 Owner income$675k-$9.2M
Owner income$675k-$9.2MHow Much Oral Appliance Therapy Owners Can Make At $1185k Monthly Revenue

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Owner income$675k-$9.2M  Net margin48%-72%
Net margin48%-72% Revenue for target pay$1.4M
Revenue for target pay$1.4M Business difficultyMedium
Business difficultyMedium


Key Takeaways
- Completed cases drive revenue more than consultations.
- Collections timing shapes cash, not just profit.
- Capacity and delegation set the monthly ceiling.
- Overhead, billing delays, and reserves cut take-home.
Owner income$675k-$9.2MNet margin48%-72%Revenue for target pay$1.4MBusiness difficultyMediumWant to test your owner pay case volume?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only, not guaranteed salary, tax advice, or owner distribution advice. Excludes taxes, personal benefits, payer-specific promises, and clinical outcome assumptions.
Want to check owner income in the model?
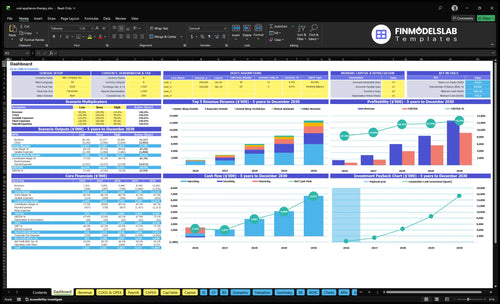
Open the Oral Appliance Therapy for Sleep Apnea Financial Model Template to see revenue, gross profit, operating profit, owner salary, and cash flow. It also shows Year 1 monthly revenue of $118,500 and Year 5 at $1,055,435.
Owner-income model highlights
- Owner take-home
- Revenue and margin
- COGS and fee scenarios
Is oral appliance therapy profitable as an add-on or standalone practice?
For Oral Appliance Therapy for Sleep Apnea, the add-on model is usually the faster path to profit because existing rent, staff, and patient relationships absorb part of the overhead. A standalone practice can scale much bigger, but it depends on dentist chair time, a clean billing workflow, and enough referral flow to keep the schedule full. Here’s the quick math: the supplied assumptions show monthly revenue rising from $118,500 in Year 1 to $1,055,435 in Year 5, but that growth also brings payroll, delegation risk, and claims timing pressure.
Add-on model
- Uses existing rent and staff
- Lowers startup overhead fast
- Fits current patient flow
- Needs tight billing cleanup
Standalone model
- Grows from 1 to 3 dentists
- Grows from 1 to 5 technicians
- Revenue scales to $1,055,435
- Raises payroll and referral risk
How many oral appliance cases per month to pay the owner?
For Oral Appliance Therapy for Sleep Apnea, there is no single monthly case target; use (fixed overhead + owner pay + reserves) ÷ contribution per case. At a $3,500 price, each senior dentist case contributes $2,712.50 before fixed overhead and payroll, so the $10,600 monthly overhead alone takes about 4 cases. Add staff wages, debt, reserves, and your target pay, and the real number moves up fast.
Case math
- $3,500 price per device
- $2,712.50 contribution per case
- $10,600 monthly fixed overhead
- 4 cases cover overhead only
Set the real target
- Include owner pay
- Add reserves for cash risk
- Include debt service
- Count staff wages too
How much can a dentist make from oral appliance therapy?
A dentist in How Much To Start Oral Appliance Therapy For Sleep Apnea Business? can show strong top-line revenue, but owner earnings are not the same as revenue. In the supplied Year 1 model, revenue is $142M, lead dentist salary is $210,000, and cash before unprovided wages, reserves, debt, and taxes is $764,850. The real take-home depends on case volume, payer mix, net collections, and how much overhead the practice assigns to this service.
Earnings View
- Separate revenue from owner pay
- Use $210,000 as dentist salary
- Treat $764,850 as pre-tax cash
- Reserve for wages, debt, taxes
Profit Drivers
- Add-on model can share overhead
- Dedicated model adds staffing load
- Payer mix changes net collections
- Case volume drives owner income
Want the six drivers behind owner take-home?
1
$118.5K/moCase Volume
Year 1 revenue runs at $118.5K a month, so every extra completed case lifts owner cash after clinical costs.
2
$3.5KNet Collections
Senior cases start at $3,500 and lower-priced support services pull the blend down, so pricing mix changes take-home fast.
3
65%Provider Capacity
The lead dentist runs at 65% of a 40-case plan in Year 1, so better delegation unlocks more revenue without a full cost reset.
4
14.5%Lab Costs
Lab fees and supplies start at 14.5% of revenue, and each point saved drops straight to EBITDA and owner distributions.
5
8.0%Referral Efficiency
Outreach and billing fees total 8.0% in Year 1, so tighter referral channels and cleaner claims keep more cash in the practice.
6
$10.6KOverhead Discipline
Fixed overhead is $10.6K a month, and loose billing or reserve builds can eat the cash left for owner draws.
Oral Appliance Therapy for Sleep Apnea Core Six Income Drivers
Completed Cases Per Month
Completed Cases Per Month
Completed cases drive owner pay more than consult volume because revenue only lands when a consult becomes a qualified start, then a fitting, a delivery, and a paid completed case. The supplied Year 1 senior dentist output is 40 monthly treatments at 650% capacity, or 26 revenue-producing cases. At $3,500 each, that is $91,000/month in case revenue.
The owner’s income depends on the conversion chain, not just demand. The supplied Year 1 role-based revenue is $118,500/month, but if consultations do not turn into delivered and collected appliances, that cash never reaches the practice. One weak step in the funnel can leave chair time busy and owner pay thin.
Track the Full Case Funnel
Measure the funnel weekly: consults, qualified starts, fittings, deliveries, and collected cases. Here’s the quick math: 26 collected cases × $3,500 = $91,000 in monthly case revenue, so a small drop in conversion hits cash fast. Track the gap between scheduled work and paid completions.
- Count delivered, not just scheduled.
- Track collected cases by provider.
- Review no-show and drop-off rates.
- Match staffing to case flow.
- Forecast cash from collected cases.
Use the same case definitions in sales, clinical, and billing. If consults are rising but completed cases are flat, the owner is buying activity, not income. Tie staffing, marketing, and collection reviews to paid completed cases, not raw consult volume.
1
Net Collections Per Oral Appliance Case
Net Collections Per Oral Appliance Case
Net collections per case is the cash you actually keep after cash pay, allowed amounts, patient responsibility, and payer adjustments. For this model, senior-dentist pricing rises from $3,500 in Year 1 to $3,900 in Year 5, while associate pricing rises from $3,300 in Year 2 to $3,600 in Year 5. If collections are slow or partial, profit can look fine on paper while cash for payroll and owner pay stays tight.
Track collected dollars per completed case, not just billed price, and separate cash pay from payer-backed cases. One clean rule: a case only helps owner income when it is collected, posted, and past the refund risk window. Avoid payer-specific promises until you know the allowed amount and the timing of patient payments.
Measure Collections by Collected Case
Build the forecast from price, payer mix, patient share, adjustment write-offs, and days to collect. That tells you whether a $3,500 case really acts like a $3,500 case, or less. If collections slip into later months, month-end revenue can still look healthy while cash on hand falls.
- Track cash collected per completed case
- Separate billed, allowed, and collected
- Watch days from delivery to payment
- Test senior and associate pricing separately
- Flag any partial or late collections
Use those numbers to set owner draw only after cash clears. That keeps income tied to real cash, not just posted revenue.
2
Lab, Device, And Clinical Delivery Cost
Lab and Delivery Cost Per Case
For each completed oral appliance case, direct cost sets gross margin. The supplied model shows COGS at 145% in Year 1, split between 120% lab fabrication and 25% clinical supplies, then improving to 121% by Year 5. On a $3,500 case, Year 1 gross profit is listed at $2,99250 before marketing, billing, overhead, payroll, and reserves.
That means owner pay depends on keeping cost and rework tied to completed cases, not just appointments. Remakes, adjustments, extra chair time, and follow-up visits can quietly eat margin, so one case that needs more lab work or more clinical time lowers cash flow even if revenue stays flat.
Track Cost by Completed Case
Measure lab fabrication, clinical supplies, and rework per completed case, then compare each case to the $3,500 price. The key question is simple: how much direct cost and chair time did each delivered appliance need before it was paid?
Use a case log with remakes, adjustments, extra visits, and collection timing. If one case needs repeated follow-up, its real gross profit drops fast, so tighten fit, document defects, and review the lab process before volume grows.
- Track cost per completed case
- Separate lab and clinic spend
- Count remakes and adjustments
- Log extra chair time
- Review follow-up visit frequency
3
Referral And Patient Acquisition Efficiency
Referral And Patient Acquisition Efficiency
Acquisition cost should be measured per accepted, collected case, not per lead. In Year 1, digital marketing and physician outreach can consume 50% of revenue, and medical billing and insurance processing adds another 30%, so 80% of revenue is already spoken for before fixed overhead and owner pay. Good leads that do not collect are expensive noise.
The inputs that matter are leads, consults, accepted starts, delivered appliances, collected cash, and source mix from physicians, sleep labs, dentists, hygiene patients, and local marketing. If conversion is weak, outreach spend turns into overhead, cash comes in late, and the owner’s draw gets squeezed even when case volume looks busy.
Track Conversion By Source, Not Just Spend
Measure cost per collected case by source and by step: lead to consult, consult to acceptance, acceptance to delivery, and delivery to collection. That tells you which channel actually funds profit. In Year 5, outreach falls to 30% of revenue and billing to 22%, or 52% total, so the business can keep more cash only if conversion improves.
- Cut low-converting sources fast.
- Track cash collected, not just starts.
- Follow each case to final payment.
- Watch delayed billing like a cost leak.
4
Provider Capacity And Delegation
Provider Capacity And Delegation
Capacity sets the ceiling on profitable case volume. Here, senior dentist capacity moves from 650% in Year 1 to 850% by Year 4 and Year 5, while associate dentist capacity starts at 550% in Year 2 and reaches 800% in Year 5. That matters because every completed case must pass through exams, scans, fittings, adjustments, documentation, billing handoffs, and admin follow-up.
If the owner keeps too much of that work, chair time gets trapped in low-value tasks and completed cases stall. If delegation is tight and clinical quality stays high, the practice can move more cases through the same day and turn more collected revenue into owner pay. Weak handoffs do the opposite: they create rework, delay billing, and cap profit.
Track Chair Time, Not Just Headcount
Measure capacity by completed cases per chair hour, not just by provi der count. Track which steps stay with the owner and which move to trained staff, then watch the time used on exams, scans, fittings, adjustments, documentation, billing handoffs, and admin follow-up. The goal is simple: keep the owner on the highest-value clinical steps only.
- Completed cases per month
- Owner chair hours per case
- Handoff delay days
- Remake and adjustment rates
- Collected revenue per provider hour
Test delegation one step at a time. Start with documentation, billing handoffs, and admin follow-up, then protect the clinical steps that affect fit and outcome. If owner chair load falls and case completion stays steady, the same staff base can support more revenue without raising overhead at the same rate.
5
Overhead, Billing, And Cash Reserves
Overhead, Billing, and Cash Reserves
For this practice, operating profit is not the same as owner pay. Fixed overhead is $10,600/month for rent, utilities, insurance, software, waste disposal, and admin, and Year 1 billing fees take 30% of revenue. If revenue is $91,000/month, billing fees are about $27,300, so overhead plus billing already uses $37,900/month before direct costs, debt service, and taxes.
That means cash can look fine on paper and still be tight in the bank. Denied or delayed claims, software, equipment, debt payments, and reserves all reduce distributable cash flow, so the owner should separate salary, profit, reserves, debt payments, and taxes before taking distributions.
Track Cash Before Owner Draws
Measure collected revenue, billing lag, and days cash on hand each month. If claims pay late, the practice can show profit but still miss rent, payroll, or equipment debt service. Keep a reserve bucket separate from operating cash so owner draws do not crowd out taxes or claim gaps.
- Track denied claims by dollar value.
- Review overhead against collected revenue.
- Set reserves before owner distributions.
- Separate debt service from profit.
6
Compare lean add-on, owner-operated, and expanded income scenarios
Owner income scenarios
Owner income moves with case volume, pricing, staffing, and overhead. The low, base, and high cases show what the practice can pay out before taxes, reserves, debt, and missing wage lines.
| Scenario | Low CaseLow Case | Base CaseBase Case | High CaseHigh Case |
|---|---|---|---|
| Launch model | This is the lean add-on path, with lower income from smaller case volume and lighter overhead. | This is the base operating case, using the Year 1 model and one lead dentist on the schedule. | This is the upside path, with higher income from fuller schedules and a larger provider team. |
| Typical setup | The practice runs with fewer completed cases, lower allocated overhead, and a smaller support stack than the model case. | Year 1 runs at about $118,500 monthly revenue, with 145% COGS, 80% variable fees, $10,600 fixed overhead, and a $210,000 lead dentist salary. | By Year 5, revenue reaches about $1,055,435 per month, with 121% COGS, 52% variable fees, 3 senior sleep dentists, 2 associate dentists, and larger support staff. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | Lower six figuresLow Case | $675kBase Case | $5.6m - $9.2mHigh Case |
| Best fit | Use this to test downside cash flow when patient flow starts slowly or stays choppy. | Use this as the core plan for budgeting, hiring, and lender talks. | Use this to test upside if referrals scale and the team keeps pace with demand. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Oral Appliance Therapy for Sleep Apnea Porter's Five Forces Analysis
- Oral Appliance Therapy for Sleep Apnea BCG Matrix
- Oral Appliance Therapy for Sleep Apnea Business Model Canvas
- What Are The 5 KPIs For Oral Appliance Therapy For Sleep Apnea Business?
- Oral Appliance Therapy Business Plan Template in Pre-Written Word
- How Increase Profits From Oral Appliance Therapy For Sleep Apnea?
- What Are The Operating Costs Of Oral Appliance Therapy?
- Oral Appliance Therapy Startup Costs: $35k Scanner Plus Runway
- Oral Appliance Therapy Financial Model Template in Excel
- How To Open An Oral Appliance Therapy Practice In 3-6 Months
- How To Write A Business Plan For Oral Appliance Therapy For Sleep Apnea?
- Oral Appliance Therapy for Sleep Apnea Marketing Mix
- Oral Appliance Therapy for Sleep Apnea Marketing Plan
- Oral Appliance Therapy for Sleep Apnea Business Proposal
- Oral Appliance Therapy for Sleep Apnea PESTEL Analysis
- Oral Appliance Therapy Pitch Deck Example Editable PPTX
- Oral Appliance Therapy for Sleep Apnea Business SWOT Analysis
- Oral Appliance Therapy for Sleep Apnea Value Proposition Canvas
Frequently Asked Questions
The supplied first-year model shows $118,500 in monthly revenue and $142M annually Listed COGS are 145%, variable marketing and billing fees are 80%, and fixed overhead is $10,600 per month After the $210,000 lead dentist salary, cash before unprovided staff wages, reserves, debt, and taxes is about $764,850