 Time to Open6-12 monthsLaunch runway
Time to Open6-12 monthsLaunch runwayHow to Launch Medical Decision Support Software in 6–12+ Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open6-12 monthsLaunch runway  Launch Sequence6 stagesCompliance first
Launch Sequence6 stagesCompliance first Key BottleneckApproval gateEHR signoff
Key BottleneckApproval gateEHR signoff First Revenue StepPaid pilotPilot fee live
First Revenue StepPaid pilotPilot fee live


To launch medical decision support software, start with one clear clinical use case, confirm the regulatory and privacy path, validate the rules or algorithms, build secure infrastructure, and test the workflow with pilot providers A realistic researched planning assumption is 6–12+ months, with the main delay usually coming from clinical validation, EHR access, security review, and provider contracting First revenue usually comes from a paid pilot, implementation fee, or provider subscription, with Year 1 assumptions showing $1,500 to $7,500 monthly subscriptions and $5,000 to $25,000 one-time setup fees by product tier
Time to Open6-12 monthsLaunch runwayLaunch Sequence6 stagesCompliance firstKey BottleneckApproval gateEHR signoffFirst Revenue StepPaid pilotPilot fee liveLaunch timeline
Short web summary of the launch plan; the XLSX export holds the detailed Gantt Chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8Month 9Month 10Month 11Month 12
Clinical scope
- Define intended use
- Pick pilot specialty
- Review clinical evidence
- Set escalation rules
Compliance review
- Regulatory classification review
- HIPAA control gap review
- Draft BAA template
- Vendor approval package
- Security audit plan
Product build
- Build core workflow
- Add analytics module
- Add alert engine
- Build diagnostics module
- QA test suite
Security and integration
- Map data fields
- Connect integration points
- Test access controls
- Validate data flow
Pilot validation
- Recruit pilot sites
- Train pilot clinicians
- Run pilot workflow
- Review pilot results
- Tune decision rules
Sales and ops
- Build sales deck
- Draft pricing sheets
- Set support scripts
- Prepare contract pack
- Plan go-live
Why stress-test the launch plan before hiring?
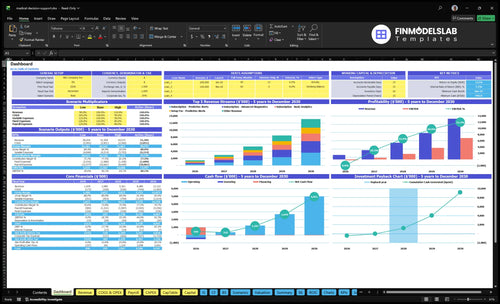
The Medical Decision Support Software Financial Model Template is a second check before hiring; it maps launch timing, staffing, runway, and breakeven. Open the model.
Model highlights
- $150k marketing spend
- $2,500 CAC target
- 25% visitor-to-lead
- 10% lead-to-paid
- $1.5k to $7.5k subscriptions
- $5k to $25k setup
- 19% variable costs
- Slow pilots, delay EHR approval
What regulatory requirements apply to clinical decision support software?
Medical Decision Support Software requirements turn on intended use: a read-only dashboard is different from an AI recommendation engine that directs diagnosis or treatment. Start with How Much To Start Medical Decision Support Software? after mapping whether the FDA (US Food and Drug Administration), HIPAA (Health Insurance Portability and Accountability Act of 1996), state privacy rules, and provider contracts apply; treat this as a compliance planning checkpoint, not legal advice. The launch bar is a written classification memo, privacy map, business associate agreement readiness, audit trails, clinical validation file, provider documentation, and counsel review before broad sales.
Rules to Map
- Document intended use before product build
- Classify patient risk: low to high
- Test clinician independence and override rights
- Check FDA CDS guidance from September 28, 2022
Launch Proof
- Map protected health information under HIPAA, 1996
- Prepare business associate agreements for providers
- Keep audit trails for every alert
- Complete counsel review before broad sales
How long does it take to launch clinical decision support software?
Medical Decision Support Software usually takes 6–12+ months to launch, not a few weeks. The early months cover clinical scope, regulatory review, data needs, and product architecture; later months get spent on algorithm validation, HIPAA-ready infrastructure, EHR API testing, pilots, training, and subscription conversion. If onboarding or security review takes 14+ days per provider, revenue recognition slows and the schedule stretches.
Launch timing
- 6–12+ months is practical.
- Early months set clinical scope.
- Build for regulatory review first.
- Plan around data and architecture.
What slows it down
- 14+ days per provider slows cash.
- Security reviews often drag launches.
- Hospital procurement adds delay.
- Trust and workflow approval matter most.
How do you get first customers for clinical decision support software?
First customers for Medical Decision Support Software usually come from one specialty pilot, not broad marketing. Start with one workflow, get a clinical champion, define outcome metrics, and demo the tool inside the provider’s real process, like the path in How Increase Medical Decision Support Software Profitability?. Revenue usually starts as a paid pilot, an implementation fee, or a subscription; Year 1 pricing can be $5,000, $12,000, and $25,000 one-time, or $1,500, $3,500, and $7,500 monthly.
Pilot first
- Pick one specialty workflow
- Secure one clinical champion
- Set outcome metrics early
- Demo inside the real workflow
Sales math
- Use $150,000 marketing budget
- Model $2,500 CAC
- Track 25% visitor-to-lead
- Track 10% lead-to-paid
Confirm what must be complete before selling to providers
Launch readiness checklist
Use this go-live approval checklist before opening. It confirms the software, compliance, staffing, and first-revenue path are ready.
Regulatory
- Intended use statement approvedCritical
The product must state its intended use before any pilot or customer contract.
- FDA review path identifiedHigh
If claims trigger review, you need a clear checkpoint before launch.
- Privacy notice publishedHigh
Users need clear privacy terms before any clinical data is collected.
- BAA process documentedCritical
A BAA is needed before handling protected health information for customers.
Security
- HIPAA hosting selectedCritical
Secure hosting must be in place before live clinical data enters the system.
- Audit trails enabledCritical
Audit logs help trace access and support security reviews after launch.
- Retention policy approvedHigh
You need a clear rule for what data stays, what deletes, and when.
- Test environment isolatedHigh
Test data should stay separate so staff do not mix it with live records.
Integrations
- EHR API plan approvedCritical
The EHR API path must work before providers can trust the workflow.
- Integration vendors signedHigh
Vendor terms must be set before any live integration work starts.
- Security audit vendor bookedHigh
HIPAA and security checks need an outside review before launch.
- Dev tools activeMedium
The team needs active dev tools to build, test, and fix issues fast.
Clinical pilot
- Validation evidence reviewedCritical
Clinical logic needs proof before providers rely on the output.
- Clinical feedback loop setHigh
Early user feedback helps catch bad logic before scale starts.
- Escalation path documentedHigh
Staff need one path for urgent clinical issues and service failures.
- Uptime monitoring liveCritical
Providers need stable access, so downtime must be tracked from day one.
Revenue
- Year one mix confirmedHigh
Year 1 should match the 60/30/10 mix for Basic, Predictive, and Advanced.
- Demo flow testedCritical
The demo path must move a visitor into a qualified lead without friction.
- Lead handoff scriptedHigh
Sales and clinical teams need one handoff path so demos do not stall.
- CAC target trackedHigh
Year 1 CAC is modeled at $2,500, so spend needs a hard cap.
Launch control
- Month one hires fundedCritical
CEO, data science, and sales roles start in Month 1, so payroll must be funded.
- Launch cash runway checkedCritical
Minimum cash hits $446k in Month 13, so launch needs room for early losses.
- Onboarding workflow readyHigh
If onboarding drags, clinicians may churn before the first contract renews.
- Go-live signoff completeCritical
No launch if use, validation, BAA, security, or pilot support is incomplete.
Which launch drivers matter most before go-live?
1Regulatory Privacy
6-12 moA clear intended-use decision speeds approvals, claims, and provider trust.
2Clinical Evidence
Pilot proofValidated cases and guideline alignment improve champion buy-in and pilot conversion.
3EHR Integration
EHR accessMapped data fields and workflow tests cut go-live delays and abandoned pilots.
4Security Approval
Vendor gateSecurity review and vendor approval can still block go-live until procurement clears.
5Provider Pilots
$5K-$25KNamed clinical champions and a paid setup fee turn pilots into real revenue.
6Support Capacity
2 core FTEDay-one support capacity keeps onboarding clean and stops pilot overload.
Regulatory, Privacy, and Intended Use
Lock Intended Use Early
Intended use is the launch gate for medical decision support software. If you sell it as a risk-scoring engine or recommendation system before the scope is written, you can trigger US Food and Drug Administration (FDA) review questions, widen Health Insurance Portability and Accountability Act (HIPAA) duties, and slow provider risk approval. That means delayed contracts, late redlines, and no clean day-one go-live.
Keep the first version narrow. A general support or Basic Analytics offer can launch with lower procurement friction, then expand to Predictive Alerts after counsel signs off on claims, documentation, and audit trail design. That path gets you faster provider trust and fewer procurement stalls.
Document the Scope Package
Before launch, write the product classification, privacy workflow, business associate agreement (BAA) process, and audit log plan. Also have counsel review provider-facing materials so sales teams stay inside the approved claim set. That’s the cleanest way to avoid selling a feature the contract and controls cannot support.
If you need outside help, the disclosed setup load includes $4,500/month for HIPAA compliance and security audits and $6,000/month for legal and regulatory counsel. Build that into launch timing, because it can hit before the first subscription invoice.
- Classify the product in writing.
- Map workflow, data, controls, contracts.
- Review provider materials with counsel.
- Test audit logs before demos.
1
Clinical Evidence and Validation
Clinical Proof
You can’t open this software on time if the evidence pack is thin. Providers need proof before they trust decision support inside care workflows, so launch depends on validated rules or algorithms, guideline alignment, clinician-reviewed test cases, bias checks, and documented performance limits.
The bottleneck is weak evidence behind a high-risk recommendation. If false positives and false negatives are not reviewed before go-live, clinical champions lose confidence, pilots stall, and the first rollout turns into rework instead of day-one use.
Validate Before Go-Live
Lock one stable product version, use clean data, and get specialty input before the pilot date. Build the validation file first, then define pilot success metrics so the team knows what “good enough” means before opening.
- Review clinician cases before rollout.
- Document alert limits and exclusions.
- Track false positives and false negatives.
- Assign one clinical reviewer per specialty.
What matters on day one is not a perfect model; it’s a known model. If the team cannot explain when the recommendation should fire, and when it should not, the software is not ready for live care use.
2
EHR and Workflow Integration
EHR Workflow Fit
EHR means electronic health record. FHIR means Fast Healthcare Interoperability Resources, and HL7 means Health Level Seven International. This launch driver matters because clinicians will not keep using a tool that slows charting, adds clicks, or fires alerts at the wrong time. For CliniSight AI, launch only works if the insight fits the clinician’s day and shows up inside the chart.
Readiness depends on mapped data fields, API access, test environment results, alert timing, and minimal workflow disruption. The biggest bottleneck is delayed EHR access from the provider, which can push out testing and stall go-live. A narrow specialty workflow is the safer first launch than broad integration across the whole organization.
Go-Live Sequence
Start with workflow mapping, then data mapping, then interface testing, then go-live dry runs. That order shows where the product breaks before clinicians feel it. If provider IT access, vendor permissions, or sandbox data are missing, treat the launch date as at risk until those gates are closed.
- Confirm provider IT access early
- Get vendor permissions in writing
- Test with sandbox data only
- Check alert timing in workflow
- Run clinician dry runs before launch
3
Security, Procurement, and Vendor Approval
Vendor Approval and Security Review
Healthcare buyers often block go-live until vendor risk review is done, so security can delay opening even when the product is ready. For a clinical decision support platform, that means the first customer may not start until the security questionnaire, penetration test plan, access controls, data retention policy, BAA (business associate agreement) readiness, and any required SOC 2 readiness are in hand.
The launch risk is not just paperwork. You also need documented HIPAA safeguards, audit logs, user roles, incident response, and hosting controls before procurement will clear the vendor. Budget matters too: the source figures show $4,500/month for HIPAA compliance and security audits plus $6,000/month for legal and regulatory counsel, and slow hospital approval can push first revenue back.
Pre-Clear the Buyer Review
Start vendor approval work before sales close. Have the cloud setup, legal review, and security files ready at the same time, because hospital procurement usually runs on its own timeline. One missed item can stall the buyer review cycle and keep the team from serving day one users.
Use a launch packet with the security questionnaire, BAA template, incident response plan, and hosting details. Assign one owner to track every open question, then test the review path with a target buyer early. That is the fastest way to shorten approval time and avoid a launch gap.
- Document HIPAA safeguards first.
- Prepare audit logs and user roles.
- Keep insurance proof ready.
- Align legal review with procurement timing.
4
Provider Pilots and Clinical Champions
Provider Pilots
Healthcare buyers usually trust workflow proof more than sales decks, so this driver decides whether the business can open with a real buying path or just a demo. A strong pilot needs a specialty use case, a named clinical champion, a clear protocol, success metrics, and a conversion path to subscription. Without that, launch slips into unpaid testing with no revenue signal.
For a medical decision support product, the pilot is the first live test of clinician availability, data access, contracting, and support capacity. If any of those are weak, go-live stalls and day-one operations become reactive instead of planned. Unpaid pilots with no buying path are the main risk because they consume time, delay first revenue, and weaken the proof needed for the next provider.
Pilot Setup
Before opening, lock the pilot scope in writing: use case, data fields, training plan, review checkpoints, and who signs off on success. Build outcome-based demos so the buyer sees the workflow, not just the model. If the team cannot assign a clinical champion and support owner, the pilot is not ready to start.
Price the pilot so it creates real launch cash and a clear next step. The disclosed setup-fee tiers are $5,000, $12,000, or $25,000 before subscription conversion. That one-time fee helps fund onboarding, integration, and support, and it turns the pilot into a first-revenue event instead of a free trial that drifts.
- Confirm clinician time for training and review.
- Verify data access before scheduling go-live.
- Document success metrics and pilot end date.
- Set the conversion path up front.
5
Implementation, Support, and Day-One Operations
Day-One Support Readiness
Launch fails fast when the first live users hit gaps in onboarding, training, uptime, or support. For a clinical decision support tool, day one is not just software being live; it is a working onboarding workflow, issue escalation path, and clinical feedback loop inside the EHR environment so staff can use it without guesswork.
The main risk is selling more pilots than the team can support. With Month 1 CEO/product strategy at $180,000 annual salary and a lead data scientist at $165,000, base payroll alone is about $28,750 per month. If support, monitoring, and release control are thin, go-live slips, incident response slows, and subscription conversion gets messier.
Go-Live Support Checklist
Before opening, lock the support model around the live workflow: who owns tickets, who approves releases, and who reviews clinical feedback. Here’s the quick math: $15,000 monthly for the CEO/product lead plus $13,750 for the data scientist means every delay burns real cash, so the launch plan has to match the staff you actually have.
- Assign one named support owner.
- Write go-live scripts for users.
- Track incidents from day one.
- Test monitoring dashboards before launch.
- Document release approval steps.
- Confirm cloud and EHR access.
What this setup hides is downtime risk from vendor stack issues, cloud hosting gaps, or delayed EHR integration. If those pieces are not tested in a sandbox first, first-day operations can stall even when the product logic is sound, and that usually shows up as slower onboarding and weaker early retention.
6
Related Products
- Medical Decision Support Software Porter's Five Forces Analysis
- Medical Decision Support Software BCG Matrix
- Medical Decision Support Software Business Model Canvas
- What Five KPIs Should Medical Decision Support Software Business Track?
- Medical Decision Support Software Business Plan Template in Pre-Written Word
- How Increase Medical Decision Support Software Profitability?
- What Are Medical Decision Support Software Operating Costs?
- Medical Decision Support Software Startup Costs: $646K Opening Plan
- Medical Decision Support Financial Model Template in Excel
- How Much Medical Decision Support Software Owners Make At $249M
- How To Write A Business Plan For Medical Decision Support Software?
- Medical Decision Support Software Marketing Mix
- Medical Decision Support Software Marketing Plan
- Medical Decision Support Software Business Proposal
- Medical Decision Support Software PESTEL Analysis
- Medical Decision Support Software Pitch Deck Example Editable PPTX
- Medical Decision Support Software Business SWOT Analysis
- Medical Decision Support Software Value Proposition Canvas
Frequently Asked Questions
Start with one clinical use case and one buyer workflow Then document intended use, validate the rules or algorithms, build HIPAA-ready infrastructure, and recruit pilot providers Use the 6–12+ month launch range as your planning base, with first revenue tied to paid pilots, setup fees, or monthly subscriptions