 Owner income$120k+
Owner income$120k+How Much Do Occupational Therapy Practice Owners Make? $98k Year 1 EBITDA

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$120k+  Net margin10.5%–26.8%
Net margin10.5%–26.8% Revenue for target pay$1.1M
Revenue for target pay$1.1M Business difficultyHard
Business difficultyHard
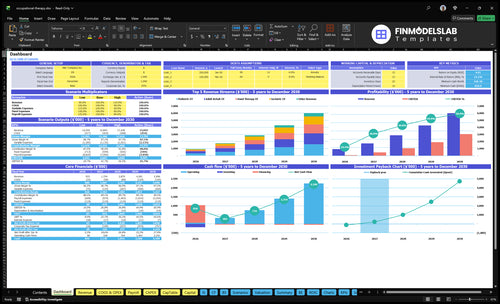


You’re planning owner income before the clinic has steady referrals, so the useful view is revenue minus payroll, overhead, reserves, and reinvestment This US occupational therapy practice model shows $933k Year 1 revenue, $98k Year 1 EBITDA, $470k Year 2 EBITDA, and a planned $120k clinic director salary
Owner income$120k+Net margin10.5%–26.8%Revenue for target pay$1.1MBusiness difficultyHardWant to test your OT owner income?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target owner pay.
Planning note: Research-based planning estimate only. Actual owner income depends on payer mix, no-shows, staffing, collections, taxes, and reserve policy. It is not guaranteed salary, tax advice, or owner distribution advice.
Want to check owner income in the Occupational Therapy financial model?
The dashboard in the Occupational Therapy Financial Model Template shows revenue, EBITDA, owner salary, cash need, payback, and visit volume. Open the model.
Owner-income model highlights
- Owner pay is shown
- Revenue and EBITDA tracked
- Scenarios test break-even timing
How much can a private occupational therapy practice owner pay themselves?
A private Occupational Therapy practice owner can pay themselves a $120k clinic director salary plus distributions only if cash allows. In Year 1, EBITDA is $98k, so the max pre-tax owner economics could reach $218k before debt, taxes, reserves, and reinvestment; watch demand through What Is The Current Growth Rate Of Client Engagement For Your Occupational Therapy Business? before taking extra cash out.
Owner Pay Math
- $120k annual clinic director salary
- $98k Year 1 EBITDA
- $218k max pre-tax owner economics
- Applies if owner fills that role
Distribution Guardrails
- $470k Year 2 EBITDA
- $1.754m Year 2 revenue
- Don’t drain working cash
- Month 2 needs $836k minimum cash
How many occupational therapy visits are needed to support owner income?
For Occupational Therapy, owner income starts with volume: Year 1 needs about 462 completed visits a month (about 107 a week) at roughly $168 collected per visit, and Year 2 rises to 829 a month (about 191 a week) at $176 per visit. Here’s the quick math: every extra 10 completed weekly visits at Year 1 pricing adds about $87k in annual collections before costs. Capacity starts at 60% and moves to 65% in Year 2, so cancellations and no-shows can cap income fast.
Year 1 volume
- 462 completed visits monthly
- 107 completed visits weekly
- About $168 collected per visit
- 60% starting capacity
Year 2 volume
- 829 completed visits monthly
- 191 completed visits weekly
- About $176 collected per visit
- 65% capacity, so no-shows matter
What profit margin can an occupational therapy practice make?
An Occupational Therapy practice can show a strong EBITDA margin, but treat it as a scenario, not a promise. For startup cost context, see How Much Does It Cost To Open, Start, Launch Your Occupational Therapy Business? In the model, Year 1 is 105% with $98k EBITDA on $933k revenue, and Year 2 is 268% with $470k on $1.754m. Margin gets better when therapist schedules fill and fixed overhead spreads over more visits.
Margin drivers
- 105% in Year 1
- 268% in Year 2
- More visits lift margin
- Fixed costs spread faster
Watch these costs
- Reimbursement rate pressure
- Therapist payroll and rent
- Documentation and billing costs
- Claim denials, supplies, marketing
Want the six OT income drivers?
1
107-191/wkVisit Volume
More billable visits lift collections fast and spread the fixed cost base, so every filled slot adds to owner take-home.
2
$168-$176Payer Mix
At $168-$176 collected per visit, better payer mix raises cash per session without adding more labor hours.
3
$528K-$819KLabor Productivity
Payroll grows from about $528K to $819K as staff scales, so tighter caseloads and scheduling protect margin.
4
60%-65%Fill Rate
At 60%-65% capacity, fewer cancellations and faster referrals keep therapists booked and avoid costly idle time.
5
$9.9K/moOverhead Control
Fixed overhead of about $9.9K a month stays steady, so rent, software, and admin waste flow straight through to profit.
6
$98K-$470KOwner Scale
With EBITDA rising from $98K to $470K later, the owner's pay depends on building a model that is not tied to every treatment hour.
Occupational Therapy Core Six Income Drivers
Billable visit volume
Billable Visit Volume
Completed visits are what turn care into cash, so they set the owner’s income ceiling. Year 1 is 462 visits per month, or 107 per week; Year 2 rises to 829 per month, or 191 per week. Use completed visits, not scheduled visits, because no-shows, cancellations, documentation time, and clinician availability cut paid volume.
Here’s the quick math: at the Year 1 average collection of $168 per completed visit, every 10 extra weekly visits adds about $87,360 a year before costs (10 × $168 × 52). At Year 1 volume, monthly collections are about $77,616 (462 × $168), so small attendance drops hit owner pay fast.
Track Completed Visits, Not Schedules
Measure the few inputs that move this driver: completed visits, cancellation and no-show rate, therapist availability, documentation time, and average collection per visit. If the schedule looks full but completed visits lag, the business is not earning its ceiling. A weekly completed-visit report is more useful than a booked-calendar report.
- Completed visits per therapist
- Same-week cancellation rate
- No-show rate by referral source
- Average collections per visit
- Open hours lost to documentation
Keep staffing and hiring tied to completed volume, not planned slots. When one extra therapist does not raise completed visits, payroll rises before revenue does. That is the real income risk here: weak attendance and slow documentation leave fixed costs in place while the owner’s draw stays capped.
1
Reimbursement and payer mix
Reimbursement and Payer Mix
This driver is the collections per completed visit. In planning terms, Year 1 runs from $100 for group programs to $200 for hand therapy, with a weighted average near $168 per visit; Year 2 rises to about $176. Mix matters because commercial, Medicare, Medicaid, workers’ compensation, school contracts, and cash-pay visits do not pay the same.
Here’s the quick math: if the payer mix shifts toward lower-paid visits, you need more completed visits to fund the same owner draw and fixed overhead. This is a planning estimate only, not a billing guarantee, and it should be modeled with completed visits, payer class, and average collection per visit.
Track Collections by Payer Class
Measure completed visits, not scheduled visits, and split collections by payer type each month. The key inputs are visit count, payer mix, price per service, and the weighted average collection per visit. If Medicaid or school-contract volume rises, check whether the lower rate is being offset by more visits or stronger capacity use.
Build forecasts from payer-specific averages, then test whether the schedule can still support owner pay after payroll and overhead. A simple rule: if the average per visit falls, the clinic needs either higher visit volume or a better mix to keep profit and cash flow steady.
2
Therapist labor productivity
Therapist Labor Productivity
Payroll is the biggest controllable cost after visit volume. This driver is the gap between collected revenue and total wage dollars, so the owner needs to watch completed visits per paid hour and collections per wage dollar. At $933k revenue against about $527k in Year 1 wages, collections are about 1.77x payroll; at $1.754m revenue and $819k wages in Year 2, that improves to about 2.14x. Empty schedules cut that fast.
Fill Paid Hours First
Track completed visits, not booked visits, plus therapist utilization, meaning paid hours that turn into billable care. Add staff only when the schedule can hold the extra load; otherwise wages rise before collections do, and margin shrinks. One clean check: if added clinicians do not lift collections per wage dollar, the hire is not paying for itself yet.
- Measure completed visits by clinician.
- Watch wage dollars per collected dollar.
- Fill calendars before adding headcount.
3
Referral flow and attendance
Referral Flow and Attendance
Referral flow only pays when an inquiry becomes a completed visit. At 60% capacity in Year 1, a 5-point gain to 65% adds about 39 more completed visits per month, or about $65k more monthly collections at $168 per visit. That extra cash drops into owner pay only after payroll, rent, and billing are covered.
Track referrals, scheduled visits, no-shows, and completed visits by source. Physician, pediatric, school, and rehab sources matter because they keep the schedule full; weak attendance makes payroll feel fixed, since staff cost stays put even when visits do not.
Measure the Visit Funnel
Use a simple funnel: referral → inquiry → scheduled visit → attended visit → completed visit. The owner should watch conversion by source, not just total leads, because a busy inbox does not pay the bills if visits are missed or canceled.
Set weekly targets for attendance rate and completed visits. If capacity moves from 60% to 65% in Year 1, collections can rise by about $65k a month at $168 per visit, so fast follow-up, reminder calls, and tight scheduling protect margin and owner draw.
- Track referrals by source.
- Count attended visits, not bookings.
- Review no-shows every week.
- Push the best referral channels.
4
Overhead control
Fixed Overhead Control
$99k per month in fixed overhead is the cost floor before payroll: rent, utilities, electronic health record software, liability insurance, cleaning, admin supplies, continuing education, and IT support. That equals $1.188m per year, so this driver decides how fast visit volume must grow just to protect owner pay.
Here’s the quick math: Year 1 revenue is $933k, so the fixed overhead base is larger than sales before clinician wages are paid. Overhead falls as a share of revenue only when completed visits rise and billing, credentialing, supplies, and admin support stay tight. If those slip, cash flow and owner draw get hit fast.
Track the cost base weekly
Measure overhead against completed visits, not scheduled visits. Watch the fixed lines and the variable lines together: 50% billing, 30% marketing, 20% therapeutic supplies, and 15% splint materials. If overhead grows faster than collections p er visit, the owner’s take-home income shrinks even when the schedule looks full.
- Review overhead by cost bucket monthly.
- Track visits, collections, and denial rate.
- Flag credentialing delays early.
- Control supply use and admin labor.
5
Owner role and scale model
Owner role and scale
Solo or mobile care keeps overhead light, but the owner’s treatment hours set the income ceiling. Outpatient and pediatric clinics can scale with hired OTs, assistants, admin support, and referral systems, lifting revenue from $933k in Year 1 to $1.754m in Year 2.
The tradeoff is cash and control: this scale path needs $836k minimum cash and about 18 months to pay back. Owner time shifts from treating to managing, so profit depends on whether added staff and referrals keep completed visits full.
Track capacity before you hire
Measure completed visits, not booked slots, plus therapist fill rate and admin load. If a new OT or assistant does not raise completed visits fast enough, payroll turns into fixed cost. The clean test is simple: grow only when referrals, attendance, and scheduling can support the next layer of staff.
6
Compare low, base, and high OT owner income scenarios
Owner income scenarios
Owner income scales with visit volume, collections, and staffing. The low, base, and high cases show a Year 1 ramp, a Year 2 staffed model, and a Year 3 upside case that still needs an EBITDA check.
| Scenario | Low CaseRamp-up | Base CaseStaffed growth | High CaseCash discipline |
|---|---|---|---|
| Launch model | This is a Year 1 ramp case with lower owner income while visits and collections are still building. | This is the modeled middle case with steadier owner income as staffing and volume normalize. | This is the stronger earnings path, but Year 3 EBITDA needs a fresh check before you turn it into owner income. |
| Typical setup | About 107 weekly visits, $168 average collections, and roughly $933k revenue before the clinic reaches fuller capacity. | About 191 weekly visits, $176 average collections, and roughly $1.754 million revenue with a fuller therapist team. | About 309 weekly visits and roughly $2.879 million revenue, with the margin line still needing validation from the source data. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $98kRamp-up case | $470kBase case | Upside pending EBITDA checkUpside case |
| Best fit | Use this to stress-test the clinic while staffing and referral flow are still uneven. | Use this as the main plan for a clinic running close to model capacity. | Use this only after confirming the Year 3 margin run-rate and payroll load. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Occupational Therapy Porter's Five Forces Analysis
- Occupational Therapy BCG Matrix
- Occupational Therapy Business Model Canvas
- 7 Essential KPIs to Track for Occupational Therapy Growth
- Occupational Therapy Business Plan Template in Pre-Written Word
- 7 Strategies to Boost Occupational Therapy Clinic Profitability
- How to Calculate Monthly Running Costs for an Occupational Therapy Clinic?
- Occupational Therapy Startup Costs: $180K Opening Asset Plan
- Occupational Therapy Financial Model Template in Excel
- How to Open an Occupational Therapy Practice in 3 to 6 Months
- How to Write an Occupational Therapy Business Plan: 7 Action Steps
- Occupational Therapy Marketing Mix
- Occupational Therapy Marketing Plan
- Occupational Therapy Business Proposal
- Occupational Therapy PESTEL Analysis
- Occupational Therapy Pitch Deck Example Editable PPTX
- Occupational Therapy Business SWOT Analysis
- Occupational Therapy Value Proposition Canvas
Frequently Asked Questions
This model shows a minimum cash need of $836k in Month 2, so the owner should plan cash before taking large distributions Startup capex totals $185k across build-out, equipment, furniture, IT, assessment tools, website, software setup, security, and marketing materials Payback is modeled at 18 months, which makes reserves part of owner-income planning