a referral source sends clients who finish plans and rebook, that channel is more valuable than a bigger source that drops off after one visit. Tie each source to completed care plans and repeat visit rate so you can see which referrals create real collections.
Control no-shows with a clear policy and fast follow-up. Because fixed costs stay due when visits cancel, even a modest rise in cancellations can squeeze margin and owner pay. Review cancellation rate weekly, compare it across sources, and shift attention toward the channels that bring in clients who stay engaged and keep returning.
6
Compare low, base, and high owner-income cases
Owner income scenarios
Owner income moves mostly with utilization, referral flow, and staffing because fixed rent and payroll stay high when volume is light. Profit only opens up after the clinic fills capacity.
| Scenario | Low CaseLow case | Base CaseBase case | High CaseHigh case |
|---|---|---|---|
| Launch model | Owner income stays under pressure because early utilization is weak and referrals are slow. | Owner income follows the modeled launch path with a normal ramp in visits and staffing. | Owner income rises faster once utilization and service mix both scale well. |
| Typical setup | Revenue runs below the first-year model level, slower referrals keep the calendar thin, and the same $7,500 monthly overhead plus payroll drag reduce take-home. | First-year revenue is about $31,335/month at a 91.0% margin before payroll and fixed overhead, and the $95,000 Clinic Director salary is already inside wages. | Year 5 revenue reaches about $215,930/month as utilization moves toward 75% to 85%, the service mix broadens, and staffing scales with demand. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | -$227k to -$129kLaunch loss | $167kProfit starts | $347k to $703kScaled profit |
| Best fit | Best for founders stress-testing a slow start and early cash pressure. | Best for a modeled launch with the owner on payroll and a standard ramp. | Best for planning a mature clinic with strong utilization and expansion upside. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Kinesiology Practice Porter's Five Forces Analysis
- Kinesiology Practice BCG Matrix
- Kinesiology Practice Business Model Canvas
- 7 Critical KPIs for Kinesiology Practice Growth and Profitability
- Kinesiology Practice Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Kinesiology Practice Profitability
- Running Costs for a Kinesiology Practice: 2026 Financial Breakdown
- Kinesiology Practice Startup Costs: $140K CAPEX Plus Runway
- Kinesiology Practice Financial Model Template in Excel
- How To Open A Kinesiology Practice In 8 To 16 Weeks
- How to Write a Kinesiology Practice Business Plan: 7 Steps
- Kinesiology Practice Marketing Mix
- Kinesiology Practice Marketing Plan
- Kinesiology Practice Business Proposal
- Kinesiology Practice PESTEL Analysis
- Kinesiology Practice Pitch Deck Example Editable PPTX
- Kinesiology Practice Business SWOT Analysis
- Kinesiology Practice Value Proposition Canvas
Frequently Asked Questions
The researched model includes $95,000 for a Clinic Director role, but owner take-home is not guaranteed First-year revenue is $31,335/month before $7,500/month fixed overhead and known payroll of $350,000/year Profit depends on completed sessions, service mix, staffing, and reserves