 Time to Open3-6 monthsSetup window
Time to Open3-6 monthsSetup windowHow to Open an Occupational Therapy Practice in 3 to 6 Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open3-6 monthsSetup window  Launch Sequence6 stagesCompliance first
Launch Sequence6 stagesCompliance first Key BottleneckCredentialing delayApproval path
Key BottleneckCredentialing delayApproval path First Revenue StepScheduled evalsBooking live
First Revenue StepScheduled evalsBooking live


You’re opening a care business where compliance, payer setup, referrals, and capacity must line up before the first patient This roadmap shows how to start an occupational therapy practice with a 3 to 6 month launch window, a five-year planning view, and a practical next step: validate licensing, credentialing, systems, staffing, and first-revenue assumptions before signing long commitments
Time to Open3-6 monthsSetup windowLaunch Sequence6 stagesCompliance firstKey BottleneckCredentialing delayApproval pathFirst Revenue StepScheduled evalsBooking liveOccupational therapy launch timeline
This is a short web summary of the launch plan, and the XLSX export carries the detailed Gantt Chart.
Launch scheduleWeek 1Week 2Week 3Week 4Week 5Week 6Week 7Week 8Week 9
Legal / compliance
- Verify state license
- Form entity
- Build HIPAA policies
- Secure malpractice
Location / build-out
- Sign lease
- Plan room layout
- Order equipment
- Complete build-out
Payer enrollment
- Create CAQH profile
- Submit payer packets
- Track approvals
- Test claims
Staffing / training
- Post therapist roles
- Hire core team
- Train documentation
- Run mock visits
Systems / billing
- Set up EHR
- Configure billing codes
- Build templates
- Test scheduling
Marketing / referrals
- Map referral sources
- Launch outreach emails
- Share opening packet
- Confirm first appointments
Why test an Occupational Therapy launch model before opening?
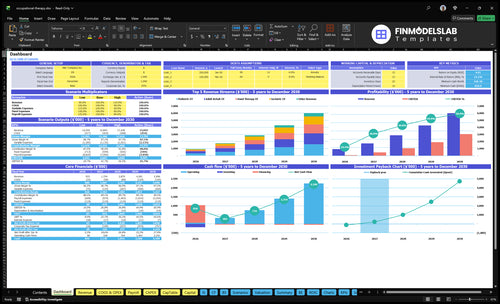
Use the Occupational Therapy Financial Model Template to check revenue ramp, payer mix, reimbursement, staffing, cash runway, and break-even. Year 1 at 60% capacity means 462 monthly treatments and about $77,760 in monthly treatment revenue, while fixed operating costs start at $9,900 before wages and variable supply costs. Open the model.
Key model tabs and charts
- Revenue ramp and visits
- Payer mix and rates
- Staffing load by role
- Runway and break-even path
How long does payer credentialing take for an occupational therapy practice?
Payer credentialing often sets the opening date for Occupational Therapy, so don’t promise insured visits until approvals are live. A realistic launch range is 3 to 6 months if credentialing and site readiness stay on track.
Credentialing sequence
- Start with NPI first
- Build CAQH ProView profile
- Upload malpractice coverage
- Submit payer applications
Launch timing rules
- Expect Medicare, Medicaid, and commercial gaps
- Run lease and EHR setup in parallel
- Use self-pay if approvals lag
- Delay insurance marketing until billing tests pass
How to get clients for an occupational therapy practice?
If you're trying to fill an Occupational Therapy caseload, the first clients usually come from referrals, not broad branding, and revenue starts when evaluations are scheduled from approved payers or the right self-pay clients. Pair local search pages with fast intake and referral relationships; service pricing can be set around $180 pediatric OT, $170 adult rehab, $160 geriatric OT, $200 hand therapy, and $100 group programs. Track referral source, booked evaluations, kept visits, and authorization delays so you can see what actually drives cash.
Referral sources
- Physicians and pediatricians
- Schools and discharge planners
- Attorneys and employer programs
- Senior-care providers and hospitals
Early revenue drivers
- Fast evaluation scheduling
- Clear service lines online
- Phone intake that answers fast
- Watch authorization delays closely
What licenses do you need to open an occupational therapy practice?
For Occupational Therapy, the launch gate is simple: be licensed, insured, documented, and billable before seeing a client; start with an active state occupational therapy license, then track demand with What Is The Current Growth Rate Of Client Engagement For Your Occupational Therapy Business?. Budget $500/month for professional liability insurance in the model, and get a 10-digit National Provider Identifier if you’ll bill payers.
Core licenses
- Confirm active state occupational therapy license
- Register business entity and tax accounts
- Obtain National Provider Identifier
- Complete CAQH ProView credentialing profile
Compliance checks
- Buy $500/month liability insurance
- Build HIPAA privacy and security policies
- Check signage, accessibility, and occupancy rules
- Enroll with Medicare, Medicaid, or insurers
Confirm the OT clinic is ready before seeing patients
Launch readiness checklist
Use this go-live approval checklist before opening to confirm the practice is compliant, schedulable, billable, staffed, and referral-active.
Licensing
- State OT license activeCritical
No license means no legal patient care or billing.
- Business registration filedHigh
The practice needs a legal entity before contracts and payer enrollment.
- NPI and CAQH completeCritical
Payers use these IDs to load claims and credential the practice.
- Payer enrollment approvedCritical
Without payer approval, visits may be schedulable but not billable.
- Malpractice insurance boundCritical
Coverage should be active before the first patient visit.
Space
- Lease and build-out completeCritical
The space must be usable before patients and staff arrive.
- Accessibility checkedHigh
Patients need safe access, restrooms, and clear movement.
- Cleaning plan approvedHigh
A clean room plan lowers infection and inspection risk.
Tools
- Therapy equipment installedCritical
Core tools must be ready for evals and treatment.
- EHR subscription activeCritical
Notes, orders, and schedules need one live system.
- IT security testedHigh
Protected systems help keep patient data and billing safe.
Records
- HIPAA policies signed offCritical
Privacy rules need to be set before records start.
- Consent forms readyHigh
Signed consent is basic protection before treatment starts.
- Documentation standards setCritical
Clear note rules keep care defensible and billable.
Staff
- Core therapist coverage setCritical
The launch needs enough clinicians for booked visits.
- Assistant support staffedHigh
Support staff keep visits moving and reduce therapist overload.
- Visit capacity matchedCritical
Do not hire ahead of demand; cash can get tight fast.
Launch
- Billing workflow testedCritical
Claims need a working path from note to payment.
- Authorization workflow readyCritical
Some payers block payment until prior approval is set.
- Referral outreach activeHigh
The first revenue step needs a live source of patients.
- Cash runway confirmedCritical
Model cash hit a $836k minimum in Month 2.
- Go-live signoff completeCritical
Final signoff should confirm compliant, staffed, and billable launch.
Which launch drivers decide if the OT practice opens cleanly?
1Licensing and compliance
3-6 moLicense, HIPAA, consent, and facility clearance must be clean before you can treat or bill.
2Payer credentialing
BillableActive payer approval makes insured referrals billable instead of delayed appointments.
3Clinic or mobile readiness
$75K buildBuild-out, equipment, and furniture must be ready for safe, schedulable care.
4EHR and billing workflow
Test claimA tested intake-to-claim workflow cuts denials and protects cash against $9.9K fixed costs before wages.
5Referral pipeline and demand
$77.8K/moBooked evaluation slots and referral partners drive the ramp to 60% of first-year capacity.
6Staffing and capacity
462/moCoverage for evaluations, follow-ups, and billing keeps 462 monthly treatments on track.
Licensing and compliance
License gate
Occupational therapy cannot legally open until the practice has state license readiness, entity setup, an NPI (National Provider Identifier), malpractice insurance, HIPAA policies, consent forms, and, if clinic-based, local facility clearance. A general business license is not enough. If any piece is missing, you can delay evaluations, treatment, billing, or patient data storage before the first visit.
Readiness shows up as a clean license status, payer-ready provider profiles, signed privacy and documentation workflows, and site approval where needed. Day one only works when the legal and clinical setup is finished, because weak compliance can trigger shutdown risk, billing blocks, and privacy exposure even if the space is ready.
Pre-open compliance check
Start with the legal path, not the lease or marketing. Verify the state license, entity, NPI, malpractice insurance, HIPAA packet, consent forms, and facility clearance before you schedule clients or buy equipment. If you are clinic-based, local clearance has to land before the first booked evaluation.
- Confirm license status and entity setup.
- Finish provider profiles before referrals.
- Test privacy, consent, and note workflows.
- Lock facility approval before opening day.
Use a simple test: can one patient move from intake to signed consent, documented care plan, and secure record storage without a gap? If not, the launch date is too early. Assign one owner to track approvals so the practice does not open with compliance holes.
1
Payer credentialing and reimbursement setup
Payer credentialing
For occupational therapy, payer credentialing decides when insured patients can turn into cash. Until NPI, CAQH ProView, payer apps, and any Medicare or Medicaid enrollment are approved, you can’t reliably bill evaluations or treatment, even if the clinic is open and referrals are coming in.
The risk is simple: if you market to insured patients before contracts and fee schedules are live, you can fill the schedule with unpaid visits or delayed starts. Active approval plus tested claims is the real day one signal. That’s what lets you convert referrals into billable evaluations instead of pushing people into waitlists.
Get billing live before outreach
Build the payer list first, then verify every input: provider identifiers, CAQH ProView profile, payer applications, contracted fee schedules, authorization rules, and claim testing. If one payer is missing, your front desk still has to sort out who can be seen, billed, or held.
Use a simple readiness check: active approvals, loaded contract terms, and a test claim that moves from charge entry to submission cleanly. The goal is not just opening the doors. It’s opening with a workflow that can turn a referral into a paid visit without scrambling after the patient arrives.
- Confirm NPI and payer profile data
- Load fee schedules before scheduling
- Track authorization rules by payer
- Test claims before first insured visit
2
Clinic or mobile-service readiness
Clinic and Mobile Setup
Ready space is the gate to day-one care. Clinic-based occupational therapy needs treatment rooms, accessibility, cleaning, furniture, and specialized equipment. Mobile care needs travel workflow, portable supplies, secure documentation, and safety protocols. The setup also changes by patient mix: pediatric sensory space, hand therapy tools, adult rehab gear, and geriatric visit workflows all affect launch speed and what can be booked first.
The spend is not small. Planned capex is $75,000 for build-out in Month 1 to Month 3, $40,000 for specialized equipment in Month 2 to Month 4, and $20,000 for furniture in Month 3 to Month 5. If any of those lag, you may have a leased space but still no safe, equipped, schedulable care.
Sequence the setup before booking visits
Match the setup to the service model first. Confirm which visit types you will open with, then buy only the room and tools needed for those cases. A pediatric-heavy launch needs different space and equipment than adult rehab or home visits. One clean rule: if a therapist cannot evaluate, treat, clean up, and document without improvising, the site is not open yet.
Test the full first-visit flow. Verify room turn time, storage, cleaning steps, travel routing, secure records, and safety checks before you take a single booking. Use the capex timing as a gate: build-out by Month 3, equipment by Month 4, furniture by Month 5. If the last item arrives late, your first revenue slips even if the lease is signed.
- Lock the first patient mix.
- Assign each tool to a service line.
- Test mobile safety and documentation.
- Confirm rooms can be scheduled.
3
EHR documentation and billing workflow
EHR and Billing Flow
An occupational therapy clinic can’t open cleanly unless the EHR workflow works before the first evaluation. That means scheduling, intake, consent, SOAP notes, care plans, authorization tracking, coding, claims submission, payment posting, denial follow-up, and HIPAA-secure records all have to connect on day one. The base run rate is $1,000 per month for the EHR, plus $700 per month for IT support and security, before billing service fees.
The real launch risk is treating patients before notes, codes, and claims are consistent. If the first evaluation can’t move from intake to claim, cash gets delayed and denials stack up. The Year 1 billing model assumes medical billing services at 50% of revenue, so weak workflow setup can hit both speed and margins. The readiness signal is simple: one test patient should move end to end without a break.
Test the full claim path
Before opening, map every handoff in writing and test it with a dummy patient. Confirm the schedule template, consent forms, documentation rules, authorization steps, coding fields, claim file, and payment posting all work together. If one step is manual or unclear, fix it before live visits start. That keeps the first week from turning into rework, missed charges, or claim rejections.
Assign one person to own the workflow and one to review the first claims. Use the test to prove the clinic can document the visit, bill it, and store it securely. If the test patient cannot reach claim submission without help, the business is not ready to take real patients yet.
- Run one test patient end to end
- Check authorization tracking early
- Verify claim submission fields
- Confirm denial follow-up steps
- Lock down HIPAA access controls
4
Referral pipeline and local demand
Referral pipeline and local demand
Referral flow is what turns a ready clinic into a live schedule. For occupational therapy, early volume usually comes from physicians, pediatricians, schools, hospitals, discharge planners, senior-care providers, attorneys, employers, community groups, and local search. If those partners are not lined up before opening, you can still launch on time, but you may open with empty slots and weak first-month treatment volume.
The practical risk is simple: a clean clinic with no booked evaluations burns cash fast. The model assumes marketing and patient acquisition at 30% of Year 1 revenue, so demand work has to start before day one. Readiness shows up as booked evaluation slots, named referral partners, intake scripts, and a follow-up cadence that keeps referrals moving.
Build demand before the doors open
Start with a referral list, then assign outreach by source. Confirm who sends what cases, what the intake ask is, and how fast your team follows up. Track each source in the CRM so you can see which channels fill evaluations and which ones stall.
Here’s the quick math: if demand ramps late, capacity stays underused even when the clinic is staffed and licensed. For launch, verify these inputs before opening day:
- Referral targets and contact names
- Local search setup and call routing
- Intake scripts and response times
- Weekly follow-up cadence
- Budget for patient acquisition
That sequence supports a faster ramp toward 60% Year 1 capacity and helps convert the first referrals into treatment visits instead of delayed starts.
5
Staffing and clinical capacity
Staffing and Clinical Capacity
Opening on time depends on having enough licensed therapists to cover evaluations, follow-ups, and documentation from day one. The staffing model lists a Clinic Director OT at $120,000, Senior Occupational Therapist at $90,000, Occupational Therapist at $75,000, plus admin, billing, and marketing support, so the clinic can’t just hire clinicians and hope the front office catches up.
The readiness signal is simple: coverage for intake, treatment, charting, and claims. If referrals arrive before staffing is balanced, wait times rise and cash gets stuck in billing. If admin support is thin, therapists spend time on scheduling and paperwork instead of visits, which lowers day-one capacity and can delay first revenue.
Match hires to visit volume
Before opening, map expected visits against each role’s load, supervision needs, and schedule. Here’s the quick check: if one gap exists in intake, billing, or documentation, clinical time leaks fast. Use the staffing plan to confirm who handles evaluations, who signs off on care plans, and who posts claims before the first patient is booked.
Test the full flow with one sample patient record: intake → evaluation → treatment note → billing → follow-up. The biggest launch risk is hiring ahead of referrals or underhiring admin support, because that creates payroll before volume and slows every step from scheduling to reimbursement.
- Confirm therapist coverage by visit type
- Assign billing before first claim
- Build admin support into day one
- Test documentation before opening
6
Related Products
- Occupational Therapy Porter's Five Forces Analysis
- Occupational Therapy BCG Matrix
- Occupational Therapy Business Model Canvas
- 7 Essential KPIs to Track for Occupational Therapy Growth
- Occupational Therapy Business Plan Template in Pre-Written Word
- 7 Strategies to Boost Occupational Therapy Clinic Profitability
- How to Calculate Monthly Running Costs for an Occupational Therapy Clinic?
- Occupational Therapy Startup Costs: $180K Opening Asset Plan
- Occupational Therapy Financial Model Template in Excel
- How Much Do Occupational Therapy Practice Owners Make? $98k Year 1 EBITDA
- How to Write an Occupational Therapy Business Plan: 7 Action Steps
- Occupational Therapy Marketing Mix
- Occupational Therapy Marketing Plan
- Occupational Therapy Business Proposal
- Occupational Therapy PESTEL Analysis
- Occupational Therapy Pitch Deck Example Editable PPTX
- Occupational Therapy Business SWOT Analysis
- Occupational Therapy Value Proposition Canvas
Frequently Asked Questions
Start by proving you can legally treat, document, bill, and fill the schedule Confirm state OT license status, form the business, obtain a National Provider Identifier, set up malpractice coverage, build HIPAA-ready workflows, and start payer credentialing Then match staffing to demand The model assumes 60% Year 1 capacity and about 462 monthly treatments when staffed to plan