 Owner income$180k
Owner income$180kHow Much Medical Decision Support Software Owners Make At $249M

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$180k  Net margin-21% to 52%
Net margin-21% to 52% Revenue for target pay$344k
Revenue for target pay$344k Business difficultyHard
Business difficultyHard


A medical decision support software owner can model first-year pre-tax pay around the planned $180k CEO salary, with distributions only if cash remains after reserves and reinvestment The researched base math uses 60 new customers, $324k subscription ARR per customer, $91k average implementation fees, and $249M annualized revenue Gross margin is 88% after cloud hosting and Electronic Health Record integration costs What this estimate hides is timing: provider sales, onboarding, validation, and renewals can delay cash
Owner income$180kNet margin-21% to 52%Revenue for target pay$344kBusiness difficultyHardWant to test your owner take-home?
Owner income calculator
Estimate owner take-home and target-pay gap from monthly revenue, gross margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only; it is not guaranteed salary, tax advice, or owner distribution advice.
Want to check owner income in the Medical Decision Support Software model?
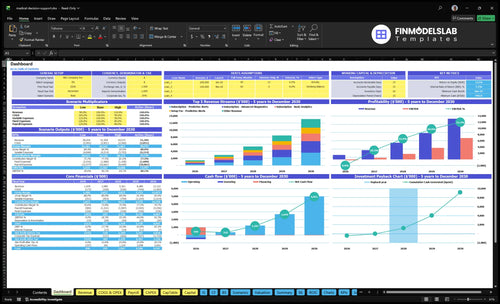
The dashboard ties assumptions, ARR, churn, staffing, compliance, and owner income together; open the Medical Decision Support Software Financial Model Template. It’s a planning bridge, not the main promise.
Owner-income model highlights
- Planned CEO salary
- ARR, revenue, margin
- Scenarios and reserve cover
Can a medical decision support software business scale profitably?
Medical Decision Support Software can scale profitably, but owner income can lag while provider sales cycles, clinical validation, integrations, and support absorb cash. Here’s the quick math: marketing rises from $150k to $800k, CAC falls from $2,500 to $2,100, and lead-to-paid conversion improves from 10% to 15%, while advanced diagnostics grows from 10% to 30% of the mix. Plan owner pay after delivery capacity.
Profit drivers
- Raise marketing from $150k to $800k
- Cut CAC from $2,500 to $2,100
- Lift conversion from 10% to 15%
- Shift mix to 30% advanced diagnostics
Scale pressure
- Sales roles rise from 1 to 5 FTEs
- Implementation roles rise from 1 to 4 FTEs
- Engineering roles rise from 2 to 6 FTEs
- Owner pay should wait for delivery capacity
What medical decision support software profit margin affects owner income?
Owner income in Medical Decision Support Software is driven by contribution margin (cash left after direct selling costs), not just top-line sales. Here’s the quick math: direct costs fall from 12% of revenue in year 1 to 8% in a mature year, so gross margin moves from 88% to 92%; year-1 sales commissions and payment processing take another 7%, so every point lost to hosting, integration, support, or billing hits owner pay fast. For the full margin map, see How Increase Medical Decision Support Software Profitability?
Margin drivers
- 12% direct costs in year 1.
- 8% direct costs in mature year.
- Gross margin rises from 88% to 92%.
- Lower direct cost lifts owner take-home.
Cash still leaves
- 7% sales commissions and payment processing.
- Health Insurance Portability and Accountability Act (HIPAA) audits cost money.
- Legal counsel and insurance cut distributable cash.
- Engineering payroll and clinical staff still drain cash.
How much can a clinical decision support software founder pay themselves?
A Medical Decision Support Software founder can pay themselves the planned $180,000 CEO and product strategy salary from launch, based on the researched model in How Much To Start Medical Decision Support Software?. Distributions are separate and should wait until direct costs, payroll, marketing, compliance, reserves, taxes, and reinvestment are covered.
Founder Pay
- Set salary at $180,000/year
- Treat salary as payroll expense
- Pay taxes through payroll
- Avoid early cash draws
Distribution Check
- Model revenue: $249M annualized
- Adjusted EBITDA before owner pay: $861,000
- Protect runway if onboarding slows
- Delay distributions if renewals weaken
Want the six owner-income drivers?
1
$324KACV
Higher contract value raises revenue per sale fast; even a small mix shift lifts owner income, but price cuts hit cash quickly.
2
88%-92%Gross Margin
With margin in this range, each cost point saved drops straight to EBITDA, especially on cloud, integrations, and billing.
3
HighRenewals
Renewals protect recurring revenue and lower replacement selling, but adoption drops after launch can erode take-home fast.
4
60Customer Count
More first-year customers spreads fixed overhead and sales cost, but weak pipeline volume shows up fast in cash burn.
5
$2.5K-$2.1KSales Efficiency
Lower CAC frees cash and shortens payback, but longer sales cycles can wipe out the gain before revenue lands.
6
$336KCompliance Load
HIPAA, legal, and security staffing are hard to trim, so a $336K fixed base can delay payback if headcount outruns revenue.
Medical Decision Support Software Core Six Income Drivers
Annual Contract Value And Pricing Model
Annual Contract Value
Higher annual contract value means each close adds more ARR, so owner income can grow faster without chasing lots of small accounts. Here, first-year weighted subscription ACV is $324k, and mature-year weighted subscription ACV reaches $5,868k, with implementation fees rising from $91k to $177k.
That pricing only holds if the software proves clinical value, fits daily workflow, and meets compliance and support needs. Big tiers can lift profit, but they can also add heavier validation, integration, and customer success work, which can eat into cash and delay owner pay if staffing does not scale with revenue. One strong deal can beat many weak ones.
Price to Scope, Not Just Seats
Measure providers, tier mix, implementation fee, and support hours for each account. The pricing model should reflect clinical scope, organization size, and the amount of workflow change the customer expects. If a deal needs more validation or integration, price that work in up front instead of funding it from subscription margin.
Track these inputs in the forecast: subscription ACV, setup fees, renewal risk, and post-sale labor. If higher-tier accounts take more clinical review or customer success time, gross margin can fall even when revenue rises. The goal is simple: raise contract value faster than delivery cost so more of each dollar turns into cash for payroll and owner draw.
- Track ACV by tier.
- Price implementation by scope.
- Log support hours per account.
- Watch margin by customer size.
1
Customer Count And Market Penetration
Active Provider Customers
Customer count drives recurring revenue only after a provider contract closes and onboarding starts. The source math shows $150k in marketing at $2,500 CAC can produce about 60 first-year customers, while $800k at $2,100 CAC can reach about 381 mature-year customers. More live accounts mean more subscription cash for payroll, compliance, and owner pay.
Leads are not revenue. A 10% to 15% conversion lift helps, but provider procurement and implementation timing can push cash later than the sales forecast. So the real income driver is not pipeline size alone; it’s how fast signed deals become active, billing customers.
Track Signed, Live, and Paying
Measure leads, closes, onboarded customers, CAC, and days to go-live. That shows where revenue is stuck. If close rates rise but onboarding drags, cash still lags and owner draw gets tighter.
- Separate signed from live accounts.
- Track lead-to-paid conversion monthly.
- Forecast cash by go-live date.
- Watch CAC against payback time.
One clean test: compare booked deals to active customers every month, not just the sales pipeline.
2
Retention, Renewals, And Churn
Retention, Renewals, And Churn
Renewals are the cleanest way to make owner pay predictable. This software lives or dies on renewal rate and churn because subscription ARR is recurring, but only if hospitals and clinics keep using it after the first contract term.
No renewal-rate value is supplied, so keep it editable in the model. A lower renewal rate cuts subscription revenue before it cuts fixed payroll or compliance cost, so churn can squeeze profit and cash flow fast even when new sales still look healthy.
Track Renewal Risk Before It Hits ARR
Measure renewed ARR ÷ ARR up for renewal. Also track churned ARR, support tickets, uptime, and EHR integration failures. Retention here depends on clinical workflow fit, measurable value, support quality, uptime, and integration reliability, so those are the real levers behind owner income.
Churn is expensive because replacement sales cost more. If renewals weaken, marketing and sales spend rises just to refill lost ARR, and that delays owner draws. Build a renewal forecast by contract month, flag accounts with poor adoption, and fix issues before the next renewal window.
3
Gross Margin After Delivery Costs
Gross Margin After Delivery Costs
Gross margin is the cash left after direct delivery costs, and here that means cloud infrastructure, HIPAA hosting, and EHR API and integration maintenance. In this model, those costs fall from 12% to 8% of revenue, so gross margin rises from 88% to 92%. That extra 4 points is the pool that pays payroll, compliance, sales, and the owner.
Here’s the quick math: every 1 margin point on $249M of revenue is about $249k of annual cash. The catch is support burden and clinical content maintenance can still दब the margin even when hosting looks better, so the owner’s take-home depends on keeping direct service work from creeping above plan.
Track Direct Cost Run Rate
Measure gross margin monthly as revenue minus direct delivery costs, then split those costs into hosting, API maintenance, support, and clinical content upkeep. That tells you whether margin is improving because the product is efficient, or just because one cost bucket slipped. If support tickets rise, margin can fall fast even with stable cloud spend.
Use a simple target: hold direct costs near 8% of revenue, and flag any drift above that before it hits payroll or owner draw. If onboarding or integration work starts to consume more hours, treat it as a margin issue, not just an ops issue, because it cuts the cash available for compliance, sales, and profit.
4
Sales, Implementation, And Onboarding Efficiency
Sales Efficiency
CAC is the cost to win a paying customer. Here, it improves from $2,500 to $2,100, and lead-to-paid conversion rises from 10% to 15%. That means the same sales budget buys more ARR, so more of each new dollar can reach owner pay instead of getting spent on selling.
Sales commissions stay at 5% of revenue, so the margin gain comes mostly from better close rates and lower acquisition cost. The catch: implementation fees are separate from subscription ARR, and weighted fees rise from $91k to $177k, so onboarding work has to stay fast or cash comes in late.
Track the full handoff
Measure marketing spend, CAC, close rate, commission dollars, and days to go-live on each deal. Lead-to-paid conversion is just the share of leads that become paying customers, and it only helps owner income if implementation can keep up.
- Watch CAC by segment
- Track lead-to-paid weekly
- Separate setup cash from ARR
- Cap custom onboarding scope
Here’s the quick math: a lower CAC plus a 15% close rate means more revenue per sales dollar, but only if delivery can absorb the work. Custom onboarding can eat clinical implementation capacity, which can delay renewals or cash collection and squeeze owner draw.
5
Compliance, Clinical Validation, And Product Staffing
Compliance And Product Staffing Load
For a clinical decision support product, compliance and validation are part of the cost of selling, not optional spend. The disclosed fixed load is $45k/month for HIPAA compliance and security audits, $6k/month for legal and regulatory counsel, $3k/month for professional liability insurance, and $25k/month for software tools: $79k/month total, or $948k/year before product payroll.
Product payroll adds more pressure. It starts at $465k in year 1 and scales to the provided mature-year figure of $1395M. So owner take-home only rises after clinical review, security controls, regulatory work, and product updates are funded. If audit scope expands or releases slow down, cash goes to reinvestment first and profit to the owner later.
Track compliance burn tightly
Measure this as a monthly reinvestment rate, not just overhead. Here’s the quick math: track audit spend, legal hours, insurance, tools, and product FTEs separately, then tie each cost to live customers, active providers, and release cycles. That shows whether compliance is scaling with revenue or just shrinking the owner draw.
- Tag required work by category.
- Forecast payroll by release.
- Review audit cost monthly.
- Separate client work from core product work.
If onboarding takes longer or validation needs more review, staff and cash needs rise before revenue catches up. Keep those costs in the model as required reinvestment so you can see the real margin left for debt service, growth spend, and owner pay.
6
Compare lean, base, and growth owner-income scenarios
Owner income scenarios
Owner pay changes fast here because revenue grows from $1.439M in Year 1 to $13.122M in Year 5 while margin improves and payroll scales hard. These cases show pre-tax pay capacity, not guaranteed distributions.
| Scenario | Low CaseConservative | Base CaseBalanced | High CaseUpside |
|---|---|---|---|
| Launch model | The low case keeps owner pay near the planned $180k salary because Year 1 EBITDA is negative. | The base case adds some owner draw as Year 3 EBITDA turns strongly positive. | The high case supports a larger owner draw once Year 5 scale and margin mature. |
| Typical setup | Year 1 runs at $1.439M revenue, 88% gross margin, $150k marketing, $850k payroll, and $336k fixed overhead, so cash is tight. | Year 3 reaches $5.361M revenue, 90% gross margin, $400k marketing, and $1.63M payroll, which supports salary plus a modest draw if collections hold. | Year 5 reaches $13.122M revenue, 92% gross margin, $800k marketing, and $2.505M payroll, so owner pay can rise if support and renewals stay efficient. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $180k salary onlySalary only | $180k plus modest drawModest draw | $180k plus large drawLarge draw |
| Best fit | Use this if Year 1 cash stays tight or collections lag. | Use this for a steady case with some owner draw room after Year 3. | Use this to test upside if renewal, timing, and support stay strong. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Medical Decision Support Software Porter's Five Forces Analysis
- Medical Decision Support Software BCG Matrix
- Medical Decision Support Software Business Model Canvas
- What Five KPIs Should Medical Decision Support Software Business Track?
- Medical Decision Support Software Business Plan Template in Pre-Written Word
- How Increase Medical Decision Support Software Profitability?
- What Are Medical Decision Support Software Operating Costs?
- Medical Decision Support Software Startup Costs: $646K Opening Plan
- Medical Decision Support Financial Model Template in Excel
- How to Launch Medical Decision Support Software in 6–12+ Months
- How To Write A Business Plan For Medical Decision Support Software?
- Medical Decision Support Software Marketing Mix
- Medical Decision Support Software Marketing Plan
- Medical Decision Support Software Business Proposal
- Medical Decision Support Software PESTEL Analysis
- Medical Decision Support Software Pitch Deck Example Editable PPTX
- Medical Decision Support Software Business SWOT Analysis
- Medical Decision Support Software Value Proposition Canvas
Frequently Asked Questions
The researched model includes $180k planned CEO salary in the first year Annualized revenue is $249M from 60 customers, with 88% gross margin and about $861k adjusted EBITDA before owner pay Extra distributions are possible only after reserves, taxes, debt service, product work, and compliance needs